You might also like
- The OCD Workbook - Your Guide To Breaking Free From Obsessive-Compulsive Disorder (PDFDrive)Document378 pagesThe OCD Workbook - Your Guide To Breaking Free From Obsessive-Compulsive Disorder (PDFDrive)MrRamm100% (8)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Group 2 Bipolar DisorderDocument22 pagesGroup 2 Bipolar DisorderSolsona Natl HS MaanantengNo ratings yet
- Nursing Exam Cram Sheet For The NCLEX-RN: 1. Test Information 5. ABG ValuesDocument8 pagesNursing Exam Cram Sheet For The NCLEX-RN: 1. Test Information 5. ABG ValuesManuela GutiérrezNo ratings yet
- NeurologyDocument119 pagesNeurologyAhmad MakhloufNo ratings yet
- Arnica The Miracle Remedy - Case Records - HomeopathyandmoreDocument23 pagesArnica The Miracle Remedy - Case Records - HomeopathyandmoreAshna100% (1)
- OBGYN Form 4 Take VersionDocument60 pagesOBGYN Form 4 Take VersionValentina BustamanteNo ratings yet
- Heterophoria: University of Gondar Department of Optometry by Nebiyat FelekeDocument27 pagesHeterophoria: University of Gondar Department of Optometry by Nebiyat Felekehenok biruk100% (1)
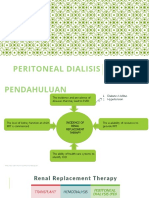
- DT Peritoneal Dialysis DektaDocument21 pagesDT Peritoneal Dialysis Dektailham nugrohoNo ratings yet
- Advanced Glauc ManagmentDocument49 pagesAdvanced Glauc Managmenthenok birukNo ratings yet
- Pre and Post Op Cataract EvaluaDocument56 pagesPre and Post Op Cataract Evaluahenok birukNo ratings yet
- Research Article: Diabetic Retinopathy in Native and Nonnative CanadiansDocument6 pagesResearch Article: Diabetic Retinopathy in Native and Nonnative Canadianshenok birukNo ratings yet
- Retinopati Diabetik PDFDocument4 pagesRetinopati Diabetik PDFaulNo ratings yet
- Proposal Defence Presentation Template: Iph, UogDocument16 pagesProposal Defence Presentation Template: Iph, Uoghenok birukNo ratings yet
- CLV, VF Assessment 2021Document133 pagesCLV, VF Assessment 2021henok birukNo ratings yet
- L2 Optical LV AidsDocument34 pagesL2 Optical LV Aidshenok birukNo ratings yet
- Clinical LV-Visual Impairment 2021Document60 pagesClinical LV-Visual Impairment 2021henok birukNo ratings yet
- Project ManagementDocument64 pagesProject Managementhenok birukNo ratings yet
- Chapter 4 Introduction To ProbabilityDocument68 pagesChapter 4 Introduction To ProbabilityG Gጂጂ TubeNo ratings yet
- Over View of Management For Optometry by ChalieDocument53 pagesOver View of Management For Optometry by Chaliehenok birukNo ratings yet
- Resource ManagementDocument90 pagesResource Managementhenok birukNo ratings yet
- ICRS Implantation Effectiveness for Keratoconus TreatmentDocument25 pagesICRS Implantation Effectiveness for Keratoconus Treatmenthenok birukNo ratings yet
- L3 TelescopeDocument51 pagesL3 Telescopehenok birukNo ratings yet
- University of Gondar Estimation and Hypothesis TestingDocument119 pagesUniversity of Gondar Estimation and Hypothesis Testinghenok birukNo ratings yet
- University of Gondar College of Medicine and Health Science Department of Epidemiology and BiostatisticsDocument34 pagesUniversity of Gondar College of Medicine and Health Science Department of Epidemiology and Biostatisticshenok birukNo ratings yet
- CLV, VF Assessment 2021Document133 pagesCLV, VF Assessment 2021henok birukNo ratings yet
- AR Implantable Collamer Lens - HundumaDocument22 pagesAR Implantable Collamer Lens - Hundumahenok birukNo ratings yet
- Childhood Glaucoma NewDocument30 pagesChildhood Glaucoma Newhenok birukNo ratings yet
- AR Refractive Surgery-KalkidanDocument47 pagesAR Refractive Surgery-Kalkidanhenok birukNo ratings yet
- Chapter 2 Method of Data Collection andDocument59 pagesChapter 2 Method of Data Collection andG Gጂጂ TubeNo ratings yet
- AR Multifocal Orthok Vs Conventional in Mypoia Control-DessieDocument37 pagesAR Multifocal Orthok Vs Conventional in Mypoia Control-Dessiehenok birukNo ratings yet
- Chapter 1 IntroductionDocument30 pagesChapter 1 Introductionhenok birukNo ratings yet
- ARContact Lens For Keratoconus - AmsaluDocument44 pagesARContact Lens For Keratoconus - Amsaluhenok birukNo ratings yet
- AR Therapeutic CL - YohanisDocument35 pagesAR Therapeutic CL - Yohanishenok birukNo ratings yet
- AR On SCCL For Adv. KCs-MeketeDocument24 pagesAR On SCCL For Adv. KCs-Meketehenok birukNo ratings yet
- A) Definition of Fusional ReservesDocument26 pagesA) Definition of Fusional Reserveshenok birukNo ratings yet
- AR Sort Term Corneal Change-ZufanDocument31 pagesAR Sort Term Corneal Change-Zufanhenok birukNo ratings yet
- AR Visual Performance BN DT CLs in KCs-BesufekadDocument19 pagesAR Visual Performance BN DT CLs in KCs-Besufekadhenok birukNo ratings yet
- CGN Pediatric 1 Lesson 2Document20 pagesCGN Pediatric 1 Lesson 2okumu atanasNo ratings yet
- Other PoisionDocument6 pagesOther PoisionNitya SharmaNo ratings yet
- Anemia Aplastik (Pansitopenia), Rahmad Aswin JuliansyahDocument34 pagesAnemia Aplastik (Pansitopenia), Rahmad Aswin Juliansyahpopi lestariNo ratings yet
- Prevention Practice For Neuromuscular Conditions PresentationDocument22 pagesPrevention Practice For Neuromuscular Conditions PresentationShimmering MoonNo ratings yet
- Chronic Kidney Disease: A. Pathophysiology A. Schematic DiagramDocument3 pagesChronic Kidney Disease: A. Pathophysiology A. Schematic DiagramDaniel GeduquioNo ratings yet
- Unit - 2nd-WPS Office-1Document8 pagesUnit - 2nd-WPS Office-1Suneel Kumar PrajapatiNo ratings yet
- Depictions of Mental Health Topics in Malayalam CinemaDocument8 pagesDepictions of Mental Health Topics in Malayalam Cinemagion.nandNo ratings yet
- Burger Allen Exercises pdf1Document133 pagesBurger Allen Exercises pdf1lucky 116No ratings yet
- Assessing The Prevalence of Diabetes Within The Sunyani Municipality. A Case of The Sunyani Regional HospitalDocument9 pagesAssessing The Prevalence of Diabetes Within The Sunyani Municipality. A Case of The Sunyani Regional HospitalIJMSIR JOURNALNo ratings yet
- Assessing Frequency of Migraine It's Associated Factors Among The Undergraduate Students of Gajju Khan Medical College, SwabiDocument46 pagesAssessing Frequency of Migraine It's Associated Factors Among The Undergraduate Students of Gajju Khan Medical College, Swabiammar hussain darNo ratings yet
- Case StudyDocument10 pagesCase StudyARABELLA FUNDARNo ratings yet
- Allied Health Council Examination QuestionsDocument39 pagesAllied Health Council Examination QuestionsSAMMYNo ratings yet
- Advice For People With MSDocument10 pagesAdvice For People With MSAsma Al-MahmoudNo ratings yet
- 4-Hyperplasia Part 2-1Document48 pages4-Hyperplasia Part 2-1Ali GamalNo ratings yet
- Boger's Synoptic Materia Medica KeyDocument3 pagesBoger's Synoptic Materia Medica KeySony AngaraNo ratings yet
- Viral Hepatitis Case Semi FinalDocument73 pagesViral Hepatitis Case Semi FinalLOIS DANIELLE REYESNo ratings yet
- Pregnancy Induced HypertensionDocument4 pagesPregnancy Induced HypertensionFatmah Sarah CornellNo ratings yet
- A Death Struck YearDocument42 pagesA Death Struck Yearapi-543810353No ratings yet
- Chest X-ray, Echo, CBC, Electrolytes for HF DiagnosisDocument2 pagesChest X-ray, Echo, CBC, Electrolytes for HF DiagnosisJeno Luis J. ACUBNo ratings yet
- BR J Haematol - 2022 - Shaulov - Early Integration of Palliative Care For Patients With Haematological MalignanciesDocument17 pagesBR J Haematol - 2022 - Shaulov - Early Integration of Palliative Care For Patients With Haematological MalignanciesCarlosGonalv2014No ratings yet
- Doctor on Call preview-1Document58 pagesDoctor on Call preview-1Fourth YearNo ratings yet
- Nasal Polyp Homeopathic Case ReportDocument35 pagesNasal Polyp Homeopathic Case ReportRahul PandeyNo ratings yet
- Thyroid and Parathyroid Disorders: by Dr. Magdi Awad Sasi 2013Document65 pagesThyroid and Parathyroid Disorders: by Dr. Magdi Awad Sasi 2013Eidi IdhamNo ratings yet