You might also like
- Examination of Orthopedic Athletic Injuries 4th Edition Starkey Test BankDocument13 pagesExamination of Orthopedic Athletic Injuries 4th Edition Starkey Test Bankvictoriawaterswkdxafcioq100% (13)
- Hotel LeadsDocument17 pagesHotel Leadssanakausar.5089No ratings yet
- The PFC MatrixDocument1 pageThe PFC MatrixBryan Elvambuena100% (4)
- 12a Diabetic Emergencies DKA Case StudiesDocument13 pages12a Diabetic Emergencies DKA Case StudiesAnonymous yTdBi7100% (1)
- Camba-Course Task 4Document5 pagesCamba-Course Task 4Rachelle CambaNo ratings yet
- PacuDocument24 pagesPacuLamtioma GultomNo ratings yet
- Transcript of Pain Control Processes - Richard NongardDocument49 pagesTranscript of Pain Control Processes - Richard Nongardguacamoledip100% (2)
- Updated Dental Clinics 07 17 2013 PDFDocument11 pagesUpdated Dental Clinics 07 17 2013 PDFGames NathanNo ratings yet
- ICP AlgorithmDocument1 pageICP AlgorithmAngel Princëzza LovërzNo ratings yet
- Census - High SpinalDocument30 pagesCensus - High SpinalBhi-An BatobalonosNo ratings yet
- A1 CBLDocument59 pagesA1 CBLEbtesamNo ratings yet
- Acute Coronary SyndromeDocument7 pagesAcute Coronary SyndromePuskesmas Pinang JayaNo ratings yet
- A1 CBLDocument59 pagesA1 CBLEbtesamNo ratings yet
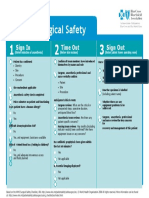
- Surgical Safety: Sign in Time Out Sign OutDocument1 pageSurgical Safety: Sign in Time Out Sign OutNathanNo ratings yet
- Peptic Ulcer Concept MapDocument17 pagesPeptic Ulcer Concept Mappotchistroberri100% (1)
- Worksheets - Isbar 3 StrokeDocument3 pagesWorksheets - Isbar 3 Strokeapi-673621869No ratings yet
- COVID Patient Result: AUGUST 3, 2021Document3 pagesCOVID Patient Result: AUGUST 3, 2021Toff GoyenecheaNo ratings yet
- Worksheets - Isbar 1Document3 pagesWorksheets - Isbar 1api-673621869No ratings yet
- SISS - Evaluation of Pediatric Abdominal Pain and ImagingDocument4 pagesSISS - Evaluation of Pediatric Abdominal Pain and ImagingPrincyNo ratings yet
- Morbidity April 2022: Aileen Concepcion M. AgustinDocument24 pagesMorbidity April 2022: Aileen Concepcion M. AgustinConcepcion R. AquinoNo ratings yet
- Surgery Revision E6.5 @TheBoggusdocDocument242 pagesSurgery Revision E6.5 @TheBoggusdocShubham ShandilyaNo ratings yet
- 12-Adult Post Resuscitation Care Algorithm 2021Document1 page12-Adult Post Resuscitation Care Algorithm 2021khaledNo ratings yet
- Reporting For Seminar 1Document41 pagesReporting For Seminar 1Aby MauanayNo ratings yet
- Laporan 1Document7 pagesLaporan 1ksm bedahNo ratings yet
- No Identity Admission To E.R. Diagnosis Treatment: Treatment From Brigjen H. Hasan Basry Kandangan HospitalDocument14 pagesNo Identity Admission To E.R. Diagnosis Treatment: Treatment From Brigjen H. Hasan Basry Kandangan HospitalDewi AngginiNo ratings yet
- ElectrodiagnosticsDocument4 pagesElectrodiagnosticsAndy Delos ReyesNo ratings yet
- Mrs. A, 35 Years Old, MR 01 13 45 74, Severity Level IIIDocument18 pagesMrs. A, 35 Years Old, MR 01 13 45 74, Severity Level IIIprimaindra27No ratings yet
- Diara Jossiean M. Rogacion: Clinical Clerk 2020-2021 Group 5B Department of MedicineDocument19 pagesDiara Jossiean M. Rogacion: Clinical Clerk 2020-2021 Group 5B Department of MedicineJara RogacionNo ratings yet
- Grand Rounds: Roxanne Jeen L. Fornolles, M.DDocument61 pagesGrand Rounds: Roxanne Jeen L. Fornolles, M.DRj FornollesNo ratings yet
- 7.2post Resus Algorithms 1Document1 page7.2post Resus Algorithms 1abrar risandiNo ratings yet
- NCP For PCAPCDocument6 pagesNCP For PCAPCEnrique Lu100% (1)
- 7.2post Resus Algorithms 1Document1 page7.2post Resus Algorithms 1Massimo Di BenedettoNo ratings yet
- CPR PosterDocument1 pageCPR PosterHemantNo ratings yet
- Algorithms of AHA 2020Document23 pagesAlgorithms of AHA 2020Emirhan llkhanNo ratings yet
- Screenshot 2024-03-29 at 20.24.01Document12 pagesScreenshot 2024-03-29 at 20.24.01hennywahyuni363No ratings yet
- Society For Obesity and Bariatric Anaesthesia: OS-MRS Calculator Tools - Farmacologiaclinica.infoDocument1 pageSociety For Obesity and Bariatric Anaesthesia: OS-MRS Calculator Tools - Farmacologiaclinica.infoHizami Norddin100% (2)
- Biomol Tranduksi Sinyal Presentasi Kelompok Komunikasi SelDocument23 pagesBiomol Tranduksi Sinyal Presentasi Kelompok Komunikasi SelAgus SGNo ratings yet
- Case - ViedyaDocument40 pagesCase - ViedyaRaka WibisonoNo ratings yet
- ICP Management Guideline Adult January 2017Document20 pagesICP Management Guideline Adult January 2017syhsyhsyh123No ratings yet
- (ANES) Mon 01 Epidural For Labor Analgesia (A2021)Document3 pages(ANES) Mon 01 Epidural For Labor Analgesia (A2021)Miguel SantosNo ratings yet
- Veterinary Technician Skills - Mastered - KimtierneyDocument1 pageVeterinary Technician Skills - Mastered - Kimtierneyapi-207993624No ratings yet
- 2-Cardiac Arrest AlgrthmDocument1 page2-Cardiac Arrest AlgrthmterminallllNo ratings yet
- Ny IsDocument15 pagesNy IsAuliaNo ratings yet
- Morning Report 1st of March 2023Document23 pagesMorning Report 1st of March 2023mita sanjayaNo ratings yet
- Case StudyDocument16 pagesCase StudyArmand Bong Santiago100% (1)
- Overview and Assessment of Balance Functions: Electronystagmography/ VideonystagmographyDocument48 pagesOverview and Assessment of Balance Functions: Electronystagmography/ VideonystagmographyArun KumarNo ratings yet
- Beverly Sze - Case Study 2Document9 pagesBeverly Sze - Case Study 2christyl necesitoNo ratings yet
- Special Laboratory and Diagnostic TestsDocument75 pagesSpecial Laboratory and Diagnostic TestskrismaevelNo ratings yet
- NCP, FHP, and Pharma Card of Patient R.K. With Myocardial InfarctionDocument21 pagesNCP, FHP, and Pharma Card of Patient R.K. With Myocardial InfarctionJoi Owen Yap TevesNo ratings yet
- 2020 Acls Megacode Testing Scenarios - 2Document13 pages2020 Acls Megacode Testing Scenarios - 2Dr. Saqib RazaNo ratings yet
- Assessment 2 FormattedDocument1 pageAssessment 2 FormattedAmbika SuwalNo ratings yet
- Follow Up LidiawatiDocument6 pagesFollow Up LidiawatiellafinarsihNo ratings yet
- POSToperative 3Document6 pagesPOSToperative 3joanneNo ratings yet
- Case Presentati On: Sevilla, Loreanne Novem Silim, Miriam Grace DDocument28 pagesCase Presentati On: Sevilla, Loreanne Novem Silim, Miriam Grace DKen StarNo ratings yet
- Snake BiteDocument62 pagesSnake Bitelailatul husnaNo ratings yet
- Acls - MegacodeDocument11 pagesAcls - MegacodeEllen Joyce FlorNo ratings yet
- Microsoft Word Cardiac Medications 1231855169882073 2Document1 pageMicrosoft Word Cardiac Medications 1231855169882073 2api-19824701No ratings yet
- Enteral and Parental NutritionDocument3 pagesEnteral and Parental Nutritionpulmano.cf65No ratings yet
- Diagnostic EvaluationDocument29 pagesDiagnostic EvaluationJaylord VerazonNo ratings yet
- Transoperative 812217287Document27 pagesTransoperative 812217287Pepe PeñaNo ratings yet
- 05 - 26 - 22 TahbsoDocument29 pages05 - 26 - 22 TahbsoMa. Therese GarganianNo ratings yet
- Endorsement of Aling AnnaDocument2 pagesEndorsement of Aling AnnaTom CuencaNo ratings yet
- Stroke Drug Study (GROUP)Document8 pagesStroke Drug Study (GROUP)Fran LanNo ratings yet
- Clinical Diabetes Research: Methods and TechniquesFrom EverandClinical Diabetes Research: Methods and TechniquesMichael RodenNo ratings yet
- Syncope CasesFrom EverandSyncope CasesRoberto García-CiveraNo ratings yet
- DiplomDiplomaCourseProspectus PDFDocument17 pagesDiplomDiplomaCourseProspectus PDFShishir Kumar Singh0% (1)
- The Pediatric Physical Exam:: Who, When, What and Why?Document26 pagesThe Pediatric Physical Exam:: Who, When, What and Why?Carlo Emmanuel SantosNo ratings yet
- REG ETA-IMG-038 Assessing A SIMGs Comparability To An ANZ Trained Surgical Specialist PDFDocument14 pagesREG ETA-IMG-038 Assessing A SIMGs Comparability To An ANZ Trained Surgical Specialist PDFGHAPRC RUDRAPURNo ratings yet
- Evaluation and Management of HematuriaDocument12 pagesEvaluation and Management of HematuriaCarlos Daniel CruzNo ratings yet
- Farmakoterapi Osteoporosis: Suharti K Suherman Dept. Farmakologi & Terapeutik FkuiDocument23 pagesFarmakoterapi Osteoporosis: Suharti K Suherman Dept. Farmakologi & Terapeutik FkuimeldrewbNo ratings yet
- Ao2021-0066 Guidelines Cert of Inclusion Blood Services NetworkDocument17 pagesAo2021-0066 Guidelines Cert of Inclusion Blood Services NetworkMic BNo ratings yet
- Allergy Test PapersDocument5 pagesAllergy Test PapersDaniel MoncadaNo ratings yet
- Diverticular Disease: John P. Welch, MD, FACS, and Jeffrey L. Cohen, MD, FACS, FASCRSDocument32 pagesDiverticular Disease: John P. Welch, MD, FACS, and Jeffrey L. Cohen, MD, FACS, FASCRSDiego Andres VasquezNo ratings yet
- Dharam Pani Pandey, Dr. Uday Shankar Sharma, Dr. Ram Babu. Electrical Muscle Stimulation (EMS) Improve Functional Independence in Critically Ill PatientsDocument8 pagesDharam Pani Pandey, Dr. Uday Shankar Sharma, Dr. Ram Babu. Electrical Muscle Stimulation (EMS) Improve Functional Independence in Critically Ill PatientsDr. Krishna N. SharmaNo ratings yet
- Pain Pathways IntroductionDocument7 pagesPain Pathways Introductionganpur01100% (1)
- Cholera in Sarawak: A Historical: Erspective (1873-1989)Document8 pagesCholera in Sarawak: A Historical: Erspective (1873-1989)Jasmin Norhasfitri Muhammad NorNo ratings yet
- Nurse Resume Masters Degree TemplateDocument2 pagesNurse Resume Masters Degree TemplatehenryodomNo ratings yet
- Interview Question Clinical TrialsDocument20 pagesInterview Question Clinical Trialshruday100% (3)
- Expertddx Chest 2Nd Edition Edition Brett W Carter Full ChapterDocument67 pagesExpertddx Chest 2Nd Edition Edition Brett W Carter Full Chapterpatrick.avenoso641100% (2)
- Alterations in VentilationDocument10 pagesAlterations in VentilationCharisma Pastor100% (1)
- Classics in The History of PsychologyDocument15 pagesClassics in The History of PsychologyDaniel MogollonNo ratings yet
- HMR TemplateDocument2 pagesHMR TemplatepharmacisticusNo ratings yet
- Pcol Quiz 1Document11 pagesPcol Quiz 1SmartieNo ratings yet
- Organ DonorDocument6 pagesOrgan DonorAlexandra ZaporozhetsNo ratings yet
- Reanna Bell Surgery Observsation 1Document2 pagesReanna Bell Surgery Observsation 1api-593123385No ratings yet
- Vertesi - The Use of Frequency V1Document654 pagesVertesi - The Use of Frequency V1Ekiskalibur NirvanaNo ratings yet
- AbortionDocument14 pagesAbortionmesseeeNo ratings yet
- IOS - Interpretation and Practical Applications - CHESTDocument7 pagesIOS - Interpretation and Practical Applications - CHESTthiago gibsonNo ratings yet
- Electro-Chemiluminescence Immunoassay (ECLIA) For The Quantitative Determination of CEA in Human Serum and PlasmaDocument2 pagesElectro-Chemiluminescence Immunoassay (ECLIA) For The Quantitative Determination of CEA in Human Serum and Plasmamaricela carmen te desea lo mejorNo ratings yet
- Adhd Symptom VisualizerDocument12 pagesAdhd Symptom Visualizerandrea97murciaNo ratings yet