You might also like
- PASSMEDICINE MRCP NOTES-INFECTIOUS DISEASES AND STIsDocument112 pagesPASSMEDICINE MRCP NOTES-INFECTIOUS DISEASES AND STIsHashim Ahmad100% (5)
- MSK StaphDocument3 pagesMSK Staphعبدالرحمن عابدNo ratings yet
- Finasls 1 Staph Strep PDFDocument50 pagesFinasls 1 Staph Strep PDFFrancis ValdezNo ratings yet
- 1 - Systemic BacteriologyDocument316 pages1 - Systemic BacteriologyAlsirNo ratings yet
- Staphylococcus: Zeinab Abd Elkhalek Prof. of Medical Microbiology & ImmunologyDocument26 pagesStaphylococcus: Zeinab Abd Elkhalek Prof. of Medical Microbiology & ImmunologyMustafa SaßerNo ratings yet
- Gram Positive CocciDocument55 pagesGram Positive CocciAyat MostafaNo ratings yet
- 760 Staphylococcus PPT UG LectureDocument47 pages760 Staphylococcus PPT UG Lectureridwan.biotekNo ratings yet
- Screenshot 2021-06-04 at 23.19.29Document72 pagesScreenshot 2021-06-04 at 23.19.29Amina Mohamed AbdikeirNo ratings yet
- staplylococci محاضرة الاولىDocument20 pagesstaplylococci محاضرة الاولىArwa HussienNo ratings yet
- Gram Positive Cocci StaphylococciDocument41 pagesGram Positive Cocci StaphylococciZainab ElgehaniNo ratings yet
- Staphylococcus & StreptococcusDocument100 pagesStaphylococcus & StreptococcusFahim NadvyNo ratings yet
- Common Cause: Staphylococcus Spp. Streptococcus Spp. Enterococcus SPPDocument8 pagesCommon Cause: Staphylococcus Spp. Streptococcus Spp. Enterococcus SPPAdel mohammadNo ratings yet
- Gram +ve BacteriaDocument58 pagesGram +ve BacteriaGx NavinNo ratings yet
- Gram Positive Cocci Sem 1 1Document45 pagesGram Positive Cocci Sem 1 1Charmaine Corpuz Granil100% (1)
- Microbiology TablesDocument19 pagesMicrobiology TablesRebecca MarshallNo ratings yet
- The Staphylococci: Membranes of Humans Others Cause Suppuration, Abscess Formation, A Variety ofDocument18 pagesThe Staphylococci: Membranes of Humans Others Cause Suppuration, Abscess Formation, A Variety ofزين العابدين محمد عويش مشريNo ratings yet
- Staphylococcus Aureus: DR Surender Kaur Asst - Prof. GMCDocument22 pagesStaphylococcus Aureus: DR Surender Kaur Asst - Prof. GMCkaursurenderNo ratings yet
- Culture and IdentificationDocument4 pagesCulture and IdentificationDewa Denis100% (1)
- Piogenic Cocci: Ania Kurniawati PD, Dr. MkesDocument58 pagesPiogenic Cocci: Ania Kurniawati PD, Dr. MkesSilmi Zhillan Nur RahmanNo ratings yet
- Staphylococci & MicrococciDocument52 pagesStaphylococci & Micrococcihoneylemon.coNo ratings yet
- 1.1 Gram Positive CocciDocument9 pages1.1 Gram Positive CocciJustine Mel Concepcion IlardeNo ratings yet
- Practical 4 Staphylococci PresentationDocument24 pagesPractical 4 Staphylococci PresentationPatrisha BuanNo ratings yet
- A. Staphylococcus Aureus B. Staphylococcus Epidermidis C. Staphylococcus SaprophyticusDocument8 pagesA. Staphylococcus Aureus B. Staphylococcus Epidermidis C. Staphylococcus SaprophyticusRuel MaddawinNo ratings yet
- Special MicrobiologyDocument68 pagesSpecial MicrobiologyrefuapalackyNo ratings yet
- StaphylococcusDocument39 pagesStaphylococcus吳冠威No ratings yet
- LGT - Pyogenic Cocci - Strept - DR.S ZeinyDocument29 pagesLGT - Pyogenic Cocci - Strept - DR.S ZeinythaeonlooreNo ratings yet
- Systemic Bacriology 1Document87 pagesSystemic Bacriology 1samar yousif mohamedNo ratings yet
- Gram Positive CocciDocument140 pagesGram Positive CocciBles Cy LagrimasNo ratings yet
- CB Part 3Document76 pagesCB Part 3Mohammad MambuayNo ratings yet
- Basic MicrobiologyDocument53 pagesBasic MicrobiologyJohn NirmalNo ratings yet
- GRAM Positive CocciDocument67 pagesGRAM Positive CocciNoraine Princess TabangcoraNo ratings yet
- L1 - StaphylococciDocument35 pagesL1 - Staphylococciyouservezeropurpose113No ratings yet
- Gram Positive Cocci Genus: Staphylococcus SPPDocument9 pagesGram Positive Cocci Genus: Staphylococcus SPPعزوز الراويNo ratings yet
- Unit 4 BacteriologyDocument51 pagesUnit 4 BacteriologySharmila LamisharNo ratings yet
- Chap 13. StaphylococcusDocument40 pagesChap 13. StaphylococcusSHARON MARIA SUNNYNo ratings yet
- Staphylococcus LectureDocument27 pagesStaphylococcus LectureRalt MedNo ratings yet
- Gram Positive Cocci: Two GeneraDocument31 pagesGram Positive Cocci: Two GeneraGeorgeNecoară100% (1)
- 34 Staphylococcus - IncompleteDocument9 pages34 Staphylococcus - IncompleteHarshada GhanekarNo ratings yet
- Bacteria of Medical Importance 1Document21 pagesBacteria of Medical Importance 1Tshepang MohlahloNo ratings yet
- S. AureusDocument39 pagesS. AureusRajkishor YadavNo ratings yet
- Staph - 2020 Nov - PDocument14 pagesStaph - 2020 Nov - PHUỲNH QUỐC KHÁNHNo ratings yet
- 3.1 Staphylococci PDFDocument36 pages3.1 Staphylococci PDFWong ShuanNo ratings yet
- Gram Positive Cocci - Sem 1Document45 pagesGram Positive Cocci - Sem 1Charmaine Corpuz GranilNo ratings yet
- S. Aureus, Cons: S.Epidermidis, Cons: S.SaprophyticusDocument14 pagesS. Aureus, Cons: S.Epidermidis, Cons: S.SaprophyticusMugiNo ratings yet
- Bacteriology by Dhshan Hassan DhshanDocument48 pagesBacteriology by Dhshan Hassan Dhshanعلي الكوافي100% (1)
- Staphylococcus: Medical Faculty - Hang Tuah UniversityDocument25 pagesStaphylococcus: Medical Faculty - Hang Tuah UniversityFranciska MawuntuNo ratings yet
- Staphylococcus Aureus Infiection Thang 1 2007Document44 pagesStaphylococcus Aureus Infiection Thang 1 2007Nguyễn Tấn BìnhNo ratings yet
- Definition: Gram +ve CocciDocument45 pagesDefinition: Gram +ve Cocciliyana04_08No ratings yet
- K20 Infeksi Bakteri Pada Kulit DR DR Enny Nugraheni, M BiomedDocument38 pagesK20 Infeksi Bakteri Pada Kulit DR DR Enny Nugraheni, M BiomedFajar Cristianta GintingNo ratings yet
- Bacteriology Edited 1Document65 pagesBacteriology Edited 1Ali AhmedNo ratings yet
- Staphylococcus LectureDocument66 pagesStaphylococcus LectureFarhan Azmain FahimNo ratings yet
- Bacte Midterm (Walang Pictures)Document21 pagesBacte Midterm (Walang Pictures)AL-HUSSEIN NAWABNo ratings yet
- StaphylococcusDocument23 pagesStaphylococcussajad abasNo ratings yet
- A. Staphylococcus Aureus B. Streptococcus Pneumoniae Haemophilus Influenzae Moraxella CatarrhalisDocument26 pagesA. Staphylococcus Aureus B. Streptococcus Pneumoniae Haemophilus Influenzae Moraxella CatarrhalisMoh EidNo ratings yet
- Week 3 - Topic 1 - Demonstration of Characteristics, Lab Diagnosis & Pathogenesis of StaphylococcusDocument24 pagesWeek 3 - Topic 1 - Demonstration of Characteristics, Lab Diagnosis & Pathogenesis of StaphylococcusTayyaba TahiraNo ratings yet
- Stafilococcus (Coccus Gram Positif)Document39 pagesStafilococcus (Coccus Gram Positif)arisita firmanNo ratings yet
- Neisseria, Diph, AnthraxDocument53 pagesNeisseria, Diph, AnthraxAyat MostafaNo ratings yet
- Streptococcus SPPDocument52 pagesStreptococcus SPPdrnuaman5No ratings yet
- Bacterial Infections of The SkinDocument9 pagesBacterial Infections of The Skinbeia21No ratings yet
- All Ventricular Muscle Cells Beat at The Same Time BecauseDocument25 pagesAll Ventricular Muscle Cells Beat at The Same Time Becauseliyana04_08No ratings yet
- 2nd Year IUMP Module 13Document1 page2nd Year IUMP Module 13liyana04_08No ratings yet
- 2nd Year IUMP Module 13Document1 page2nd Year IUMP Module 13liyana04_08No ratings yet
- 2nd Year IUMP Module 13Document1 page2nd Year IUMP Module 13liyana04_08No ratings yet
- 2nd Year Iump 2010-2011 Module 13Document3 pages2nd Year Iump 2010-2011 Module 13liyana04_08No ratings yet
- End of Semester ExamDocument1 pageEnd of Semester Examliyana04_08No ratings yet
- Jar JarDocument3 pagesJar Jarliyana04_08No ratings yet
- 2nd Year IUMP Module 13Document1 page2nd Year IUMP Module 13liyana04_08No ratings yet
- ةيناثلا ةقرفلا لودج 2010 - 2011 رشع ةيناثلا ةيميلعتلا ةدحولا respiratory system عبارلا عوبسلأاDocument3 pagesةيناثلا ةقرفلا لودج 2010 - 2011 رشع ةيناثلا ةيميلعتلا ةدحولا respiratory system عبارلا عوبسلأاliyana04_08No ratings yet
- Assignment Exam For Cardiovascular ModuleDocument2 pagesAssignment Exam For Cardiovascular Moduleliyana04_08No ratings yet
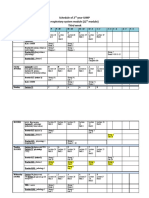
- Schedule of 2 Year IUMP Respiratory System Module (12 Module) Third WeekDocument3 pagesSchedule of 2 Year IUMP Respiratory System Module (12 Module) Third Weekliyana04_08No ratings yet
- Definition: Gram +ve CocciDocument45 pagesDefinition: Gram +ve Cocciliyana04_08No ratings yet
- Practical ExamDocument1 pagePractical Examliyana04_08No ratings yet
- Time Table Ass Cvs-1Document2 pagesTime Table Ass Cvs-1liyana04_08No ratings yet
- End of Semester Exam End of Module Exam (MCQS) Practical Assignment Subtotal Essay Mcqs 25% 25%Document1 pageEnd of Semester Exam End of Module Exam (MCQS) Practical Assignment Subtotal Essay Mcqs 25% 25%liyana04_08No ratings yet
- JARS Revisison 1st TermDocument32 pagesJARS Revisison 1st Termliyana04_08No ratings yet
- Heart SoundsDocument49 pagesHeart Soundsliyana04_08No ratings yet
- JARS Revisison 1st TermDocument32 pagesJARS Revisison 1st Termliyana04_08No ratings yet
- LifePad Cartridge IFUDocument21 pagesLifePad Cartridge IFUGuneyden GuneydenNo ratings yet
- Diagnostic Report: Patient Name: Ashwani Singh 0088UD006521 ASHWM280719800Document2 pagesDiagnostic Report: Patient Name: Ashwani Singh 0088UD006521 ASHWM280719800Ankit AgarwalNo ratings yet
- Isolation and Identification of Fungi From Fast Food Restaurants in Langa BazarDocument6 pagesIsolation and Identification of Fungi From Fast Food Restaurants in Langa BazarIJEAB JournalNo ratings yet
- Role of Child Health NurseDocument40 pagesRole of Child Health NurseBinal Joshi100% (1)
- Peritonitis and Abdominal Sepsis: Background, Anatomy, PathophysiologyDocument16 pagesPeritonitis and Abdominal Sepsis: Background, Anatomy, PathophysiologyTias SubagioNo ratings yet
- Nationally Notifiable Infectious Diseases and Conditions, United States: Annual TablesDocument5 pagesNationally Notifiable Infectious Diseases and Conditions, United States: Annual TablesgrowlingtoyouNo ratings yet
- Research Proposal Related To Coronavirus'Document15 pagesResearch Proposal Related To Coronavirus'Tasnim Lamya100% (1)
- The Medicinal Prospects of Makahiya MimoDocument6 pagesThe Medicinal Prospects of Makahiya MimoDaniel BartoloNo ratings yet
- PrioritizationDocument4 pagesPrioritizationJhennie EyescandieNo ratings yet
- Microbiology Unknown ReportDocument25 pagesMicrobiology Unknown Reportacj56100% (1)
- Objectives: General Objective: Specific ObjectivesDocument8 pagesObjectives: General Objective: Specific ObjectivesLora CarpioNo ratings yet
- J. P. Rizal Extension, West Rembo, Makati City 1215 Telephone No.: (+632) - 881 - 1571Document2 pagesJ. P. Rizal Extension, West Rembo, Makati City 1215 Telephone No.: (+632) - 881 - 1571Diane BautistaNo ratings yet
- Intro To Virology ReviewerDocument14 pagesIntro To Virology ReviewerJilianne Sablot100% (1)
- ESICM/ESCMID Task Force On Practical Management of Invasive Candidiasis in Critically Ill PatientsDocument17 pagesESICM/ESCMID Task Force On Practical Management of Invasive Candidiasis in Critically Ill PatientsrennerrsNo ratings yet
- Library G.Pulla Reddy College of Pharmacy Hyderabad: Second YearDocument16 pagesLibrary G.Pulla Reddy College of Pharmacy Hyderabad: Second YeardeepuNo ratings yet
- Hepatitis C SlidesDocument51 pagesHepatitis C SlidesChukwu NedumNo ratings yet
- Communicable Disease ReviewDocument7 pagesCommunicable Disease Reviewjudith dela cruzNo ratings yet
- Microorganisms Friend and FoeDocument7 pagesMicroorganisms Friend and FoeIlayarajaNo ratings yet
- Campeel IutDocument86 pagesCampeel IutRosa TorresNo ratings yet
- NCPDocument4 pagesNCPRachel PerandoNo ratings yet
- NCM 106 AntibacterialDocument11 pagesNCM 106 AntibacterialBruno, Kurt Andrei V.No ratings yet
- IMPETIGODocument10 pagesIMPETIGOafifulichwan18No ratings yet
- HLTINF006 Student Assessment Task 1 - 16252 - Rebeca RaducuDocument10 pagesHLTINF006 Student Assessment Task 1 - 16252 - Rebeca RaducuRebeca RaducuNo ratings yet
- Epidemiological SurveillanceDocument22 pagesEpidemiological SurveillanceSyafiq HusniNo ratings yet
- Ssi PDFDocument29 pagesSsi PDFKaterina NahampunNo ratings yet
- Colega Walter C Bsais2a MWF 12 1pmDocument15 pagesColega Walter C Bsais2a MWF 12 1pmWalter CauanNo ratings yet
- Science Technology SocietyDocument21 pagesScience Technology SocietyJesseca Luntaga Belza100% (1)
- Germ Theory MiasmDocument28 pagesGerm Theory MiasmDr. Bhumika NarvaneNo ratings yet
- Catalogo General de Productos Stratec MolecularDocument44 pagesCatalogo General de Productos Stratec MolecularyudycantNo ratings yet
- Expanded Program On Immunization (EPI) 7 Vaccine-Preventable Diseases VaccinesDocument7 pagesExpanded Program On Immunization (EPI) 7 Vaccine-Preventable Diseases VaccinesLuiciaNo ratings yet