You might also like
- Healing CodesDocument26 pagesHealing CodesPurvi100% (1)
- Overcoming CandidaDocument76 pagesOvercoming CandidaXronia Polla100% (4)
- Dr. Nilukshi Perera Consultant HaematologistDocument128 pagesDr. Nilukshi Perera Consultant HaematologistThaveeshaLindsayWhiteNo ratings yet
- ANTI AGING Dethrone Aging With Royal JellyDocument3 pagesANTI AGING Dethrone Aging With Royal Jellywhsprz100% (1)
- DR - Ashiq Tutorials Krok2 Hygiene BaseDocument47 pagesDR - Ashiq Tutorials Krok2 Hygiene Basev.stephenson headNo ratings yet
- Cancer Pain - Clinical Pain ManagementDocument464 pagesCancer Pain - Clinical Pain Managementzahir_jasNo ratings yet
- DR Nilukshi Perera Consultant HaematologistDocument68 pagesDR Nilukshi Perera Consultant HaematologistThaveeshaLindsayWhiteNo ratings yet
- Disorders of White Blood Cells and Lymphoid TissuesDocument30 pagesDisorders of White Blood Cells and Lymphoid Tissuesammar amerNo ratings yet
- LymphomaDocument78 pagesLymphomaastriwahyuni100% (4)
- Megaloblastic and Other Macrocytic Anaemia: Dr. Nilukshi Perera Consultant HaematologistDocument58 pagesMegaloblastic and Other Macrocytic Anaemia: Dr. Nilukshi Perera Consultant HaematologistThaveeshaLindsayWhiteNo ratings yet
- Acute Leukaemias: DR Nilukshi Perera Consultant HaematologistDocument60 pagesAcute Leukaemias: DR Nilukshi Perera Consultant HaematologistThaveeshaLindsayWhite100% (2)
- Acute Leukaemia: DR Afshan SumeraDocument37 pagesAcute Leukaemia: DR Afshan SumeraDineish MurugaiahNo ratings yet
- Lymphoma (Ean's) - 2Document29 pagesLymphoma (Ean's) - 2eanfital11No ratings yet
- Xyngular Ingredient BenefitsDocument18 pagesXyngular Ingredient BenefitsAnthony RodriguezNo ratings yet
- NHL Nandu CopasDocument95 pagesNHL Nandu CopaswihelminaNo ratings yet
- Lymphoid NeoplasmsDocument52 pagesLymphoid NeoplasmsAmalia Riska GNo ratings yet
- Diseases and Tumors of Lymphoid SystemDocument97 pagesDiseases and Tumors of Lymphoid SystemamyNo ratings yet
- Limfoma Maligna FinalDocument50 pagesLimfoma Maligna FinalAulia Ayu PuspitaNo ratings yet
- A Pattern Based Approach To Nodal Lymphoma: The Critical Role of HistologyDocument55 pagesA Pattern Based Approach To Nodal Lymphoma: The Critical Role of Histologylazy19No ratings yet
- Cancerul Mamar - GeneralitatiDocument60 pagesCancerul Mamar - GeneralitatiPopa MihaiNo ratings yet
- Understanding Hodgkin Lymphoma. A Guide For Patients, Survivors, and Loved Ones. October 2017From EverandUnderstanding Hodgkin Lymphoma. A Guide For Patients, Survivors, and Loved Ones. October 2017No ratings yet
- Non-Hodgkin'S Lymphoma: Oliveros Francis!!!!!!!!!!!!!!!!!Document48 pagesNon-Hodgkin'S Lymphoma: Oliveros Francis!!!!!!!!!!!!!!!!!francis00090No ratings yet
- Lymphoma: Pro - Dr.Ahmed EisaDocument45 pagesLymphoma: Pro - Dr.Ahmed EisaOmar Mohammed100% (1)
- Fast Facts: Leukemia: From initial gene mutation to survivorship supportFrom EverandFast Facts: Leukemia: From initial gene mutation to survivorship supportNo ratings yet
- Diagnosis Kanker Paru AzDocument20 pagesDiagnosis Kanker Paru AzTryanda SaidNo ratings yet
- LHYMPHOMADocument24 pagesLHYMPHOMACryptic LadyNo ratings yet
- Lymphoma: David Lee MD, FRCPCDocument36 pagesLymphoma: David Lee MD, FRCPCQasim AliNo ratings yet
- Blockxiv Neoplasms Lymphoid 2006Document54 pagesBlockxiv Neoplasms Lymphoid 2006Ryo RyozNo ratings yet
- Acute LeukaemiaDocument39 pagesAcute LeukaemiaAbby LiewNo ratings yet
- 1 - Lymphomas - Gelinde NarekineDocument64 pages1 - Lymphomas - Gelinde NarekineAntna SinekNo ratings yet
- Lymphoma: An Overview: DR Louise Connell 05/03/2103Document66 pagesLymphoma: An Overview: DR Louise Connell 05/03/2103Dodo Saputera Damian100% (1)
- Boala HodgkinDocument44 pagesBoala HodgkinCristina BuzatuNo ratings yet
- Hematopathlogy 2Document87 pagesHematopathlogy 2evansmando12No ratings yet
- Week 15-Mature-Lymphoid-Neoplasms-SCDocument65 pagesWeek 15-Mature-Lymphoid-Neoplasms-SCKyle CollladoNo ratings yet
- PATHO LEC WBC Lymph Nodes Spleen Thymus Part1 CompressedDocument84 pagesPATHO LEC WBC Lymph Nodes Spleen Thymus Part1 CompressedAngelo HinonNo ratings yet
- Lymphoma CancerDocument34 pagesLymphoma CancerwasihaiderkNo ratings yet
- Lymphoreticular FinalDocument42 pagesLymphoreticular FinalNafis Fuad SheikhNo ratings yet
- Pathology of NHL, Part 1 For 2nd Year Medical StudentDocument28 pagesPathology of NHL, Part 1 For 2nd Year Medical Studentmina mounirNo ratings yet
- Acute Leukemia: David Lee, MD, FRCPCDocument31 pagesAcute Leukemia: David Lee, MD, FRCPCfranzzjosefNo ratings yet
- Non Hodgkin Lymphoma by Dr. AnumDocument43 pagesNon Hodgkin Lymphoma by Dr. AnumHumar HaiderNo ratings yet
- LymphomaDocument69 pagesLymphomaDawit g/kidanNo ratings yet
- Haematology-Pdf - 1Document91 pagesHaematology-Pdf - 1shreyNo ratings yet
- Genevieve Crane - Approach To Lymph Node-Path Cast Lymph Node Pathology Eve CraneDocument75 pagesGenevieve Crane - Approach To Lymph Node-Path Cast Lymph Node Pathology Eve CraneJose SirittNo ratings yet
- Lymphoma 101Document44 pagesLymphoma 101Muhammad SaeedNo ratings yet
- 4b TUMOR JAR RetikuloendotelialAAADocument98 pages4b TUMOR JAR RetikuloendotelialAAARyo RyozNo ratings yet
- NHL 1Document13 pagesNHL 1kushalNo ratings yet
- LNs HNDocument190 pagesLNs HNNinna Isabel VictorioNo ratings yet
- Curs5 Hematologie AnvDocument59 pagesCurs5 Hematologie AnvRaluca PăunaNo ratings yet
- Prof. Dr. Gamal Abdul Hamid University of AdenDocument95 pagesProf. Dr. Gamal Abdul Hamid University of AdenAarpit PatwaNo ratings yet
- Keganasan Pada HematologiDocument12 pagesKeganasan Pada Hematologi'Ilham Malda'No ratings yet
- Lymphomas: Dr. Y.A. AdelabuDocument28 pagesLymphomas: Dr. Y.A. Adelabuadamu mohammadNo ratings yet
- Hodgkin'S Disease AND Non-Hodgkin'S LymphomaDocument42 pagesHodgkin'S Disease AND Non-Hodgkin'S LymphomaRayya TriandaNo ratings yet
- NHL FK UnimalDocument46 pagesNHL FK UnimalicaNo ratings yet
- Non-Hodgkins LymphomaDocument22 pagesNon-Hodgkins LymphomaNyoman TapayanaNo ratings yet
- Non - Hodgkin LymphomaDocument25 pagesNon - Hodgkin LymphomaRo RyNo ratings yet
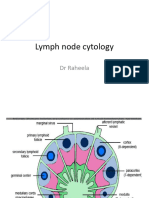
- Lymph Node CytologyDocument39 pagesLymph Node Cytologykamranghani641No ratings yet
- C6.1clasificare LimfoameDocument10 pagesC6.1clasificare LimfoameRădulescu AndreeaNo ratings yet
- Hodgkin Lymphoma: Dr. G Sirisha M.D Assistant Professor Department of Pathology, GMC, SrikakulamDocument41 pagesHodgkin Lymphoma: Dr. G Sirisha M.D Assistant Professor Department of Pathology, GMC, SrikakulamDevisriNo ratings yet
- (KULIAH) LimfomaDocument12 pages(KULIAH) Limfoma'Ilham Malda'No ratings yet
- Pathology of Lymph Nodes: Norman Levy, MDDocument92 pagesPathology of Lymph Nodes: Norman Levy, MDAdi ParamarthaNo ratings yet
- 11 Hematological MalignanciesDocument34 pages11 Hematological MalignanciesalitahawarbarintNo ratings yet
- Hodgkein and Nonhodgkein LymphomaDocument57 pagesHodgkein and Nonhodgkein Lymphomasamar yousif mohamedNo ratings yet
- Lymphoid NeoplasmsDocument39 pagesLymphoid NeoplasmsMoshe GiftNo ratings yet
- LymphomaDocument46 pagesLymphomashapan biswaNo ratings yet
- Leukocytes White Blood CellsDocument64 pagesLeukocytes White Blood CellsNevin BhunjunNo ratings yet
- LymphomasDocument50 pagesLymphomasgzrgythpyjNo ratings yet
- NHL Arshad KhanDocument30 pagesNHL Arshad KhanArshad khanNo ratings yet
- WBC DisordersDocument45 pagesWBC DisordersyalahopaNo ratings yet
- Overview of LymphomaDocument42 pagesOverview of Lymphomaadamu mohammadNo ratings yet
- Acute Leukemia: Dimas Bayu Tutik Harjianti A. FachruddinDocument41 pagesAcute Leukemia: Dimas Bayu Tutik Harjianti A. FachruddinFI 034 Mega Rahmawati MaulanaNo ratings yet
- European Day of The Prevention of The Cardiovascular Risk by SlidesgoDocument76 pagesEuropean Day of The Prevention of The Cardiovascular Risk by Slidesgobinojdaniel17No ratings yet
- NHLDocument35 pagesNHLnn zelaNo ratings yet
- 3-T and Sicke Cell Disease 2016Document68 pages3-T and Sicke Cell Disease 2016ThaveeshaLindsayWhiteNo ratings yet
- Benign WBC Disorders: Dr. Nilukshi Perera Consultant HematologistDocument31 pagesBenign WBC Disorders: Dr. Nilukshi Perera Consultant HematologistThaveeshaLindsayWhiteNo ratings yet
- English Specimen Paper 1 2018Document8 pagesEnglish Specimen Paper 1 2018ThaveeshaLindsayWhiteNo ratings yet
- 2 Mercaptobenzothiazole ToxicologyDocument175 pages2 Mercaptobenzothiazole ToxicologyRuoting PengNo ratings yet
- Cell TherapyDocument5 pagesCell Therapyayari samiNo ratings yet
- Actualización en El Manejo Médico Del Cáncer de Cérvix Recurrente - Bradley MonkDocument35 pagesActualización en El Manejo Médico Del Cáncer de Cérvix Recurrente - Bradley Monkinfo7615No ratings yet
- Biological Activities of Curcuminoids, Other Biomolecules From Turmeric and Their Derivatives e A ReviewDocument29 pagesBiological Activities of Curcuminoids, Other Biomolecules From Turmeric and Their Derivatives e A ReviewRigotti BrNo ratings yet
- Malignant and Benign Breast Cancer Classification Using Machine Learning AlgorithmsDocument5 pagesMalignant and Benign Breast Cancer Classification Using Machine Learning AlgorithmsRohit SinghNo ratings yet
- The Navarro Urine TestDocument3 pagesThe Navarro Urine TestSalvator2000100% (2)
- All Topics - 2008-2011 - ADocument37 pagesAll Topics - 2008-2011 - ADebangshu KumarNo ratings yet
- Measuring Disease and Exposure: Key Aspects of EpidemiologyDocument30 pagesMeasuring Disease and Exposure: Key Aspects of EpidemiologyUlfaNo ratings yet
- Low Peh Hueh International Medical University, MalaysiaDocument19 pagesLow Peh Hueh International Medical University, MalaysiaChaitanya Venkata SattiNo ratings yet
- Evs MCQ BankDocument25 pagesEvs MCQ BankSahil MehtaNo ratings yet
- Grupo NG Mga Adik Sa MarijuanaDocument5 pagesGrupo NG Mga Adik Sa MarijuanaAnonymous MUgicb7VytNo ratings yet
- Antoine Priore - US Patent # 3,280,816, Method of Producing Radiations For Penetrating Living CellsDocument15 pagesAntoine Priore - US Patent # 3,280,816, Method of Producing Radiations For Penetrating Living CellsoscarnineNo ratings yet
- 155 (Milla, Sara)Document24 pages155 (Milla, Sara)Nourma Kusuma WinawanNo ratings yet
- 10 11648 J Ijmi 20170505 12Document5 pages10 11648 J Ijmi 20170505 12Anchit AggarwalNo ratings yet
- Breast Cancer Pathology Fact SheetDocument6 pagesBreast Cancer Pathology Fact SheetBallisticsNo ratings yet
- Fungal Beta-Glucans As Adjuvants For Treating Cancer Patients - Revisão Sistemática de ECRDocument10 pagesFungal Beta-Glucans As Adjuvants For Treating Cancer Patients - Revisão Sistemática de ECRMaria Vitória Cota de AbreuNo ratings yet
- QB BT PDFDocument505 pagesQB BT PDFنيزو اسوNo ratings yet
- Lay LanguageDocument14 pagesLay LanguageOsama AldahamshehNo ratings yet
- Guided Imagery Literature Review: Ó 2018 Regents of The University of Minnesota. All Rights ReservedDocument13 pagesGuided Imagery Literature Review: Ó 2018 Regents of The University of Minnesota. All Rights ReservedN. SivaNo ratings yet
- Case Study 1.1. The Nurse Who Told A Lie: Did The Nurse Do The Right Thing? Was The Doctor's Advice Good Advice?Document12 pagesCase Study 1.1. The Nurse Who Told A Lie: Did The Nurse Do The Right Thing? Was The Doctor's Advice Good Advice?Payal NaiduNo ratings yet
- الدعم الاجتماعي المدرك لدى مريضات سرطان الثدي في ضوء بعض المتغيرات المجلة الاردنيةDocument16 pagesالدعم الاجتماعي المدرك لدى مريضات سرطان الثدي في ضوء بعض المتغيرات المجلة الاردنيةMohamed BelhadefNo ratings yet