You might also like
- Aloe BookDocument136 pagesAloe Booktony6111100% (5)
- Holy Anointing Oil RecipeDocument4 pagesHoly Anointing Oil Recipewally ziembickiNo ratings yet
- Immune Response: Cell Biology and Its Application BI-1202Document35 pagesImmune Response: Cell Biology and Its Application BI-1202Eriani Wulandari100% (1)
- Magnesium DeficiencyDocument54 pagesMagnesium DeficiencyEdie M Murgia100% (1)
- 5 Myths and Truths About Massage Therapy FinalDocument50 pages5 Myths and Truths About Massage Therapy FinalElma McGouganNo ratings yet
- EarthworksDocument26 pagesEarthworksElvin G. TactacNo ratings yet
- Head and Neck OncologyDocument361 pagesHead and Neck OncologyDino Alberto MurilloNo ratings yet
- Ust Mock Boards 2017 - Micropara-1Document9 pagesUst Mock Boards 2017 - Micropara-1Lj Veneth100% (1)
- Comprehensive Aesthetic Rejuvenation Regional ApproachDocument188 pagesComprehensive Aesthetic Rejuvenation Regional ApproachRosa Maria Mercado100% (5)
- ColregDocument21 pagesColregVladimirNo ratings yet
- Schwartz Hour - BurnDocument62 pagesSchwartz Hour - BurnM3 SURGERY100% (1)
- Comprehensive Geriatric AssessmentDocument58 pagesComprehensive Geriatric Assessmentrisa astriaNo ratings yet
- Chapter7 B and T Cell Activation (1) ImmunologyDocument21 pagesChapter7 B and T Cell Activation (1) ImmunologyIka BakarNo ratings yet
- A Guide To Aim Global Business - South AfricaDocument36 pagesA Guide To Aim Global Business - South AfricaWa Tu LeeNo ratings yet
- ColregDocument21 pagesColregVladimirNo ratings yet
- Atopic DermatitisDocument74 pagesAtopic Dermatitiskhola aijazNo ratings yet
- Rw-01 - Along Daang Hari OnlyDocument1 pageRw-01 - Along Daang Hari OnlyRon Jovi GarciaNo ratings yet
- Estado Inmune de Sangre Del Cordon para Predecir Alergia y Asma - Allergy 2012Document4 pagesEstado Inmune de Sangre Del Cordon para Predecir Alergia y Asma - Allergy 2012Elisa FloresNo ratings yet
- ColregDocument21 pagesColregVladimirNo ratings yet
- Light X Diet X ZeroDocument10 pagesLight X Diet X ZeroMillena CristinaNo ratings yet
- Mechanisms of Immunotherapy in Allergic RhinitisDocument5 pagesMechanisms of Immunotherapy in Allergic RhinitisAchmad YunusNo ratings yet
- Actividad de Aprendizaje 5: Dalmiro Alberto Terán MuñozDocument9 pagesActividad de Aprendizaje 5: Dalmiro Alberto Terán MuñozDalmiro Alberto Teran MuñozNo ratings yet
- Immunosuppressant DrugsDocument8 pagesImmunosuppressant DrugsandruuuNo ratings yet
- Call To See Patient PDFDocument111 pagesCall To See Patient PDFKevin KhawNo ratings yet
- BiomoleculesDocument10 pagesBiomoleculesMohammed ArifuddinNo ratings yet
- Typhidot AssayDocument16 pagesTyphidot Assaychocoholic potchiNo ratings yet
- GINA Severe Asthma Guide 2023 PDFDocument51 pagesGINA Severe Asthma Guide 2023 PDFalfonsinaNo ratings yet
- Sinonim ObatDocument18 pagesSinonim ObatWin EfendiNo ratings yet
- The Dynamics of Dendritic Cell Mediated Innate Immune RegulationDocument6 pagesThe Dynamics of Dendritic Cell Mediated Innate Immune RegulationSofi Papel JachoNo ratings yet
- CROSSWORD QUIZ: Fire Protection (CONTROL) : L I G H T F E L L A I R T T TDocument2 pagesCROSSWORD QUIZ: Fire Protection (CONTROL) : L I G H T F E L L A I R T T Tmercyella prasetyaNo ratings yet
- L 1 Unit 1 Medicinal Chemistry LL LATEST LEARN PHARMACYDocument5 pagesL 1 Unit 1 Medicinal Chemistry LL LATEST LEARN PHARMACYYASH DESHMUKH 66No ratings yet
- Tryp Coloring-1Document2 pagesTryp Coloring-1Dheepikha ShivakumarNo ratings yet
- Pawankar R, Mori S, Ozu C, Kimura S 2011Document11 pagesPawankar R, Mori S, Ozu C, Kimura S 2011Pridho GaziansyahNo ratings yet
- Magnetic. InductionDocument1 pageMagnetic. InductionCeline ShawNo ratings yet
- Calmac Ice Storage AircoDocument4 pagesCalmac Ice Storage AircosukamtoNo ratings yet
- NO Sket/Lokasi: Daftar Ukuran Pipa-Pipa Yang Harus Diganti Baru Mt. Minas / P.35 Main Pipe Branch Pipe FittingDocument5 pagesNO Sket/Lokasi: Daftar Ukuran Pipa-Pipa Yang Harus Diganti Baru Mt. Minas / P.35 Main Pipe Branch Pipe FittingDhabierzt JiehNo ratings yet
- Imunologi Dasar Penyakit Alergi: OlehDocument38 pagesImunologi Dasar Penyakit Alergi: OlehtalithanrNo ratings yet
- 64a957e1f81b70001842ef6d - ## - Human Health and Diseases Handwritten Notes (Of Lecture 03)Document6 pages64a957e1f81b70001842ef6d - ## - Human Health and Diseases Handwritten Notes (Of Lecture 03)sourajeetsahoo2610No ratings yet
- Appendix I: IA IUPAC Nucleotide Ambiguity CodesDocument2 pagesAppendix I: IA IUPAC Nucleotide Ambiguity Codespeeps007No ratings yet
- Zain Ul Abdin F2020381019 (CP SEC A)Document4 pagesZain Ul Abdin F2020381019 (CP SEC A)Aqib LatifNo ratings yet
- Asthma: Retno Ariza S Soemarwoto PulmologistDocument18 pagesAsthma: Retno Ariza S Soemarwoto PulmologistAulidaweli DasrulNo ratings yet
- Jurnal Rhinosinusitis KronisDocument12 pagesJurnal Rhinosinusitis Kronismutia saraNo ratings yet
- Namrata Final PaperDocument22 pagesNamrata Final PaperAngel TechNo ratings yet
- DataHaven Greater New Haven Community Index 2019Document124 pagesDataHaven Greater New Haven Community Index 2019Helen BennettNo ratings yet
- Selective N-Alkylation of Aniline With Methanol Over ,/-AluminaDocument14 pagesSelective N-Alkylation of Aniline With Methanol Over ,/-Aluminaabubakar chohaanNo ratings yet
- Immunology of Tuberculosis: Steffen Stenger, Medical Microbiology and Infection Control, University Hospital Ulm, GermanyDocument11 pagesImmunology of Tuberculosis: Steffen Stenger, Medical Microbiology and Infection Control, University Hospital Ulm, GermanyElizabeth AlbarránNo ratings yet
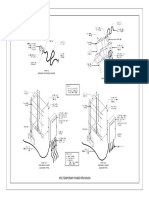
- Site Temporary Power Provision: Type "A" Ordinary Extension Chord Type "B"Document1 pageSite Temporary Power Provision: Type "A" Ordinary Extension Chord Type "B"Maverick OmnesNo ratings yet
- CSS THT 2Document12 pagesCSS THT 2Milzam TarisNo ratings yet
- DVT MicroDocument38 pagesDVT MicroInsha HaSanNo ratings yet
- FB011 Sample PDFDocument10 pagesFB011 Sample PDFDilara KüçükkurtNo ratings yet
- Probing Opioid Signalosome in NeuroblastomaDocument35 pagesProbing Opioid Signalosome in Neuroblastomalara gay villaruzNo ratings yet
- Bellaskywayfestivalprogram 2018 enDocument21 pagesBellaskywayfestivalprogram 2018 enPatríciaFreireNo ratings yet
- ACE37 Oct90Document172 pagesACE37 Oct90lerainlawlietNo ratings yet
- Evidencia 5 BilinguismoDocument8 pagesEvidencia 5 BilinguismoValentina JimenezNo ratings yet
- NO Sket/Lokasi: Daftar Ukuran Pipa-Pipa Yang Harus Diganti Baru Mt. Minas / P.35 Main Pipe Branch Pipe FittingDocument8 pagesNO Sket/Lokasi: Daftar Ukuran Pipa-Pipa Yang Harus Diganti Baru Mt. Minas / P.35 Main Pipe Branch Pipe FittingDhabierzt JiehNo ratings yet
- Workshop: Getting Started As A TranslatorDocument8 pagesWorkshop: Getting Started As A TranslatorTatiana Garrido SuarrezNo ratings yet
- Dosage Adjustment in Renal DiseaseDocument25 pagesDosage Adjustment in Renal DiseaseAswin DamodaranNo ratings yet
- Journal Reading - Allergic Rhinitis - Safira AmaliaDocument34 pagesJournal Reading - Allergic Rhinitis - Safira AmaliasafiraNo ratings yet
- Cmi 201759Document3 pagesCmi 201759Rahul VermaNo ratings yet
- 2008 Atopic Dermatitis Mechanism of DiseaseDocument12 pages2008 Atopic Dermatitis Mechanism of DiseaseAlma EscobarNo ratings yet
- Asthma PhenotypesDocument45 pagesAsthma PhenotypesAlina CaraciobanuNo ratings yet
- Farmaco Bac ExcelDocument25 pagesFarmaco Bac ExcelivanNo ratings yet
- Business Card Sawara8888Document1 pageBusiness Card Sawara8888Ashutosh MohantyNo ratings yet
- Ijcem0008 15752Document9 pagesIjcem0008 15752Kiki BakriNo ratings yet
- 3,5-Bis (2-Indolyl) Pyridine and 3 - ( (2-Indolyl) - 5-Phenyl) Pyrid PDFDocument22 pages3,5-Bis (2-Indolyl) Pyridine and 3 - ( (2-Indolyl) - 5-Phenyl) Pyrid PDFpaiaravindNo ratings yet
- Documento - GINA AsmaDocument42 pagesDocumento - GINA AsmaDarck birdNo ratings yet
- (Lecture 2) Skin TestDocument31 pages(Lecture 2) Skin TestShubham KadiwalaNo ratings yet
- Futuro de Inmunoterapia Especifica Con AlergenosDocument10 pagesFuturo de Inmunoterapia Especifica Con Alergenoscaronte2108No ratings yet
- Hipoparatiroidisme PDFDocument2 pagesHipoparatiroidisme PDFRyan aginta 1No ratings yet
- Immune Responses in The Oral CavityDocument1 pageImmune Responses in The Oral CavityCiro GuerraNo ratings yet
- Allergy Blood Test (IgE)Document5 pagesAllergy Blood Test (IgE)Muhammad RaheemNo ratings yet
- Hypersensitivity ReactionsDocument2 pagesHypersensitivity ReactionsMythily VedhagiriNo ratings yet
- Fitoestrógenos y Sus EfectosDocument7 pagesFitoestrógenos y Sus EfectosRuther Miranda MNo ratings yet
- Antibody: Von Ryan F. Lingcallo, RMTDocument33 pagesAntibody: Von Ryan F. Lingcallo, RMTJuan SalenNo ratings yet
- Pharm.D 2nd Year SyllabusDocument21 pagesPharm.D 2nd Year Syllabus12 E 36 Yatri PatelNo ratings yet
- Contoh RESEARCH PROPOSALDocument8 pagesContoh RESEARCH PROPOSALJuliand HidayatNo ratings yet
- Juvenileidiopathic Arthritis: Peter J. Gowdie,, Shirley M.L. TseDocument27 pagesJuvenileidiopathic Arthritis: Peter J. Gowdie,, Shirley M.L. TseFandi ArgiansyaNo ratings yet
- WBC SummaryDocument10 pagesWBC SummaryNeilJohnL.OrineoNo ratings yet
- Proceedings of The 14th European Immunogenicity Platform Open Symposium On Immunogenicity of BiopharmaceuticalsDocument8 pagesProceedings of The 14th European Immunogenicity Platform Open Symposium On Immunogenicity of Biopharmaceuticalsgskcl429No ratings yet
- Food NutritionsDocument3 pagesFood NutritionsCindy SaputriNo ratings yet
- Conceptus-Modulated Innate Immune Function During Early Pregnancy in Ruminants - A Review (Rocha C. C. Et Al. 2021)Document16 pagesConceptus-Modulated Innate Immune Function During Early Pregnancy in Ruminants - A Review (Rocha C. C. Et Al. 2021)Vanessa BussNo ratings yet
- BioDocument9 pagesBioJayAnneLiporadaNo ratings yet
- The Pathogenesis of Graves' Disease: Bryan Mciver, MBCHB, and John C. MorrisDocument17 pagesThe Pathogenesis of Graves' Disease: Bryan Mciver, MBCHB, and John C. MorrisSOPHIASTIA KUSBIANTI MHS 2017No ratings yet
- Gene TherapyDocument20 pagesGene Therapyhimikotoga1123No ratings yet
- Organization and Expression of Ig GenesDocument54 pagesOrganization and Expression of Ig GenesViswa TejaNo ratings yet
- Actualización de Inmunoterapia en CáncerDocument13 pagesActualización de Inmunoterapia en CáncerAli BelloNo ratings yet
- (Current Topics in Microbiology and Immunology) Michael G. Katze - Systems Biology-Springer (2013)Document276 pages(Current Topics in Microbiology and Immunology) Michael G. Katze - Systems Biology-Springer (2013)giulianavictoria1No ratings yet
- The Effects of Different Levels of Sodium Diformate on Growth Performance, Immunological Respond, Digestive Enzyme Activity and Intestinal Histomorphology in Juvenile Siberian Sturgeon Acipenser Baerii-2Document8 pagesThe Effects of Different Levels of Sodium Diformate on Growth Performance, Immunological Respond, Digestive Enzyme Activity and Intestinal Histomorphology in Juvenile Siberian Sturgeon Acipenser Baerii-2Poohfa JirathNo ratings yet
- Controversies in PeriodonticsDocument56 pagesControversies in PeriodonticsReshmaa Rajendran100% (1)