You might also like
- Systemic BacteriologyDocument495 pagesSystemic BacteriologyAkash KaranwalNo ratings yet
- ASCP ReviewerDocument8 pagesASCP Reviewergillian102290100% (6)
- Medtech ReviewerDocument4 pagesMedtech ReviewerLyudmyla Gillego100% (4)
- Berklee Intro Music Therapy PDFDocument17 pagesBerklee Intro Music Therapy PDFTheodore VaillantNo ratings yet
- 3 MDRRMC SampleDocument57 pages3 MDRRMC SampleMakoy Salonga100% (2)
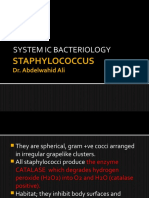
- 34 Staphylococcus - IncompleteDocument9 pages34 Staphylococcus - IncompleteHarshada GhanekarNo ratings yet
- 1.1 Gram Positive CocciDocument9 pages1.1 Gram Positive CocciJustine Mel Concepcion IlardeNo ratings yet
- S. AureusDocument39 pagesS. AureusRajkishor YadavNo ratings yet
- A. Staphylococcus Aureus B. Staphylococcus Epidermidis C. Staphylococcus SaprophyticusDocument8 pagesA. Staphylococcus Aureus B. Staphylococcus Epidermidis C. Staphylococcus SaprophyticusRuel MaddawinNo ratings yet
- MSK StaphDocument3 pagesMSK Staphعبدالرحمن عابدNo ratings yet
- Microbiology TablesDocument19 pagesMicrobiology TablesRebecca MarshallNo ratings yet
- CB Part 3Document76 pagesCB Part 3Mohammad MambuayNo ratings yet
- Gram-Positive Cocci Staphylococci Morphology Identification DiseasesDocument24 pagesGram-Positive Cocci Staphylococci Morphology Identification DiseasesTayyaba TahiraNo ratings yet
- Finasls 1 Staph Strep PDFDocument50 pagesFinasls 1 Staph Strep PDFFrancis ValdezNo ratings yet
- Gram Positive Cocci Sem 1 1Document45 pagesGram Positive Cocci Sem 1 1Charmaine Corpuz Granil100% (1)
- Staphylococcus & StreptococcusDocument100 pagesStaphylococcus & StreptococcusFahim NadvyNo ratings yet
- Screenshot 2021-06-04 at 23.19.29Document72 pagesScreenshot 2021-06-04 at 23.19.29Amina Mohamed AbdikeirNo ratings yet
- Definition: Gram +ve CocciDocument50 pagesDefinition: Gram +ve Cocciliyana04_08No ratings yet
- 760 Staphylococcus PPT UG LectureDocument47 pages760 Staphylococcus PPT UG Lectureridwan.biotekNo ratings yet
- L1 - StaphylococciDocument35 pagesL1 - Staphylococciyouservezeropurpose113No ratings yet
- 1 - Systemic BacteriologyDocument316 pages1 - Systemic BacteriologyAlsirNo ratings yet
- Strepto Cocci PDFDocument34 pagesStrepto Cocci PDFMustafa SaßerNo ratings yet
- Strep_ 2020 Nov_pDocument16 pagesStrep_ 2020 Nov_pHUỲNH QUỐC KHÁNHNo ratings yet
- Bacterial Infections of The SkinDocument9 pagesBacterial Infections of The Skinbeia21No ratings yet
- Gram Positive Cocci The Staphylococci CharacteristicsDocument15 pagesGram Positive Cocci The Staphylococci CharacteristicsKyle PicocNo ratings yet
- Streptococcus Pneumoniae MbbsDocument53 pagesStreptococcus Pneumoniae MbbsShyam MishraNo ratings yet
- Gram Positive Cocci Genera Staphylococci and Streptococci Medical ImportanceDocument40 pagesGram Positive Cocci Genera Staphylococci and Streptococci Medical ImportanceAshwani Mathur, Ma-306100% (1)
- STREPTOCOCCUSDocument24 pagesSTREPTOCOCCUSTUSHAR MORESHWARNo ratings yet
- Family of StreptococcaceaeDocument10 pagesFamily of StreptococcaceaeLovely B. AlipatNo ratings yet
- Gram Positive Cocci StaphylococciDocument41 pagesGram Positive Cocci StaphylococciZainab ElgehaniNo ratings yet
- Streptococcus SPPDocument52 pagesStreptococcus SPPdrnuaman5No ratings yet
- GRAM Positive CocciDocument67 pagesGRAM Positive CocciNoraine Princess TabangcoraNo ratings yet
- Staphylococci identification and virulence factorsDocument5 pagesStaphylococci identification and virulence factorskerynne dyNo ratings yet
- Pre 1 MibrobiologyDocument3 pagesPre 1 MibrobiologyDeannise AnnNo ratings yet
- Bacterial Agents of Cardio-Vascular DiseasesDocument43 pagesBacterial Agents of Cardio-Vascular Diseasesfitrah fajrianiNo ratings yet
- StreptococcusDocument4 pagesStreptococcusTejpalNo ratings yet
- New Microsoft Office Word DocumentDocument4 pagesNew Microsoft Office Word DocumentTejpalNo ratings yet
- Dams Lastlook Microbiology PDFDocument27 pagesDams Lastlook Microbiology PDFChauhan Monika100% (1)
- 81139.1613396781micro 1 FinalDocument27 pages81139.1613396781micro 1 FinalDiptangshu PalNo ratings yet
- Staphylococci & MicrococciDocument52 pagesStaphylococci & Micrococcihoneylemon.coNo ratings yet
- Prepared By: Ken Robin A. Canada, RMT, Mls AscpiDocument35 pagesPrepared By: Ken Robin A. Canada, RMT, Mls AscpiKen Robin CanadaNo ratings yet
- Micro Rapid ReviewDocument6 pagesMicro Rapid ReviewEvan Miller100% (3)
- Microbiologia de Murray 8va Edicion-194-227Document34 pagesMicrobiologia de Murray 8va Edicion-194-227Ailyn Montalvo FigueroaNo ratings yet
- Staphylococcus: Zeinab Abd Elkhalek Prof. of Medical Microbiology & ImmunologyDocument26 pagesStaphylococcus: Zeinab Abd Elkhalek Prof. of Medical Microbiology & ImmunologyMustafa SaßerNo ratings yet
- Molecular and biochemical characterization of Staphylococcus aureus β-lactamaseDocument8 pagesMolecular and biochemical characterization of Staphylococcus aureus β-lactamaseMaha hameedNo ratings yet
- Gram Positive Cocci Identification and DifferentiationDocument45 pagesGram Positive Cocci Identification and DifferentiationCharmaine Corpuz GranilNo ratings yet
- Piogenic Cocci: Ania Kurniawati PD, Dr. MkesDocument58 pagesPiogenic Cocci: Ania Kurniawati PD, Dr. MkesSilmi Zhillan Nur RahmanNo ratings yet
- Neisseria GonorrhoeaDocument33 pagesNeisseria Gonorrhoeaprabad dunusingheNo ratings yet
- staplylococci محاضرة الاولىDocument20 pagesstaplylococci محاضرة الاولىArwa HussienNo ratings yet
- MICROBIOLOGYDocument7 pagesMICROBIOLOGYjiangNo ratings yet
- Microbiology Special Report: General Template for Characterizing Important MicrobesDocument68 pagesMicrobiology Special Report: General Template for Characterizing Important MicrobesrefuapalackyNo ratings yet
- Pyogenic Cocci Pyogenic Means " Pus Forming" Cocci Means "Spherical Bacteria"Document14 pagesPyogenic Cocci Pyogenic Means " Pus Forming" Cocci Means "Spherical Bacteria"Ab AbNo ratings yet
- Staphylococcus: Made By: Shalini BishtDocument70 pagesStaphylococcus: Made By: Shalini BishtEduardo SalazarNo ratings yet
- Staphylococcus: Made By: Shalini BishtDocument70 pagesStaphylococcus: Made By: Shalini BishtEduardo SalazarNo ratings yet
- Infectious DiseasesDocument37 pagesInfectious Diseasespolaris_027No ratings yet
- StreptococciDocument10 pagesStreptococciGea MarieNo ratings yet
- StreptococcusDocument6 pagesStreptococcusrita900717No ratings yet
- Basic MicrobiologyDocument53 pagesBasic MicrobiologyJohn NirmalNo ratings yet
- Mass Spectrometric Analysis of The Secretome of Candida AlbicansDocument12 pagesMass Spectrometric Analysis of The Secretome of Candida AlbicansPedro ItaloNo ratings yet
- Yeasts Undergraduate Recording 2021Document33 pagesYeasts Undergraduate Recording 2021Dabrat JullzNo ratings yet
- Micro CDBDocument9 pagesMicro CDBLicensed to HealNo ratings yet
- MSDS for Feldspar PowderDocument7 pagesMSDS for Feldspar PowderRıdvan SürmeliNo ratings yet
- Human Resources Manager in San Jose CA Resume Priscilla CramerDocument2 pagesHuman Resources Manager in San Jose CA Resume Priscilla CramerPriscillaCramerNo ratings yet
- CPT 2021 guide for identifying medical proceduresDocument7 pagesCPT 2021 guide for identifying medical proceduresChester FernandezNo ratings yet
- 270 lbs. man's 6-meal diet and workout planDocument10 pages270 lbs. man's 6-meal diet and workout planYuuki XDNo ratings yet
- RaweDocument34 pagesRaweSonuNo ratings yet
- Vacation With Sunny Leone - Without FlightDocument4 pagesVacation With Sunny Leone - Without FlightkalidasdoraemonNo ratings yet
- Understanding patients' and healthcare providers' confidentiality rights and obligationsDocument2 pagesUnderstanding patients' and healthcare providers' confidentiality rights and obligationsMelody B. MiguelNo ratings yet
- UG MaharashtraNationalLawUniversityMNLUMumbaiDocument5 pagesUG MaharashtraNationalLawUniversityMNLUMumbaiArpan KushwahaNo ratings yet
- 2020 Lamberti RCT Effectiveness of RBFT Slow Walking On Mobility in Severe Multiple SclerosisDocument11 pages2020 Lamberti RCT Effectiveness of RBFT Slow Walking On Mobility in Severe Multiple SclerosisArmin ParavlićNo ratings yet
- Top 10 Graphic Design Interview Questions and AnswersDocument16 pagesTop 10 Graphic Design Interview Questions and Answersbetsjonh100% (1)
- Connectors 2Document14 pagesConnectors 2Irene SánchezNo ratings yet
- Metabolic Surge - Rapid Fat Loss ProgramDocument5 pagesMetabolic Surge - Rapid Fat Loss ProgramTamer Luka100% (2)
- Cea SDocument10 pagesCea Syousra zeidanNo ratings yet
- Nursing Care Plan for Patient SafetyDocument9 pagesNursing Care Plan for Patient SafetyACOB, Jamil C.No ratings yet
- Concussionspaper 1Document6 pagesConcussionspaper 1api-350027909No ratings yet
- Top 5 Consumer Court CasesDocument7 pagesTop 5 Consumer Court CasesTanishka SoniNo ratings yet
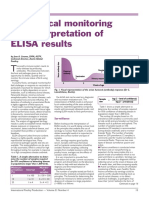
- Serological Monitoring by ELISADocument3 pagesSerological Monitoring by ELISAreza tavayef100% (1)
- BSBMKG502 Task 2Document9 pagesBSBMKG502 Task 2Diana PulidoNo ratings yet
- Psychopathic Personality: Bridging The Gap Between Scientific Evidence and Public PolicyDocument69 pagesPsychopathic Personality: Bridging The Gap Between Scientific Evidence and Public PolicyGokushimakNo ratings yet
- Breaking The Silence - Art TherapyDocument43 pagesBreaking The Silence - Art TherapyAdriana100% (1)
- CYBERBULLYINGDocument2 pagesCYBERBULLYINGAdinda CahayaNo ratings yet
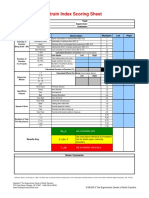
- Strain Index Scoring Sheet: Date: Task: Company: Supervisor: Dept: EvaluatorDocument1 pageStrain Index Scoring Sheet: Date: Task: Company: Supervisor: Dept: EvaluatorUdaydeep SinghNo ratings yet
- 3075 SWMS RendererDocument13 pages3075 SWMS Renderernik KooNo ratings yet
- Annexure I: Block / Building Fire Safety Audit-Check List Fire Safety Audit ChecklistDocument5 pagesAnnexure I: Block / Building Fire Safety Audit-Check List Fire Safety Audit ChecklistGaurav Singh67% (3)
- PIL For Sudafed DecongestantDocument2 pagesPIL For Sudafed DecongestantOdunlamiNo ratings yet
- Pseudostrabismus ExplainedDocument3 pagesPseudostrabismus ExplainedbebetangNo ratings yet
- Awarness About Breast CancerDocument4 pagesAwarness About Breast CancerliaahlanNo ratings yet
- T2anklearthrodesis Optech b1000044d0710Document36 pagesT2anklearthrodesis Optech b1000044d0710Alsed GjoniNo ratings yet