You might also like
- Acute Fulminant Hepatic Failure Due To Hepatitis A Virus: A Case ReportDocument3 pagesAcute Fulminant Hepatic Failure Due To Hepatitis A Virus: A Case ReportTor JaNo ratings yet
- Visceral Leishmaniasis Turning into Chronic Liver DiseaseDocument4 pagesVisceral Leishmaniasis Turning into Chronic Liver DiseasePratyay HasanNo ratings yet
- Bosentan Hepatotoxicity Case ReportDocument4 pagesBosentan Hepatotoxicity Case Reportefra maneNo ratings yet
- Umayam Patho & Drug Study 3rd RotationDocument6 pagesUmayam Patho & Drug Study 3rd RotationRyan Dave UmayamNo ratings yet
- Case Report Glycogenic Hepatopathy in Type 1 Diabetes MellitusDocument4 pagesCase Report Glycogenic Hepatopathy in Type 1 Diabetes MellitusCarlos Alberto Rodriguez ValbuenaNo ratings yet
- The treatment of diabetes mellitus in patients with chronic liver diseaseDocument9 pagesThe treatment of diabetes mellitus in patients with chronic liver diseaseRista mokogintaNo ratings yet
- Bezafibrate: 1232 Cardiovascular DrugsDocument3 pagesBezafibrate: 1232 Cardiovascular DrugslichenresearchNo ratings yet
- 01 Hyp 5 4 623Document5 pages01 Hyp 5 4 623crbl64No ratings yet
- Wa0013Document4 pagesWa0013Sastra WijayaNo ratings yet
- Initial evaluation reveals quadriplegia after epidural hematomaDocument12 pagesInitial evaluation reveals quadriplegia after epidural hematomaMargareth Christine CusoNo ratings yet
- SopDocument13 pagesSopAnita OctaviaNo ratings yet
- Assessing Risk of Bleeding in a Patient with Acute GastroenteritisDocument3 pagesAssessing Risk of Bleeding in a Patient with Acute GastroenteritisAce Dioso Tubasco100% (2)
- MW2 DRUG STUDYDocument2 pagesMW2 DRUG STUDYc.cagas.529054No ratings yet
- Anticoagulants TransaminasesDocument5 pagesAnticoagulants TransaminasesSony Eka NugrahaNo ratings yet
- Concept Map Level 4 Student for C.GDocument3 pagesConcept Map Level 4 Student for C.GdguginNo ratings yet
- 述评 Human Albumin Infusion Strategy in Liver Cirrhosis Liberal or RestrictiveDocument3 pages述评 Human Albumin Infusion Strategy in Liver Cirrhosis Liberal or Restrictive倪沁赟No ratings yet
- 1-4-3 Liver Cirrhosis - Group 3Document35 pages1-4-3 Liver Cirrhosis - Group 3Maica LectanaNo ratings yet
- 133 141 FrancoisDocument9 pages133 141 Francoiscamapafe7873No ratings yet
- Case Based Learning Renal and EndocrineDocument38 pagesCase Based Learning Renal and EndocrineSyeren VenesiaNo ratings yet
- Compli Cirrhosis RXDocument10 pagesCompli Cirrhosis RXdrgmavmhNo ratings yet
- Propranolol in The Management of Portal Hypertension: Manisha Dwivedi, S. P. MisraDocument7 pagesPropranolol in The Management of Portal Hypertension: Manisha Dwivedi, S. P. MisraazedaaNo ratings yet
- Drug Study of FurosemideDocument5 pagesDrug Study of FurosemideAntonette Lei100% (1)
- Mw2 Drug StudyDocument2 pagesMw2 Drug Studyc.cagas.529054No ratings yet
- Bevacizumab Therapy Reduces PH in HHT Patient with Liver DiseaseDocument9 pagesBevacizumab Therapy Reduces PH in HHT Patient with Liver DiseaseAli Uğur SoysalNo ratings yet
- DR A-Mwafy 1 Hepatology 4Document29 pagesDR A-Mwafy 1 Hepatology 4عبد الله عبد اللهNo ratings yet
- Clinical Liver Disease - 2012 - Reverter - Management of An Acute Variceal Bleeding EpisodeDocument4 pagesClinical Liver Disease - 2012 - Reverter - Management of An Acute Variceal Bleeding EpisodeEUODIA HANA KRISTINANo ratings yet
- Cilnidipine Adverse Effect in Hypertensive Chronic Kidney Disease Patient With Pedal Edema A Case ReportDocument3 pagesCilnidipine Adverse Effect in Hypertensive Chronic Kidney Disease Patient With Pedal Edema A Case Reportvyshnavi machirajuNo ratings yet
- PIIS1053077018310437Document5 pagesPIIS1053077018310437andi rahmatNo ratings yet
- Gloomy LifeDocument6 pagesGloomy LifeLanna HarumiyaNo ratings yet
- Dolan Drug StudyDocument3 pagesDolan Drug StudyLian Robbie BautistaNo ratings yet
- Zomen in CKDDocument12 pagesZomen in CKDClaudiu BalabanNo ratings yet
- European J of Heart Fail - 2018 - Mullens - Rationale and Design of The ADVOR Acetazolamide in Decompensated Heart FailureDocument10 pagesEuropean J of Heart Fail - 2018 - Mullens - Rationale and Design of The ADVOR Acetazolamide in Decompensated Heart FailureAnnisa Tria FadillaNo ratings yet
- 2014 Article 109Document4 pages2014 Article 109luckytacandraNo ratings yet
- Penunjang Pemeriksaan KlinisDocument88 pagesPenunjang Pemeriksaan Klinisgrady_christian_9720No ratings yet
- Liver Friendly GERD ManagementDocument5 pagesLiver Friendly GERD ManagementInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Thrombocytopenia Treatment in Chronic Liver DiseaseDocument11 pagesThrombocytopenia Treatment in Chronic Liver DiseasePablo AlvarezNo ratings yet
- Liver CirrhosisDocument9 pagesLiver CirrhosismedsmracelisNo ratings yet
- Hep4 1 726Document10 pagesHep4 1 726Medicina InternaNo ratings yet
- Stase Gastro SirosisDocument27 pagesStase Gastro SirosisLuluFanDyNo ratings yet
- Try Out CompilationDocument17 pagesTry Out CompilationRendi RafsanjaniNo ratings yet
- Propanolol Dan Hipertensi PortalDocument6 pagesPropanolol Dan Hipertensi PortalIndah LestariNo ratings yet
- Lipitor A Drug Study OnDocument8 pagesLipitor A Drug Study OnAlexandrea MayNo ratings yet
- Acute Renal Failure CaseDocument4 pagesAcute Renal Failure CaseMayer RosenbergNo ratings yet
- AMLODIPINEDocument3 pagesAMLODIPINESL Hanna NebridaNo ratings yet
- NCP Sunga Mariane G. BSN4 5Document6 pagesNCP Sunga Mariane G. BSN4 5Erryl Justine AdvinculaNo ratings yet
- Lipitor Drug Study for Emergency NursingDocument8 pagesLipitor Drug Study for Emergency NursingAlexandrea MayNo ratings yet
- Liver Functions, Gastric Functions and Pancreatic Functions TestsDocument26 pagesLiver Functions, Gastric Functions and Pancreatic Functions TestsHoping HeartsNo ratings yet
- Lipitor A Drug Study OnDocument7 pagesLipitor A Drug Study OnAlexandrea MayNo ratings yet
- Generic Name:: Drug Name Indicatio N Mechanism of Action Side Effects Nursing ResponsibilitiesDocument1 pageGeneric Name:: Drug Name Indicatio N Mechanism of Action Side Effects Nursing Responsibilitiesgrace pitogoNo ratings yet
- Nursing Diagnosis Nursing Diagnosis: Nursing Diagnosis:: Kidney Biopsy - Diffuse Proliferative GlomerulonephritisDocument1 pageNursing Diagnosis Nursing Diagnosis: Nursing Diagnosis:: Kidney Biopsy - Diffuse Proliferative GlomerulonephritisRiza Angela BarazanNo ratings yet
- Hepatic AdenomaDocument4 pagesHepatic AdenomadnnivNo ratings yet
- Clinical Liver Disease - 2021 - Sharma - Liver Abscess Complications and TreatmentDocument5 pagesClinical Liver Disease - 2021 - Sharma - Liver Abscess Complications and TreatmentNaldo NathanNo ratings yet
- 2013 Article 788Document5 pages2013 Article 788skripsi kapNo ratings yet
- Trousseau’s Syndrome in CholangiocarcinomaDocument7 pagesTrousseau’s Syndrome in CholangiocarcinomaAnna MariaNo ratings yet
- 5.5.5 BMJ Case Reports 2018 Pizzarossa RodríguezDocument3 pages5.5.5 BMJ Case Reports 2018 Pizzarossa RodríguezAna PizzarossaNo ratings yet
- Philip 2016Document5 pagesPhilip 2016Nindya EsesNo ratings yet
- B74. HELLP Syndrome An Atypical Presentation PDFDocument3 pagesB74. HELLP Syndrome An Atypical Presentation PDFjhon heriansyahNo ratings yet
- Levy Mwanawasa University Teaching Hospital Pharmaceutical Care PlanDocument6 pagesLevy Mwanawasa University Teaching Hospital Pharmaceutical Care PlanTowela BandaNo ratings yet
- Clopidogrel Bisulfate (PLOGREL)Document2 pagesClopidogrel Bisulfate (PLOGREL)Kristine Young0% (1)
- Hobfoll Et Al., 2018 PDFDocument28 pagesHobfoll Et Al., 2018 PDFQundeel HaiderNo ratings yet
- Corporate Governance Integration With Sustainability: A Systematic Literature ReviewDocument15 pagesCorporate Governance Integration With Sustainability: A Systematic Literature ReviewmehakNo ratings yet
- Journal of Cleaner Production: Marco Formentini, Paolo TaticchiDocument14 pagesJournal of Cleaner Production: Marco Formentini, Paolo TaticchiJuan AlmeydaNo ratings yet
- Impact of Corporate Governance On Corporate Sustainable GrowthDocument18 pagesImpact of Corporate Governance On Corporate Sustainable GrowthmehakNo ratings yet
- A Review of The Challenge-Hindrance Stress Model: Recent Advances, Expanded Paradigms, and Recommendations For Future ResearchDocument12 pagesA Review of The Challenge-Hindrance Stress Model: Recent Advances, Expanded Paradigms, and Recommendations For Future ResearchmehakNo ratings yet
- BoswellOlson BuchananLePine2004JVBStressDocument18 pagesBoswellOlson BuchananLePine2004JVBStressmehakNo ratings yet
- Job Satisfaction, Organizational Commitment and Job Involvement: The Mediating Role of Job InvolvementDocument12 pagesJob Satisfaction, Organizational Commitment and Job Involvement: The Mediating Role of Job InvolvementmehakNo ratings yet
- The Relationship Between Challenge and Hindrance Stressors and Emotional Exhaustion: The Moderating Role of Perceived Servant LeadershipDocument15 pagesThe Relationship Between Challenge and Hindrance Stressors and Emotional Exhaustion: The Moderating Role of Perceived Servant LeadershipmehakNo ratings yet
- The Corporate Governance of Environmental Sustainability: A Review and Proposal For More Integrated ResearchDocument30 pagesThe Corporate Governance of Environmental Sustainability: A Review and Proposal For More Integrated ResearchmehakNo ratings yet
- Ijbel22 204Document9 pagesIjbel22 204mehakNo ratings yet
- A Review Corporate Governance and SustainabilityDocument11 pagesA Review Corporate Governance and SustainabilitymehakNo ratings yet
- Impact of Corporate Governance On Corporate Sustainable GrowthDocument18 pagesImpact of Corporate Governance On Corporate Sustainable GrowthmehakNo ratings yet
- Ijbel22 204Document9 pagesIjbel22 204mehakNo ratings yet
- Corporate Governance Integration With Sustainability: A Systematic Literature ReviewDocument15 pagesCorporate Governance Integration With Sustainability: A Systematic Literature ReviewmehakNo ratings yet
- The Corporate Governance of Environmental Sustainability: A Review and Proposal For More Integrated ResearchDocument30 pagesThe Corporate Governance of Environmental Sustainability: A Review and Proposal For More Integrated ResearchmehakNo ratings yet
- A Review Corporate Governance and SustainabilityDocument11 pagesA Review Corporate Governance and SustainabilitymehakNo ratings yet
- Journal of Cleaner Production: Marco Formentini, Paolo TaticchiDocument14 pagesJournal of Cleaner Production: Marco Formentini, Paolo TaticchiJuan AlmeydaNo ratings yet
- A Review Corporate Governance and SustainabilityDocument11 pagesA Review Corporate Governance and SustainabilitymehakNo ratings yet
- Governance and SustainabilityDocument17 pagesGovernance and SustainabilitymehakNo ratings yet
- Ijbel22 204Document9 pagesIjbel22 204mehakNo ratings yet
- Journal of Cleaner Production: Marco Formentini, Paolo TaticchiDocument14 pagesJournal of Cleaner Production: Marco Formentini, Paolo TaticchiJuan AlmeydaNo ratings yet
- The Corporate Governance of Environmental Sustainability: A Review and Proposal For More Integrated ResearchDocument30 pagesThe Corporate Governance of Environmental Sustainability: A Review and Proposal For More Integrated ResearchmehakNo ratings yet
- Corporate Governance Integration With Sustainability: A Systematic Literature ReviewDocument15 pagesCorporate Governance Integration With Sustainability: A Systematic Literature ReviewmehakNo ratings yet
- Michel On 2010Document33 pagesMichel On 2010Tawsif HasanNo ratings yet
- Current Management of Hepatocellular Carcinoma: Ana Maria Crissien, MD, and Catherine Frenette, MDDocument9 pagesCurrent Management of Hepatocellular Carcinoma: Ana Maria Crissien, MD, and Catherine Frenette, MDmehakNo ratings yet
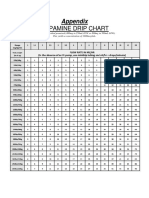
- Dopamine Drip Chart AppendixDocument1 pageDopamine Drip Chart AppendixmehakNo ratings yet
- Relationship Between Corporate Governance, Corporate Sustainability and Financial PerformanceDocument21 pagesRelationship Between Corporate Governance, Corporate Sustainability and Financial PerformancemehakNo ratings yet
- Impact of Corporate Governance On Corporate Sustainable GrowthDocument18 pagesImpact of Corporate Governance On Corporate Sustainable GrowthmehakNo ratings yet
- Guias Del Uso de Albumina e IgGDocument19 pagesGuias Del Uso de Albumina e IgGRonny Muñoz AcuñaNo ratings yet
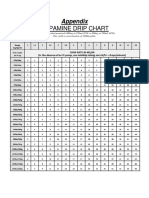
- Dopamine Drip ChartDocument1 pageDopamine Drip ChartmehakNo ratings yet
- Pathophysiology of Hypovolemic ShockDocument8 pagesPathophysiology of Hypovolemic ShockKAYCEENo ratings yet
- Understanding Liver CirrhosisDocument54 pagesUnderstanding Liver CirrhosisaprillyaNo ratings yet
- Ase Resentation: Marianne Angelina R. Lorenzo Post-Graduate InternDocument65 pagesAse Resentation: Marianne Angelina R. Lorenzo Post-Graduate InternMarianne R. LorenzoNo ratings yet
- Aksha Poster AbstractDocument14 pagesAksha Poster Abstractडॉ यश तलेराNo ratings yet
- Cirrhosis ToolkitDocument39 pagesCirrhosis Toolkitvr venkatesanNo ratings yet
- Tjandra MCQDocument35 pagesTjandra MCQnz chuksNo ratings yet
- Causes of Sis and Management of A CaseDocument26 pagesCauses of Sis and Management of A CaseEmmanuelLazarusNo ratings yet
- Is Caviar Disease (Sublingual Varices) Associated With Trauma?Document2 pagesIs Caviar Disease (Sublingual Varices) Associated With Trauma?Mardiyah PratiwiNo ratings yet
- GI BleedDocument96 pagesGI Bleedjaish8904100% (2)
- Fatty Liver AssignmentDocument9 pagesFatty Liver AssignmentMaryam ShahzadiNo ratings yet
- GI BleedingDocument8 pagesGI BleedingNemanja VukcevicNo ratings yet
- Practical Approach To GIB Dr. Chris Huang 7.12.2013Document86 pagesPractical Approach To GIB Dr. Chris Huang 7.12.2013Juni Zuhairah Abd GhafarNo ratings yet
- Spleen and Liver Sur LecDocument14 pagesSpleen and Liver Sur LecYA M AYNo ratings yet
- GI Bleeding Case 2Document4 pagesGI Bleeding Case 2Imah ArmildezNo ratings yet
- Varices Esophagus PDFDocument7 pagesVarices Esophagus PDFDimas ErlanggaNo ratings yet
- GI 2007 Exam QuestionsDocument47 pagesGI 2007 Exam QuestionsRoh JitenNo ratings yet
- Brochure Ultrasonograph y of The Live Ru 42 eDocument132 pagesBrochure Ultrasonograph y of The Live Ru 42 ealiceinwinterNo ratings yet
- Esophageal Varices Diagnosis and TreatmentDocument20 pagesEsophageal Varices Diagnosis and Treatmentx483xDNo ratings yet
- Nihms 818708Document22 pagesNihms 818708bela RachmanNo ratings yet
- Portal Vein Thrombosis: ReviewDocument9 pagesPortal Vein Thrombosis: ReviewMahmoud AbouelsoudNo ratings yet
- Non-Variceal Upper GI Bleeding GuideDocument34 pagesNon-Variceal Upper GI Bleeding GuideChe Ainil ZainodinNo ratings yet
- Gastrointestinal: High-Yield SystemsDocument46 pagesGastrointestinal: High-Yield SystemsArvindNo ratings yet
- Cirrhosis in Adults - Overview of Complications, General Management, and PrognosisDocument24 pagesCirrhosis in Adults - Overview of Complications, General Management, and PrognosisAhraxazel Galicia ReynaNo ratings yet
- Hepatitis B in PregnancyDocument23 pagesHepatitis B in PregnancyBrooly Denfrek100% (1)
- Previous MRCP II ExamsDocument247 pagesPrevious MRCP II ExamsAdil Shabbir100% (3)
- Baveno IVDocument10 pagesBaveno IVdepe_cutzNo ratings yet
- Non-Invasive Panel For Prediction of Large Esophageal Varices in Patients With HCV-Related Cirrhosis After DAAS TherapyDocument15 pagesNon-Invasive Panel For Prediction of Large Esophageal Varices in Patients With HCV-Related Cirrhosis After DAAS TherapyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Doppler US Validates Portal Vein Flow in CirrhosisDocument5 pagesDoppler US Validates Portal Vein Flow in CirrhosisL0v3B00k5No ratings yet
- GI Bleeding - NursesDocument71 pagesGI Bleeding - Nursesapi-3760283100% (6)
- CASE 1 Group 2 7 1Document4 pagesCASE 1 Group 2 7 1Monique BorresNo ratings yet