You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Rib FractureDocument69 pagesRib FractureAlfina Aulia RizkiNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Ikm TBDocument72 pagesIkm TBAlfina Aulia RizkiNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Respiratory Disorders: Pleural and Thoracic InjuryDocument34 pagesRespiratory Disorders: Pleural and Thoracic InjuryAlfina Aulia RizkiNo ratings yet
- Efusi Pleura TBDocument35 pagesEfusi Pleura TBAlfina Aulia RizkiNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Mycoplasma and UreaplasmaDocument20 pagesMycoplasma and UreaplasmaAlfina Aulia RizkiNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
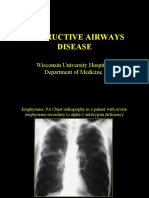
- Obstructive Airways Disease: Wisconsin University Hospital. Department of MedicineDocument27 pagesObstructive Airways Disease: Wisconsin University Hospital. Department of MedicineAlfina Aulia RizkiNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Dosennya DR Sauqi - Neurokrin Sp2 PT Fer1 NewDocument136 pagesDosennya DR Sauqi - Neurokrin Sp2 PT Fer1 NewAlfina Aulia RizkiNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Committee On Trauma Presents: Thermal InjuriesDocument35 pagesCommittee On Trauma Presents: Thermal InjuriesAlfina Aulia RizkiNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Thyroid CADocument63 pagesThyroid CAAlfina Aulia RizkiNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- House KeepingDocument23 pagesHouse KeepingAlfina Aulia RizkiNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Seminar Presented By: DR Himanshu Rana (JR-3) : History Taking and General Examination of Respiratory SystemDocument48 pagesSeminar Presented By: DR Himanshu Rana (JR-3) : History Taking and General Examination of Respiratory SystemAlfina Aulia RizkiNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Meniere DiseaseDocument15 pagesMeniere DiseaseAlfina Aulia RizkiNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- General Physical Assessment: C. Richard Finley, Ed.D, PA-CDocument56 pagesGeneral Physical Assessment: C. Richard Finley, Ed.D, PA-CAlfina Aulia RizkiNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Hydrotherapy Indi ContraDocument71 pagesHydrotherapy Indi Contrateam7MFkkOP YTNo ratings yet
- Nervous System AlterationsDocument34 pagesNervous System Alterationsmiekot15No ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- NCP - ERDocument5 pagesNCP - ERAnnelore ArcayNo ratings yet
- DONOR SELECTION (Deferral) - BBDocument5 pagesDONOR SELECTION (Deferral) - BBMaikka IlaganNo ratings yet
- Geriatric OtolaryngologyDocument26 pagesGeriatric OtolaryngologySari RakhmawatiNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Thyroid Function Blood TestsDocument5 pagesThyroid Function Blood TestsCassandra ColigadoNo ratings yet
- Herpes Zoster PDFDocument19 pagesHerpes Zoster PDFNicolás LaverdeNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Cervical DystociaDocument22 pagesCervical DystociaBaldau TiwariNo ratings yet
- DR - Thompsons CBC-RBC Indices Guide - A Guide To Red Blood Cell IndicesDocument54 pagesDR - Thompsons CBC-RBC Indices Guide - A Guide To Red Blood Cell IndicesYohana SetiawanNo ratings yet
- Toronto Notes - Cardiac SurgeryDocument32 pagesToronto Notes - Cardiac Surgerymicielij100% (1)
- EmergencyDocument7 pagesEmergencymedodiabNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Amisulprid 2Document5 pagesAmisulprid 2Robert MovileanuNo ratings yet
- CH 084 Oral ThrushDocument7 pagesCH 084 Oral ThrushSavir GuptaNo ratings yet
- Motor and Sensory Examination: Dr. Bandar Al Jafen, MD Consultant NeurologistDocument36 pagesMotor and Sensory Examination: Dr. Bandar Al Jafen, MD Consultant NeurologistJim Jose Antony100% (1)
- Holoxan Pi PDFDocument18 pagesHoloxan Pi PDFKarol IonasNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Dengue Fever EngDocument17 pagesDengue Fever EngRia Tustina HendrayaniNo ratings yet
- APA Formatted Paper Handout-APA 7eDocument3 pagesAPA Formatted Paper Handout-APA 7eOscar QuispeNo ratings yet
- Treatment of Hemophilia A and B PDFDocument268 pagesTreatment of Hemophilia A and B PDFYusry SuryawiraNo ratings yet
- August Complete (Compressed)Document447 pagesAugust Complete (Compressed)Dr-Qazi Ejaz AhmadNo ratings yet
- All India Ayush Post Graduate Entrance Test 2019 Question PaperDocument24 pagesAll India Ayush Post Graduate Entrance Test 2019 Question PaperSoumitra BoseNo ratings yet
- Notes by Dr. Khurram PDFDocument22 pagesNotes by Dr. Khurram PDFAdnan AsgharNo ratings yet
- Moduleiii:Summativeevaluation: Pheochromocytoma. (2020) - N Ational Library of M EdicineDocument1 pageModuleiii:Summativeevaluation: Pheochromocytoma. (2020) - N Ational Library of M EdicineKashley DangliNo ratings yet
- Hypoglycemia in Adults Clinical Manifestations, Definition, and CausesDocument1 pageHypoglycemia in Adults Clinical Manifestations, Definition, and CausesnovaNo ratings yet
- Hypertensive Disorder in PregnancyDocument5 pagesHypertensive Disorder in Pregnancymendato marcabanNo ratings yet
- 327-Differential Diagnosis of SEIZURE - SattawutDocument44 pages327-Differential Diagnosis of SEIZURE - Sattawutyusma wati99No ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- KSC WSSforKSCCQIDocument34 pagesKSC WSSforKSCCQILệnhHồXungNo ratings yet
- Diagnostic Exam Level 4Document83 pagesDiagnostic Exam Level 4cianm1143No ratings yet
- Identifikasi Risiko Musculoskeletal Disorders (MSDS) Pada Pekerja Pandai BesiDocument10 pagesIdentifikasi Risiko Musculoskeletal Disorders (MSDS) Pada Pekerja Pandai BesiTito MuharamNo ratings yet
- Cumulative Trauma DisordersDocument5 pagesCumulative Trauma Disordersravinaj21100% (1)
- Drugs Affecting Coagulation ObjectivesDocument14 pagesDrugs Affecting Coagulation ObjectiveslouradelNo ratings yet