You might also like
- Medicine in Brief: Name the Disease in Haiku, Tanka and ArtFrom EverandMedicine in Brief: Name the Disease in Haiku, Tanka and ArtRating: 5 out of 5 stars5/5 (1)
- ARDS Respiratory Distress SyndromeDocument49 pagesARDS Respiratory Distress Syndromesonam yadav67% (3)
- Will The Real SMART Goals Please Stand Up?: Robert S. Rubin Saint Louis UniversityDocument2 pagesWill The Real SMART Goals Please Stand Up?: Robert S. Rubin Saint Louis UniversityKyoko TakayanagiNo ratings yet
- Operator Manual For Respons920 With ISE - v2016.02Document358 pagesOperator Manual For Respons920 With ISE - v2016.02Juan Pablo CondoriNo ratings yet
- F.E. Campbell - Sweet Slavery - HIT 139Document115 pagesF.E. Campbell - Sweet Slavery - HIT 139HokusLocus67% (3)
- Work Permit Renewal Application FormDocument2 pagesWork Permit Renewal Application FormyamojodnabNo ratings yet
- Respiratory Failure: by ArDocument39 pagesRespiratory Failure: by ArAleksei RomahovNo ratings yet
- Alka.S.Kandula Roll No: 6Document15 pagesAlka.S.Kandula Roll No: 6Raksha G GowdaNo ratings yet
- Acute Respiratory FailureDocument51 pagesAcute Respiratory Failureigorhorenko15No ratings yet
- ARFDocument50 pagesARFAme MehadiNo ratings yet
- Acute Respiratory Distress SyndromeDocument18 pagesAcute Respiratory Distress SyndromeJerinNo ratings yet
- ARDS Respiratory Distress Syndrome Diagnosis Treatment PrognosisDocument24 pagesARDS Respiratory Distress Syndrome Diagnosis Treatment PrognosisPooja ShashidharanNo ratings yet
- Acute Respiratory Failure (ARF): Causes, Symptoms and TreatmentDocument41 pagesAcute Respiratory Failure (ARF): Causes, Symptoms and TreatmentNozanin MahmadalievaNo ratings yet
- Understanding Respiratory FailureDocument134 pagesUnderstanding Respiratory FailureFirdaus AldyNo ratings yet
- Acute Respiratory Distress SyndromeDocument3 pagesAcute Respiratory Distress SyndromechoobiNo ratings yet
- Near Hanging: Professor Dr.S.Geetha'S UnitDocument24 pagesNear Hanging: Professor Dr.S.Geetha'S UnitJoshua JayakaranNo ratings yet
- Acute Respiratory Distress Syndrome (Ards) : Muamar Aldalaeen, RN, Mba, HCRM, Cic, Ipm, MSN, Phd. Haneen Alnuaimi, MSNDocument59 pagesAcute Respiratory Distress Syndrome (Ards) : Muamar Aldalaeen, RN, Mba, HCRM, Cic, Ipm, MSN, Phd. Haneen Alnuaimi, MSNAboodsha ShNo ratings yet
- Acute Respiratory Distress Syndrome (Ards) and Sepsis: Frans Abednego Barus Spesialis ParuDocument29 pagesAcute Respiratory Distress Syndrome (Ards) and Sepsis: Frans Abednego Barus Spesialis Paruarif qadhafyNo ratings yet
- Acute Respiratory Failure: Causes, Signs, TreatmentDocument6 pagesAcute Respiratory Failure: Causes, Signs, Treatmentniki estuNo ratings yet
- Blok KGD Pemicu 7Document93 pagesBlok KGD Pemicu 7LuzjrNo ratings yet
- Copd, Chronic Bronchitis, EmphysemaDocument28 pagesCopd, Chronic Bronchitis, EmphysemaHoney BoneyNo ratings yet
- Chronic Obstructive Lung Disease (COPD) : Is An Obstructive Lung Diseases in Which Irreversible Lung Damage Has OccuredDocument25 pagesChronic Obstructive Lung Disease (COPD) : Is An Obstructive Lung Diseases in Which Irreversible Lung Damage Has OccuredOmar AbdillahiNo ratings yet
- UNIT 5 RESPIRTATORY DISEASE NINJADocument18 pagesUNIT 5 RESPIRTATORY DISEASE NINJAronaronixstheboyNo ratings yet
- Standard Treatment Guidelines Medicine: (Respiratory Diseases)Document109 pagesStandard Treatment Guidelines Medicine: (Respiratory Diseases)Amiy ShamaNo ratings yet
- Acute Respiratory Distress SyndromeDocument20 pagesAcute Respiratory Distress SyndromeAngel Cauilan100% (1)
- Asthama & COPDDocument84 pagesAsthama & COPDAbdullah BhattiNo ratings yet
- Respiratory EMDocument51 pagesRespiratory EMMwalimu Hachalu FayeNo ratings yet
- Acute Respiratory Distress SyndromDocument19 pagesAcute Respiratory Distress SyndromTaqdees ManzoorNo ratings yet
- Acute Respiratory Distress SyndromeDocument17 pagesAcute Respiratory Distress SyndromeSherree Hayes100% (2)
- Respiratory FailureDocument21 pagesRespiratory FailureDennis MiritiNo ratings yet
- AssccDocument96 pagesAssccFirdaus AzinunNo ratings yet
- CHPT 70 Respiratory Part 2Document56 pagesCHPT 70 Respiratory Part 2helen brockNo ratings yet
- Respiratory DiseasesDocument9 pagesRespiratory Diseaseschristian pulmonesNo ratings yet
- Hypoxemia in ICU: Prepared by Hadi JazanDocument41 pagesHypoxemia in ICU: Prepared by Hadi JazanHadi JazanNo ratings yet
- Respiratory Failure (1) .Document36 pagesRespiratory Failure (1) .Ibrahim HemdanNo ratings yet
- C.O.P.D: (Chronic Obstructive Pulmonary Disorder)Document47 pagesC.O.P.D: (Chronic Obstructive Pulmonary Disorder)KrystelNo ratings yet
- DR - Donal Anjar Simanjuntak.M, Ked (Paru) .SP.PDocument15 pagesDR - Donal Anjar Simanjuntak.M, Ked (Paru) .SP.PM.Satria PerdanapNo ratings yet
- Acute Pulmonary FailureDocument15 pagesAcute Pulmonary FailureMariahnaSadjaluddinNo ratings yet
- Essential Guide to Oxygen TherapyDocument14 pagesEssential Guide to Oxygen TherapyUmdah HawatiNo ratings yet
- Classification of Respiratory FailureDocument8 pagesClassification of Respiratory Failurerau_rauNo ratings yet
- 48 Respiratory System Trauma - Dr. GreggDocument30 pages48 Respiratory System Trauma - Dr. GreggMinh Nguyễn Phương HồngNo ratings yet
- Acute Respiratory Failure LectureDocument53 pagesAcute Respiratory Failure Lectureprototypeallhell100% (2)
- NCM 112 LEC Topic 9 Respiratory Distress Syndrome RDSDocument4 pagesNCM 112 LEC Topic 9 Respiratory Distress Syndrome RDSViviene Faye FombuenaNo ratings yet
- Respiration 16 Respiratory FailureDocument31 pagesRespiration 16 Respiratory Failureapi-19641337No ratings yet
- Lo Tropmed 1Document49 pagesLo Tropmed 1belleNo ratings yet
- Hemothorax AND PneumoniaDocument43 pagesHemothorax AND Pneumoniaashoaib0313No ratings yet
- PulmonaryDocument3 pagesPulmonaryBaha'aeddin HammadNo ratings yet
- Pemicu 4: John Jordan 405140197Document149 pagesPemicu 4: John Jordan 405140197Dedy LeoNo ratings yet
- 5 Documents HealthDocument6 pages5 Documents HealthAbdiwali AhmedNo ratings yet
- Acute Respiratory Failure: R. Bhakialakshmi M.Sc. Nursing 2 Year PSG College of NursingDocument31 pagesAcute Respiratory Failure: R. Bhakialakshmi M.Sc. Nursing 2 Year PSG College of NursingassumptaNo ratings yet
- Pulmonary EdemaDocument10 pagesPulmonary EdemaMohammed EliasNo ratings yet
- Acute RFDocument7 pagesAcute RFLoren SangalangNo ratings yet
- Asthma, Pulmonary Edema, ARDS, Pulmonary EmbolismDocument16 pagesAsthma, Pulmonary Edema, ARDS, Pulmonary EmbolismKoRnflakesNo ratings yet
- Student Copy of COPD Lecture NotesDocument8 pagesStudent Copy of COPD Lecture NotesMary MarshNo ratings yet
- Respiratory FailureDocument39 pagesRespiratory FailureMuntasir BashirNo ratings yet
- Respiratory Failure: Dr. Sat Sharma Univ of ManitobaDocument38 pagesRespiratory Failure: Dr. Sat Sharma Univ of ManitobaGonzalo Venegas RojasNo ratings yet
- Acute Respiratory FailureDocument17 pagesAcute Respiratory FailurejulianajosNo ratings yet
- Group 1 6 Problem Emergency Medicine Block Monday, 30 Oct 2017Document121 pagesGroup 1 6 Problem Emergency Medicine Block Monday, 30 Oct 2017Jonathan TandajuNo ratings yet
- MonitoringDocument45 pagesMonitoringضبيان فرحانNo ratings yet
- Respiratory System Muamar Aldalaeen, RN, Mba, HCRM, Cic, Ipm, MSN, PHD - Haneen Alnuaimi, MSNDocument46 pagesRespiratory System Muamar Aldalaeen, RN, Mba, HCRM, Cic, Ipm, MSN, PHD - Haneen Alnuaimi, MSNAboodsha ShNo ratings yet
- Copd (Chronic Obstructive: Pulmonary Disease)Document68 pagesCopd (Chronic Obstructive: Pulmonary Disease)sinan kNo ratings yet
- 13.acute Respiratory FailureDocument34 pages13.acute Respiratory Failurekarim hassan100% (1)
- Acute Respiratory Distress SyndromeDocument18 pagesAcute Respiratory Distress SyndromeIrham TahkikNo ratings yet
- Asit Baz 2Document50 pagesAsit Baz 2Sarper Hikmet TAZENo ratings yet
- Mechanical VentilationDocument27 pagesMechanical VentilationMutaz DredeiNo ratings yet
- Pulmonary EmbolismDocument14 pagesPulmonary EmbolismMutaz Dredei100% (5)
- Chest TraumaDocument23 pagesChest TraumaMutaz DredeiNo ratings yet
- Acute Respiratory FailureDocument13 pagesAcute Respiratory FailureMutaz DredeiNo ratings yet
- Chemistry Units 8 12Document29 pagesChemistry Units 8 12reg speckNo ratings yet
- Apcosil 605Document1 pageApcosil 605rihtak123No ratings yet
- Fosfomycin: Review and Use Criteria BackgroundDocument12 pagesFosfomycin: Review and Use Criteria BackgroundAbu Azzam Al-Hadi100% (1)
- Water For Injections BP: What Is in This Leaflet?Document2 pagesWater For Injections BP: What Is in This Leaflet?Mohamed OmerNo ratings yet
- Girl Scouts ActivitiesDocument5 pagesGirl Scouts ActivitiessluttybitchNo ratings yet
- Experiment 1 Marble Race Virtual Science Lab Chem 2Document4 pagesExperiment 1 Marble Race Virtual Science Lab Chem 2Oribe, Narciso A.100% (1)
- Glover 6e - Chapter 02Document41 pagesGlover 6e - Chapter 02JIGNESH DESAINo ratings yet
- 01 Well Head ComponentsDocument46 pages01 Well Head ComponentsKhanh Pham Minh100% (7)
- Master Key Bonus - The Healing CodeDocument8 pagesMaster Key Bonus - The Healing CodeChanterelle Vasto100% (12)
- Psychedelic Drugs-A New Era in Psychiatry?Document9 pagesPsychedelic Drugs-A New Era in Psychiatry?PeterNo ratings yet
- Ishrae 365 2009 PDFDocument16 pagesIshrae 365 2009 PDFZeeshan HasanNo ratings yet
- 6-Step Guide to Crushing Imposter SyndromeDocument10 pages6-Step Guide to Crushing Imposter SyndromeMark KestNo ratings yet
- Pathology AIIMSDocument26 pagesPathology AIIMSvkNo ratings yet
- PackageCare Maintenance ChecklistDocument1 pagePackageCare Maintenance ChecklistBùi ViệtNo ratings yet
- LV CB Catalogue PDFDocument260 pagesLV CB Catalogue PDFBoobesh Kumar SekarNo ratings yet
- Project Execution ProcedureDocument4 pagesProject Execution Procedurecyno2167% (3)
- Rational Choice TheoryDocument6 pagesRational Choice TheoryMaria Theresa HerbolingoNo ratings yet
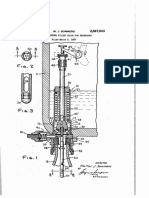
- Counter-pressure filler valve for beveragesDocument3 pagesCounter-pressure filler valve for beveragesbimalishaNo ratings yet
- Trangia Worksheet IntroDocument2 pagesTrangia Worksheet Introjames.mccooeyNo ratings yet
- Polythionic Acid Stress Corrosion CrackingDocument2 pagesPolythionic Acid Stress Corrosion CrackingVajid MadathilNo ratings yet
- Economic Case for Immobilizing EnzymesDocument25 pagesEconomic Case for Immobilizing EnzymesNikki ChauhanNo ratings yet
- Make Every Day Count: George Eliot's inspirational poemDocument3 pagesMake Every Day Count: George Eliot's inspirational poemRUTUJA KALENo ratings yet
- Fuente As-IDocument4 pagesFuente As-IadalaviNo ratings yet
- DL420 15c SpecificationsDocument4 pagesDL420 15c Specificationsesteban muñozNo ratings yet
- PricelistDocument184 pagesPricelistWissam JarmakNo ratings yet
- Halal Policy PDFDocument1 pageHalal Policy PDFSaid SaidiNo ratings yet