You might also like
- Food Protein Induced Enterocolitis (FPIES): Diagnosis and ManagementFrom EverandFood Protein Induced Enterocolitis (FPIES): Diagnosis and ManagementTerri Faye Brown-WhitehornNo ratings yet
- In the Shadow of Illness: Parents and Siblings of the Chronically Ill ChildFrom EverandIn the Shadow of Illness: Parents and Siblings of the Chronically Ill ChildNo ratings yet
- Case StudyDocument111 pagesCase StudyBrian OballoNo ratings yet
- Community Acquired Pneumonia Case StudyDocument14 pagesCommunity Acquired Pneumonia Case StudycenakatokNo ratings yet
- Acute Tonsillar Pharyngitis Case StudyDocument39 pagesAcute Tonsillar Pharyngitis Case Studyirish felixNo ratings yet
- Case Study PneumoniaDocument45 pagesCase Study PneumoniaYashoda Satpute83% (6)
- EBR1 PediaDocument3 pagesEBR1 PediaNovah LadromaNo ratings yet
- Pneumonia Case PresentationDocument102 pagesPneumonia Case PresentationRegineCuasSulibNo ratings yet
- Case Study of BronchoPneumoniaDocument64 pagesCase Study of BronchoPneumoniaJomari Zapanta100% (2)
- Pleural EffusionDocument38 pagesPleural EffusionMela VincoNo ratings yet
- Case Study On Dengue FeverDocument76 pagesCase Study On Dengue FeverMary Rose Silva Gargar0% (1)
- Pediatric Pneumonia Case StudyDocument44 pagesPediatric Pneumonia Case StudyPreiane PayladoNo ratings yet
- PCAP-c Group A NiggasDocument39 pagesPCAP-c Group A NiggasJenny YenNo ratings yet
- Case Study - PneumoniaDocument41 pagesCase Study - PneumoniaCaleb Mcmahon67% (6)
- Spinal TuberculosisDocument46 pagesSpinal TuberculosisAbby Austero100% (1)
- Pediatric Ward Journal Binwag BSN 2aDocument2 pagesPediatric Ward Journal Binwag BSN 2aVincentus BinNo ratings yet
- Case Study SepsisDocument44 pagesCase Study Sepsisnursedale100% (4)
- A Case Study On Pneumonia: Angeles University Foundation Angeles City College of NursingDocument80 pagesA Case Study On Pneumonia: Angeles University Foundation Angeles City College of Nursingmaria_cordero_19No ratings yet
- GRP 20 Final Abscess Case StudyDocument14 pagesGRP 20 Final Abscess Case StudyBorja, Kimberly GraceNo ratings yet
- Chapter I - Case Background and AssessmentDocument21 pagesChapter I - Case Background and AssessmentJuhainie Dipatuan MagundacanNo ratings yet
- Pneumonia Case Study of a 4-Month Old BabyDocument41 pagesPneumonia Case Study of a 4-Month Old BabyTrixNo ratings yet
- Pneumonia Case Pres Level 2 Group 4Document43 pagesPneumonia Case Pres Level 2 Group 4Archie Punzalan67% (3)
- The Body FinalDocument61 pagesThe Body FinalMhargie RomanillosNo ratings yet
- ZNJ - Volume 17 - Issue 2 - Pages 1-13Document13 pagesZNJ - Volume 17 - Issue 2 - Pages 1-13Ljc JaslinNo ratings yet
- Edit NG Drug StudyDocument35 pagesEdit NG Drug StudyAlleinad BarracasNo ratings yet
- SURIGAO EDUCATION CENTER pcapcDocument9 pagesSURIGAO EDUCATION CENTER pcapckholeensendrienesheensNo ratings yet
- Case Analysis Group 9 MeaslesDocument19 pagesCase Analysis Group 9 MeaslesJob Arden EstepaNo ratings yet
- PCAP CDocument42 pagesPCAP CJenny YenNo ratings yet
- Pneumonia Clinical Case Study BSN 2 2 Group 4Document43 pagesPneumonia Clinical Case Study BSN 2 2 Group 4Precious Jenichris TamayoNo ratings yet
- INTRODUCTIONDocument8 pagesINTRODUCTIONmalindaNo ratings yet
- Case Study-Tb MeningitisDocument41 pagesCase Study-Tb Meningitislhan alvin83% (6)
- ETO NA TALAGA - Tapos Na Ang Lahat !!!Document32 pagesETO NA TALAGA - Tapos Na Ang Lahat !!!Keenen Engel Bonifacio Pascua100% (1)
- Pcap MRDocument31 pagesPcap MRClark SavageNo ratings yet
- Clinical PaperDocument18 pagesClinical PaperlhhjklllNo ratings yet
- Pediatric Community Acquired Pneumonia (PCAP)Document24 pagesPediatric Community Acquired Pneumonia (PCAP)deejayseroje93% (28)
- Case Pres-PcghDocument48 pagesCase Pres-PcghAlcala TayoNo ratings yet
- Acute Bronchitis... The OneDocument35 pagesAcute Bronchitis... The One'mYk FavilaNo ratings yet
- Case Study PN Pcap C FinalDocument50 pagesCase Study PN Pcap C FinalKimberly Milaran0% (2)
- Case Report Neurology DivisionDocument82 pagesCase Report Neurology DivisionOlgHaENo ratings yet
- Intraauricular AbscessDocument15 pagesIntraauricular AbscessromaNo ratings yet
- Nursing care for a child with miliary tuberculosisDocument28 pagesNursing care for a child with miliary tuberculosisNicole Angela Concepcion100% (2)
- Juvenile Idiopathic Oligoarthritis Case ReportDocument32 pagesJuvenile Idiopathic Oligoarthritis Case ReportMuhammad Rifani KnNo ratings yet
- Ajol File Journals - 494 - Articles - 112516 - Submission - Proof - 112516 5833 312396 1 10 20150204Document6 pagesAjol File Journals - 494 - Articles - 112516 - Submission - Proof - 112516 5833 312396 1 10 20150204ASK De OliveiraNo ratings yet
- Fernandez, Case StudyDocument17 pagesFernandez, Case StudyrhenzmonfielNo ratings yet
- 172-1610189659-Case ReportDocument5 pages172-1610189659-Case ReportBojan IlievNo ratings yet
- Impact of Childhood Asthma On Children and Mothers Exploring The Sri Lankan SituationDocument6 pagesImpact of Childhood Asthma On Children and Mothers Exploring The Sri Lankan SituationInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Bronchiolitis ScriptDocument6 pagesBronchiolitis ScriptAhmed RmelahNo ratings yet
- Nursing Case Study on Pulmonary TuberculosisDocument36 pagesNursing Case Study on Pulmonary TuberculosisJek Dela CruzNo ratings yet
- Case Presentation Calalang General Hospital: Far Eastern University Institute of Nursing Summer 2009Document15 pagesCase Presentation Calalang General Hospital: Far Eastern University Institute of Nursing Summer 2009Bianca de GuzmanNo ratings yet
- Acute BronchitisDocument108 pagesAcute Bronchitisemofreo100% (1)
- Community Acquired PneumoniaDocument43 pagesCommunity Acquired PneumoniaJeco ValdezNo ratings yet
- Febrile SeizureDocument27 pagesFebrile Seizuremanu_gutierrez08No ratings yet
- Grand CP PowerpntDocument96 pagesGrand CP PowerpntDatu Puti MangelenNo ratings yet
- Case Study Pleural EffusionDocument32 pagesCase Study Pleural Effusionwguino100% (1)
- CS - PPDocument48 pagesCS - PPNicole ArandingNo ratings yet
- Case Study Bronchial Asthma - GROUP 2Document59 pagesCase Study Bronchial Asthma - GROUP 2Jimlord GarciaNo ratings yet
- Respiratory-Pneumonia Casebook CCCDocument59 pagesRespiratory-Pneumonia Casebook CCCFrancis Adrian100% (1)
- The Weight of Online Learning on a Nursing Student's HealthDocument48 pagesThe Weight of Online Learning on a Nursing Student's HealthAnn Nicole UlitNo ratings yet
- Case Presentation Calalang General Hospital: Far Eastern University Institute of Nursing Summer 2009Document13 pagesCase Presentation Calalang General Hospital: Far Eastern University Institute of Nursing Summer 2009Bianca de GuzmanNo ratings yet
- Dengue Case StudyDocument20 pagesDengue Case Studyjohn jumborockNo ratings yet
- Solanio SlidesCarnivalDocument29 pagesSolanio SlidesCarnivalAlexandra Mae D. MiguelNo ratings yet
- Pneumonia Pathophysiology (Book Based) : Non-Modifiable: ModifiableDocument2 pagesPneumonia Pathophysiology (Book Based) : Non-Modifiable: ModifiableYVETTE CLAIRE BORRESNo ratings yet
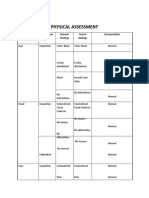
- Physical Assessment: Organ/ System Technique Normal Findings Actual Findings InterpretationDocument12 pagesPhysical Assessment: Organ/ System Technique Normal Findings Actual Findings InterpretationYVETTE CLAIRE BORRESNo ratings yet
- Rynaldo SlidesCarnivalDocument31 pagesRynaldo SlidesCarnivalRey VelasNo ratings yet
- Pneumonia Pathophysiology (Patient Based) : Non-Modifiable: ModifiableDocument2 pagesPneumonia Pathophysiology (Patient Based) : Non-Modifiable: ModifiableYVETTE CLAIRE BORRESNo ratings yet
- Homocystinuria Diagnosis and Imaging FindingsDocument5 pagesHomocystinuria Diagnosis and Imaging FindingsYVETTE CLAIRE BORRESNo ratings yet
- In Uence of Learning StylesDocument21 pagesIn Uence of Learning StylesYVETTE CLAIRE BORRESNo ratings yet
- Chemotherapy and YouDocument60 pagesChemotherapy and YouYVETTE CLAIRE BORRESNo ratings yet
- OXYTOCIN DRUG STUDYDocument4 pagesOXYTOCIN DRUG STUDYYVETTE CLAIRE BORRESNo ratings yet
- AuthorsDocument42 pagesAuthorsYVETTE CLAIRE BORRESNo ratings yet
- Subjective Cues Long Term Objective Independent: Independent: Long Term: Goal MetDocument3 pagesSubjective Cues Long Term Objective Independent: Independent: Long Term: Goal MetYVETTE CLAIRE BORRESNo ratings yet
- Nursing care plan template for studentsDocument2 pagesNursing care plan template for studentsYVETTE CLAIRE BORRESNo ratings yet
- Journal Critiquing Article Reviewed:: Submitted To: Prof. Cynthia A. Umila, RN, MAN Submitted By: Yvette Claire L. BorresDocument6 pagesJournal Critiquing Article Reviewed:: Submitted To: Prof. Cynthia A. Umila, RN, MAN Submitted By: Yvette Claire L. BorresYVETTE CLAIRE BORRESNo ratings yet
- CPP - Oropharyngeal Airway InsertionDocument3 pagesCPP - Oropharyngeal Airway InsertionYVETTE CLAIRE BORRESNo ratings yet
- Understanding Undifferentiated SchizophreniaDocument48 pagesUnderstanding Undifferentiated SchizophreniaYVETTE CLAIRE BORRESNo ratings yet
- HOPE Approach to Assessing Spiritual Resources and Effects on CareDocument1 pageHOPE Approach to Assessing Spiritual Resources and Effects on CareYVETTE CLAIRE BORRESNo ratings yet
- PET Therapy II PDFDocument7 pagesPET Therapy II PDFYVETTE CLAIRE BORRESNo ratings yet
- JC NCM 2ND SemDocument5 pagesJC NCM 2ND SemYVETTE CLAIRE BORRESNo ratings yet
- JC NCM HBLNM Article PDFDocument15 pagesJC NCM HBLNM Article PDFYVETTE CLAIRE BORRESNo ratings yet
- JC Duty DRDocument2 pagesJC Duty DRYVETTE CLAIRE BORRESNo ratings yet
- Case Study BipolarDocument22 pagesCase Study BipolarRobert de Guzman Jr.93% (29)
- Journal Critique in Health Education: Submitted By: Borres, Yvette Claire, LDocument7 pagesJournal Critique in Health Education: Submitted By: Borres, Yvette Claire, LYVETTE CLAIRE BORRESNo ratings yet
- Case StudyDocument8 pagesCase StudyAmberlynn Stolarski100% (2)
- Pathophysiology GyneDocument2 pagesPathophysiology GyneYVETTE CLAIRE BORRESNo ratings yet
- Journal Critique in Health Education: Submitted By: Borres, Yvette Claire, LDocument7 pagesJournal Critique in Health Education: Submitted By: Borres, Yvette Claire, LYVETTE CLAIRE BORRESNo ratings yet
- Homocystinuria: Diagnosis and Neuroimaging Findings of Iranian Pediatric PatientsDocument7 pagesHomocystinuria: Diagnosis and Neuroimaging Findings of Iranian Pediatric PatientsYVETTE CLAIRE BORRESNo ratings yet
- GYNECOLOGICALDocument255 pagesGYNECOLOGICALTaco BellNo ratings yet
- JCHE Final 2Document9 pagesJCHE Final 2YVETTE CLAIRE BORRESNo ratings yet
- INTERACTIVE LECTURE FloresDocument7 pagesINTERACTIVE LECTURE FloresYVETTE CLAIRE BORRESNo ratings yet
- Drug Study On PpudDocument3 pagesDrug Study On PpudLezelle Mandane CardinoNo ratings yet
- Ice TherapyDocument5 pagesIce TherapyDiane CastillonNo ratings yet
- Case Study Endometrial PDFDocument17 pagesCase Study Endometrial PDFapi-279886264No ratings yet
- How to use an incentive spirometer for COPDDocument19 pagesHow to use an incentive spirometer for COPDKoleen KirstenNo ratings yet
- Hypoparathyroidism Review of The Literature 2018 PDFDocument7 pagesHypoparathyroidism Review of The Literature 2018 PDFsajmirNo ratings yet
- BPJS Coding IcdDocument4 pagesBPJS Coding IcdDewi Agustina100% (1)
- Liver CancerDocument233 pagesLiver CancerandikhgNo ratings yet
- Newborn Head Appearance and FeaturesDocument2 pagesNewborn Head Appearance and FeaturesAdiel CalsaNo ratings yet
- Rated Review ExamplesDocument41 pagesRated Review ExamplesMaria AspriNo ratings yet
- CVA Case StudyDocument9 pagesCVA Case Studypylzanne100% (1)
- From Chronic To Critical: A Latino Family Confronts End-of-Life DecisionsDocument2 pagesFrom Chronic To Critical: A Latino Family Confronts End-of-Life DecisionsRoyKimNo ratings yet
- Analgesics in SingaporeDocument10 pagesAnalgesics in SingaporePhua Wei TingNo ratings yet
- 2020 Крок Англ 1-деньDocument4 pages2020 Крок Англ 1-деньPrince NathanNo ratings yet
- Daepoch Protocolo BccancerDocument9 pagesDaepoch Protocolo BccancerLuiz MeloNo ratings yet
- Wound Healing, Tissue Repair, and FibrosisDocument28 pagesWound Healing, Tissue Repair, and FibrosisRibka Theodora100% (1)
- Urethral Trauma - Injuries Poisoning - MSD Manual Professional EditionDocument2 pagesUrethral Trauma - Injuries Poisoning - MSD Manual Professional EditionNaufal NaswanNo ratings yet
- Monthlyshot December 1Document10 pagesMonthlyshot December 1api-308247685No ratings yet
- BLS MCQDocument22 pagesBLS MCQGeraldine Augusta100% (1)
- CDS - MMS Protocols A-Z - Yummy - Doctor Holistic Health EducationDocument23 pagesCDS - MMS Protocols A-Z - Yummy - Doctor Holistic Health Educationbagus918No ratings yet
- Parenteral NutritionDocument6 pagesParenteral NutritionAngela NeriNo ratings yet
- NHM Letter World Diabetes DayDocument9 pagesNHM Letter World Diabetes DayAnonymous RCDcVGlFpzNo ratings yet
- OrthodonticDocument3 pagesOrthodonticFirma Nurdinia DewiNo ratings yet
- PDF 0OIutGciNYy1qLCkgEMFDocument2 pagesPDF 0OIutGciNYy1qLCkgEMFSusanta MohapatraNo ratings yet
- 19 AD CBT Mock Questions A4 V1 PDFDocument29 pages19 AD CBT Mock Questions A4 V1 PDFAncy JustineNo ratings yet
- Agreement Between 2D and 3D Radiographic Outcome Assessment 1 Year After Periapical SurgeryDocument11 pagesAgreement Between 2D and 3D Radiographic Outcome Assessment 1 Year After Periapical SurgeryMufidah NurulNo ratings yet
- Mycology Report 2Document6 pagesMycology Report 2Ange OuedraogoNo ratings yet
- PBL 1 Aspergillus - G1Document14 pagesPBL 1 Aspergillus - G1Rahmi Syarafina HakimNo ratings yet
- IV Pyelography procedure and nursing responsibilitiesDocument2 pagesIV Pyelography procedure and nursing responsibilitiesShaina Angelique SaliNo ratings yet
- Text BookDocument696 pagesText BookMaged Saif100% (9)
- Exercise # 3: How To Use CalculatorDocument5 pagesExercise # 3: How To Use CalculatorAbdullah SajidNo ratings yet