You might also like
- A Study of the Lack of Hiv/Aids Awareness Among African American Women: a Leadership Perspective: Awareness That All Cultures Should Know AboutFrom EverandA Study of the Lack of Hiv/Aids Awareness Among African American Women: a Leadership Perspective: Awareness That All Cultures Should Know AboutRating: 5 out of 5 stars5/5 (1)
- Study Designs in EpidemiologyDocument34 pagesStudy Designs in EpidemiologyPawan BaraiNo ratings yet
- Descriptive Epidemiology: Submitted by Nirmal Varghese KDocument26 pagesDescriptive Epidemiology: Submitted by Nirmal Varghese KHAMID100% (1)
- Cohort StudyDocument37 pagesCohort Studygilbert2691No ratings yet
- 1-Introduction To EpidemiologyDocument22 pages1-Introduction To EpidemiologyANTHONY KHAOYANo ratings yet
- Parametric Vs Non Parametric StatisticsDocument12 pagesParametric Vs Non Parametric StatisticsiampuneiteNo ratings yet
- BMC Psychiatry: An Animated Depiction of Major Depression EpidemiologyDocument6 pagesBMC Psychiatry: An Animated Depiction of Major Depression Epidemiologyklysmanu93No ratings yet
- Survival Analysis With Python Tutorial - How, What, When, and Why - by Towards AI Team - Towards AIDocument44 pagesSurvival Analysis With Python Tutorial - How, What, When, and Why - by Towards AI Team - Towards AI8c354be21dNo ratings yet
- Measures of Disease Frequency NOTESDocument22 pagesMeasures of Disease Frequency NOTESSJ JungNo ratings yet
- Metlit 11-Survival Analysis - KuntjoroDocument45 pagesMetlit 11-Survival Analysis - KuntjoroLaurencia LenyNo ratings yet
- Mathematical EpidemiologyDocument12 pagesMathematical EpidemiologyAhmed EshebliNo ratings yet
- 3 Summarizing DataDocument71 pages3 Summarizing DataJoevyvamae TorreNo ratings yet
- Diagnosis and Treatment of Bacterial ProstatitisDocument5 pagesDiagnosis and Treatment of Bacterial ProstatitislobeseyNo ratings yet
- Epidemiology SlidesDocument30 pagesEpidemiology SlidesHongMingNo ratings yet
- The study of disease distribution and determinantsDocument409 pagesThe study of disease distribution and determinantsfonka100% (2)
- AKC Histo Drawings PDFDocument130 pagesAKC Histo Drawings PDFDanDeleanuNo ratings yet
- Malaria Disease Prediction and Grading System: A Performance Model of Multinomial Naïve Bayes (MNB) Machine Learning in Nigerian HospitalsDocument14 pagesMalaria Disease Prediction and Grading System: A Performance Model of Multinomial Naïve Bayes (MNB) Machine Learning in Nigerian HospitalsTemitope Olufunmi AtoyebiNo ratings yet
- Young Adult Stroke Prediction Using Machine LearningDocument5 pagesYoung Adult Stroke Prediction Using Machine LearningInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Dynamics of Disease TransmissionDocument18 pagesThe Dynamics of Disease TransmissionJ MNo ratings yet
- 02-Cross Sectional Studies 2017Document30 pages02-Cross Sectional Studies 2017Whatever UseeNo ratings yet
- Descriptive Epidemiology Study Types and MethodsDocument34 pagesDescriptive Epidemiology Study Types and Methodslemon yellowNo ratings yet
- Understanding EpidemiologyDocument40 pagesUnderstanding EpidemiologyCharityOchiengNo ratings yet
- Epidemiological Study Design Cheat Sheet 1Document1 pageEpidemiological Study Design Cheat Sheet 1Syed Muhammad Shazan Ali RizviNo ratings yet
- Week-5-Exposure Assessment and ModelsDocument72 pagesWeek-5-Exposure Assessment and ModelsAndrew_Jay_Mal_4286100% (1)
- Incidence and Prevalence PDFDocument9 pagesIncidence and Prevalence PDFSreya SanilNo ratings yet
- Okuda-Time Series Analysis of Under-Five MortalityDocument61 pagesOkuda-Time Series Analysis of Under-Five MortalityBoniface Okuda100% (4)
- Evidence Based Medicine: What It Is and What It Isn'tDocument3 pagesEvidence Based Medicine: What It Is and What It Isn'tCristian EstradaNo ratings yet
- Case-Control Study: Dr. Sourab Kumar DasDocument31 pagesCase-Control Study: Dr. Sourab Kumar DasSanjeet SahNo ratings yet
- Hierarchy of Epidemiologic Study Design: Tower & Spector, 2007Document42 pagesHierarchy of Epidemiologic Study Design: Tower & Spector, 2007Aslam BajwaNo ratings yet
- Assignt On Computer Application in AgricultureDocument11 pagesAssignt On Computer Application in AgricultureK.A. Law Nominee LTDNo ratings yet
- Basic Concepts in Epidemiology 2Document42 pagesBasic Concepts in Epidemiology 2Twinkle SalongaNo ratings yet
- Epidemiology: Dr. Sheryl M. ReyesDocument19 pagesEpidemiology: Dr. Sheryl M. ReyesNilda ReyesNo ratings yet
- Breast Cancer by Sadaf NaeemDocument11 pagesBreast Cancer by Sadaf NaeemSadaf naeemNo ratings yet
- Disease Surveillance in India: DR Sampath K Krishnan National Professional Officer (Communicable Diseases Surveillance)Document54 pagesDisease Surveillance in India: DR Sampath K Krishnan National Professional Officer (Communicable Diseases Surveillance)Sri Rama Suryatez KattulaNo ratings yet
- Epidemiology Study Design GuideDocument20 pagesEpidemiology Study Design GuideChristian JeffersonNo ratings yet
- Association and CausationDocument60 pagesAssociation and Causationsehar_bashirNo ratings yet
- Meta-Analysis: Montarat Thavorncharoensap, Ph.D. Faculty of Pharmacy, Mahidol UniversityDocument44 pagesMeta-Analysis: Montarat Thavorncharoensap, Ph.D. Faculty of Pharmacy, Mahidol UniversityNanangNo ratings yet
- Life Table ApproachDocument32 pagesLife Table ApproachDrnuzhat Fatema100% (1)
- Child Vaccination Schedule by Age SingaporeDocument3 pagesChild Vaccination Schedule by Age Singaporefcleong69No ratings yet
- MicroRNA in CancerDocument148 pagesMicroRNA in CancerDevvvNo ratings yet
- Recurrence Stroke of Ischemic Stroke Patients in Thailand:a Nationwide StudyDocument7 pagesRecurrence Stroke of Ischemic Stroke Patients in Thailand:a Nationwide StudyIJPHSNo ratings yet
- Case Control Study DesignDocument15 pagesCase Control Study Designgeorgeloto12No ratings yet
- Count, Rate, Ratio, ProportionDocument51 pagesCount, Rate, Ratio, Proportionprasanna lamaNo ratings yet
- SIS Model For An Infectious DiseaseDocument3 pagesSIS Model For An Infectious DiseaseMohammed AlnasryNo ratings yet
- 1 Interim ReportDocument29 pages1 Interim ReportPiyush sharmaNo ratings yet
- Week 4 CPH LEC - Introduction To Epidemiology: Fundamentals of Epidemiology in Public Health PracticeDocument11 pagesWeek 4 CPH LEC - Introduction To Epidemiology: Fundamentals of Epidemiology in Public Health PracticeQueency DangilanNo ratings yet
- Blood Smears and The Use of Wrights StainDocument5 pagesBlood Smears and The Use of Wrights Stainkaleb16_2No ratings yet
- Chodankar2021 Real World Evidence Vs RCTDocument4 pagesChodankar2021 Real World Evidence Vs RCTMumtaz MaulanaNo ratings yet
- Survival AnalysisDocument16 pagesSurvival AnalysisMeNo ratings yet
- 2011 - Metformin - Multi-Faceted Protection Against CancerDocument22 pages2011 - Metformin - Multi-Faceted Protection Against CancerVladDaculNo ratings yet
- Epidemiology in EmergenciesDocument18 pagesEpidemiology in EmergenciessmartisaacNo ratings yet
- Knowledge Assessment of Female Students of Southern Technical University in Basrah-Iraq, Regarding Breast Cancer and BSEDocument12 pagesKnowledge Assessment of Female Students of Southern Technical University in Basrah-Iraq, Regarding Breast Cancer and BSERajaa A. MahmoudNo ratings yet
- Climate Change and Vector-Borne Diseases of Public Health SignificanceDocument8 pagesClimate Change and Vector-Borne Diseases of Public Health SignificanceAriadne Cristina De Antonio100% (1)
- Cohort Study: Steps, Types, Advantages and ChallengesDocument88 pagesCohort Study: Steps, Types, Advantages and Challengesankirana02No ratings yet
- PHD Thesis TempDocument25 pagesPHD Thesis TempSaleh Al-SugairNo ratings yet
- Oral Epidemiology: Epidemiology. Dr. Mohamed Al-MontaserDocument58 pagesOral Epidemiology: Epidemiology. Dr. Mohamed Al-Montaserغلاها عبدوNo ratings yet
- Research TechniquesDocument90 pagesResearch TechniquesTimothy Ian KooNo ratings yet
- Test Statistics Formulas For Probabiltity and StatisticsDocument6 pagesTest Statistics Formulas For Probabiltity and StatisticsJet Niko BrizuelaNo ratings yet
- Managing Sickle Cell DiseaseDocument50 pagesManaging Sickle Cell DiseaseAlphonse AsobochiaNo ratings yet
- Cardiovascular SystemDocument74 pagesCardiovascular Systemاسامة محمد السيد رمضانNo ratings yet
- Gastrointestinal System - Lecture 8Document54 pagesGastrointestinal System - Lecture 8Ibrahem AlNo ratings yet
- Patient Education: A Guide for NursesDocument32 pagesPatient Education: A Guide for Nursesاسامة محمد السيد رمضانNo ratings yet
- Cardiovascular SystemDocument74 pagesCardiovascular Systemاسامة محمد السيد رمضانNo ratings yet
- Eyes - Ears - Mouth - Nose (Lecture 5)Document50 pagesEyes - Ears - Mouth - Nose (Lecture 5)اسامة محمد السيد رمضانNo ratings yet
- General Survey & Health History Part 1Document23 pagesGeneral Survey & Health History Part 1اسامة محمد السيد رمضانNo ratings yet
- 8 Group DynamicsDocument30 pages8 Group Dynamicsاسامة محمد السيد رمضانNo ratings yet
- 5 Communication SkillsDocument39 pages5 Communication Skillsاسامة محمد السيد رمضانNo ratings yet
- Motivating Learners: Factors and ModelsDocument28 pagesMotivating Learners: Factors and Modelsاسامة محمد السيد رمضان100% (1)
- Verbal Communication SkillsDocument28 pagesVerbal Communication Skillsاسامة محمد السيد رمضانNo ratings yet
- 3 - Learning TheoriesDocument22 pages3 - Learning Theoriesاسامة محمد السيد رمضانNo ratings yet
- 2 - The Role of LearnerDocument30 pages2 - The Role of Learnerاسامة محمد السيد رمضانNo ratings yet
- 2 Priciples of CommunicationDocument16 pages2 Priciples of Communicationاسامة محمد السيد رمضانNo ratings yet
- Non Verbal Communication: by Dr. Nadia BassuoniDocument38 pagesNon Verbal Communication: by Dr. Nadia Bassuoniاسامة محمد السيد رمضانNo ratings yet
- Chapter 5 - Displacement of UterusDocument25 pagesChapter 5 - Displacement of Uterusاسامة محمد السيد رمضانNo ratings yet
- Verbal Communication SkillsDocument28 pagesVerbal Communication Skillsاسامة محمد السيد رمضانNo ratings yet
- 1 Definition of TermsDocument15 pages1 Definition of Termsاسامة محمد السيد رمضانNo ratings yet
- Chapter 6 - Infertility Lecture NewDocument26 pagesChapter 6 - Infertility Lecture Newاسامة محمد السيد رمضان100% (1)
- Chapter 2 - Physiology of MenstruationDocument18 pagesChapter 2 - Physiology of Menstruationاسامة محمد السيد رمضان100% (1)
- 5 Planning and Conducting ClassesDocument24 pages5 Planning and Conducting Classesاسامة محمد السيد رمضانNo ratings yet
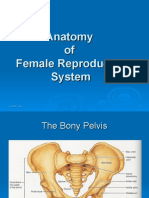
- Chapter 1-Anatomy of Female Reproductive SystemDocument31 pagesChapter 1-Anatomy of Female Reproductive Systemاسامة محمد السيد رمضانNo ratings yet
- Chapter 2 - Physiology of MenstruationDocument18 pagesChapter 2 - Physiology of Menstruationاسامة محمد السيد رمضان100% (1)
- Epidemiology and PreventionDocument34 pagesEpidemiology and Preventionاسامة محمد السيد رمضانNo ratings yet
- Importance of Epidemiology for Public HealthDocument45 pagesImportance of Epidemiology for Public Healthاسامة محمد السيد رمضانNo ratings yet
- Epidemiology Lec 1Document24 pagesEpidemiology Lec 1اسامة محمد السيد رمضانNo ratings yet
- Epidemiology and PreventionDocument34 pagesEpidemiology and Preventionاسامة محمد السيد رمضانNo ratings yet
- Chapter 1-Anatomy of Female Reproductive SystemDocument31 pagesChapter 1-Anatomy of Female Reproductive Systemاسامة محمد السيد رمضانNo ratings yet
- Epidemiology Lec 4 - 1Document21 pagesEpidemiology Lec 4 - 1اسامة محمد السيد رمضانNo ratings yet
- Epidemiology Lec 4 - 1Document21 pagesEpidemiology Lec 4 - 1اسامة محمد السيد رمضانNo ratings yet
- Eyelids, Conjunctiva, Cornea and Sclera: McquestionsDocument52 pagesEyelids, Conjunctiva, Cornea and Sclera: McquestionsHawwi Ismail100% (1)
- Cystic Liver LesionsDocument2 pagesCystic Liver LesionsNatnael GetahunNo ratings yet
- At The Crossroads of Gout and Psoriatic Arthritis: "Psout"Document9 pagesAt The Crossroads of Gout and Psoriatic Arthritis: "Psout"ireneardianiNo ratings yet
- Wordly Wise Book 4Document153 pagesWordly Wise Book 4Lillian Liang84% (45)
- Frontiers - Rheumatic Heart Valve Disease Pathophysiology and Underlying MechanismsDocument33 pagesFrontiers - Rheumatic Heart Valve Disease Pathophysiology and Underlying MechanismsJAHNELLA XYRINE PERITONo ratings yet
- SGA Guide: Causes, Risks and Care of Small for Gestational Age InfantsDocument3 pagesSGA Guide: Causes, Risks and Care of Small for Gestational Age InfantsAdiel CalsaNo ratings yet
- Monitoring An IV Site and InfusionDocument4 pagesMonitoring An IV Site and InfusionAlex Cacayan CortinaNo ratings yet
- DynaMed Plus Rheumatoid ArthritisDocument20 pagesDynaMed Plus Rheumatoid ArthritisHeather Marie MathisNo ratings yet
- Health Information & Basic Medical StatisticsDocument65 pagesHealth Information & Basic Medical StatisticsSaiNo ratings yet
- 5-Antemortem ExaminationDocument14 pages5-Antemortem ExaminationXher FaixalNo ratings yet
- Bacteriology Questions 2Document8 pagesBacteriology Questions 2Kry VillanuevaNo ratings yet
- Herpes Viruses: Clinical FeaturesDocument4 pagesHerpes Viruses: Clinical FeaturesMoka MohsenNo ratings yet
- Bedside Evaluation of DysphagiaDocument41 pagesBedside Evaluation of Dysphagiaaleeza nomanNo ratings yet
- Anxiety Disorders: David R. Rosenberg and Jennifer A. ChiribogaDocument10 pagesAnxiety Disorders: David R. Rosenberg and Jennifer A. ChiribogaMelissa CohenNo ratings yet
- 5 Nursing Diagnosis For GlomerulonephritisDocument2 pages5 Nursing Diagnosis For GlomerulonephritisGeorich Narciso67% (3)
- Otitis Externaand Otitis Mediain 76 Cats 2013Document11 pagesOtitis Externaand Otitis Mediain 76 Cats 2013kadek ayu ichaNo ratings yet
- MCN RLE Sitz Bath Procedure ChecklistDocument3 pagesMCN RLE Sitz Bath Procedure ChecklistHannah Angelu Cabading100% (1)
- Case Study - PneumoniaDocument14 pagesCase Study - Pneumonianeil garcia89% (36)
- Recommended Texts For Neurology Trainees 2Document5 pagesRecommended Texts For Neurology Trainees 2Karam Ali ShahNo ratings yet
- Practice of Medicine - by Balaram JanaDocument93 pagesPractice of Medicine - by Balaram JanaFarhana V PNo ratings yet
- Apple Cider Vinegar For Wart RemovalDocument1 pageApple Cider Vinegar For Wart RemovaljohnnyNo ratings yet
- Oregon Health Authority COVID-19 Weekly Report (Published 10/28)Document38 pagesOregon Health Authority COVID-19 Weekly Report (Published 10/28)KGW NewsNo ratings yet
- Taenia Solium Cysticercosis - The Lessons of HistoryDocument4 pagesTaenia Solium Cysticercosis - The Lessons of HistoryAntonio Márquez LaraNo ratings yet
- Respiratory System: Agatha Babyet A. Alabata, Bsn-Iii StemDocument31 pagesRespiratory System: Agatha Babyet A. Alabata, Bsn-Iii StemJay VillasotoNo ratings yet
- Delusional Disorder: by Dr. Min Min Phyo 27 May 2019Document56 pagesDelusional Disorder: by Dr. Min Min Phyo 27 May 2019thu thuNo ratings yet
- 4.3 - Educating Patients, Family, and Health Care Professionals About Foot CareDocument1 page4.3 - Educating Patients, Family, and Health Care Professionals About Foot CareEva Cica SusantiNo ratings yet
- 01.02 - Organizing Knowledge and InformationDocument12 pages01.02 - Organizing Knowledge and InformationDaphne DunneNo ratings yet
- Ampicillin Drug Study GuideDocument3 pagesAmpicillin Drug Study GuideAlyssa Mae DumularNo ratings yet
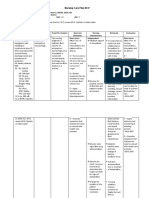
- Nursing Care Plan NCPDocument24 pagesNursing Care Plan NCPRosemarie R. Reyes100% (1)
- Obstructive Diseases Cheat SheetDocument5 pagesObstructive Diseases Cheat SheetWiz SamNo ratings yet