You might also like
- Respiratory Nursing #1Document19 pagesRespiratory Nursing #1shenric16100% (12)
- Problems With OxygenationDocument92 pagesProblems With OxygenationEbiNo ratings yet
- Respiratory gymnastics (Translated): Purification - Health - Strength - EnergyFrom EverandRespiratory gymnastics (Translated): Purification - Health - Strength - EnergyNo ratings yet
- Test results and costs for disease diagnosisDocument3 pagesTest results and costs for disease diagnosisWathek Al Zuaiby67% (6)
- Injector and Ignition Driver For Automotive ApplicationsDocument25 pagesInjector and Ignition Driver For Automotive ApplicationsAnonymous 4IEjoc100% (2)
- Econometric S Lecture 45Document31 pagesEconometric S Lecture 45Khurram AzizNo ratings yet
- The Respiratory SystemDocument117 pagesThe Respiratory SystemPark chin-haeNo ratings yet
- Physiology of RespirationDocument26 pagesPhysiology of Respirationrevaniwati100% (1)
- List of Indian Standard Code For Civil and Structural Works PDFDocument148 pagesList of Indian Standard Code For Civil and Structural Works PDFKalipada Sen100% (1)
- Respiratory SystemDocument192 pagesRespiratory SystemQuolette Constante100% (1)
- D Physiology of RespirationDocument45 pagesD Physiology of RespirationValluri Mukesh100% (1)
- (STATISTICS & PROBABILITY) Unit II - Lesson 1 Understanding The Normal Curve DistributionDocument14 pages(STATISTICS & PROBABILITY) Unit II - Lesson 1 Understanding The Normal Curve DistributionVany SpadesNo ratings yet
- Basic Respiratory Mechanics: Ventilation, Diffusion, and Gas ExchangeDocument36 pagesBasic Respiratory Mechanics: Ventilation, Diffusion, and Gas ExchangeRizqi Luqmanul HakimNo ratings yet
- Oxygenation 1 PDFDocument4 pagesOxygenation 1 PDFAbdullah Al NomanNo ratings yet
- Breathing and Exchange of GasesDocument5 pagesBreathing and Exchange of Gaseslpc4944No ratings yet
- Anatomy and Physiology of Respiratory SystemDocument34 pagesAnatomy and Physiology of Respiratory SystemSamson SeiduNo ratings yet
- Nat Reviewer Set B - Math 10Document2 pagesNat Reviewer Set B - Math 10Jo Mai Hann90% (10)
- Review of Respiratory PhysiologyDocument53 pagesReview of Respiratory PhysiologyMiftahul IfahNo ratings yet
- Notes of Human Physiology Class 11Document9 pagesNotes of Human Physiology Class 11ADWAITH LALUNo ratings yet
- 11 Biology Notes ch17-pdf1Document9 pages11 Biology Notes ch17-pdf1LishaNo ratings yet
- Respiratory System (Week 14)Document33 pagesRespiratory System (Week 14)Krisha Mabel TabijeNo ratings yet
- CBSE Class 11 Biology Chapter 17 Notes on Breathing and Exchange of GasesDocument8 pagesCBSE Class 11 Biology Chapter 17 Notes on Breathing and Exchange of Gasesfast-track for n2021No ratings yet
- SPM Notes On Chapter RespirationDocument18 pagesSPM Notes On Chapter RespirationSyamila YusofNo ratings yet
- BREATHING & GASES EXCHANGEDocument7 pagesBREATHING & GASES EXCHANGEKankana Biswas100% (1)
- CBSE Quick Revision Notes on Breathing and Exchange of GasesDocument4 pagesCBSE Quick Revision Notes on Breathing and Exchange of GasesParimala deviNo ratings yet
- MODULE 22 HANDOUTS Repiratory SystemDocument3 pagesMODULE 22 HANDOUTS Repiratory SystemMichaela PoNo ratings yet
- Self test 3Document6 pagesSelf test 3202310446No ratings yet
- 9572 (21) 00068-X/fulltext: GuidelinesDocument53 pages9572 (21) 00068-X/fulltext: GuidelinesRehoboth BandaNo ratings yet
- Functional Anatomy of The Respiratory SystemDocument3 pagesFunctional Anatomy of The Respiratory SystemRica Mae TingcoNo ratings yet
- Human Respiratory System ExplainedDocument4 pagesHuman Respiratory System ExplainedSheehan MathurNo ratings yet
- Oxygen InsufficiencyDocument16 pagesOxygen Insufficiencydeolzf100% (1)
- The Respiratory System: An OverviewDocument33 pagesThe Respiratory System: An OverviewCess Abad AgcongNo ratings yet
- Ventilation and Respiratory Volumes ExplainedDocument20 pagesVentilation and Respiratory Volumes ExplainedJessa mae CabredoNo ratings yet
- Breathing and RespirationDocument30 pagesBreathing and Respirationhamzahazard527No ratings yet
- Functions of The Respiratory SysteDocument5 pagesFunctions of The Respiratory SysteMohd FirdausNo ratings yet
- Breathing & Exchange of GasesDocument5 pagesBreathing & Exchange of GasesMamta TiwariNo ratings yet
- Introduction To Respiratory SystemDocument5 pagesIntroduction To Respiratory SystemDr Md Abedur RahmanNo ratings yet
- Physiology of The Respiratory System: Citra Rosyidah Physiology Department Medical Faculty Hasanuddin UniversityDocument28 pagesPhysiology of The Respiratory System: Citra Rosyidah Physiology Department Medical Faculty Hasanuddin UniversityHartarto AkhmadNo ratings yet
- Respiiiraatatoory SystemDocument78 pagesRespiiiraatatoory Systempriyanshuraj717No ratings yet
- Respiratory SystemDocument7 pagesRespiratory SystemNgenyi ChiarittaNo ratings yet
- Sistem Respirasi-Isti AnindyaDocument18 pagesSistem Respirasi-Isti AnindyaSindia MirnaNo ratings yet
- Hand Note - Session-1 2Document12 pagesHand Note - Session-1 2Abod AbodNo ratings yet
- The Respiratory SystemDocument2 pagesThe Respiratory SystemRaluca MoldovanNo ratings yet
- Topic 10 - Respiratory System Chapter 18Document6 pagesTopic 10 - Respiratory System Chapter 18api-388956899No ratings yet
- Fisiologi Respirasi: Proses Pernapasan dan Pertukaran GasDocument49 pagesFisiologi Respirasi: Proses Pernapasan dan Pertukaran GasRaniyah Az-zahraNo ratings yet
- Respiratory SystemDocument56 pagesRespiratory SystemSalma NawazNo ratings yet
- Physiology Previous Year PDFDocument129 pagesPhysiology Previous Year PDFmina mounirNo ratings yet
- WEEK 11 ANPH 111Document6 pagesWEEK 11 ANPH 111itsmearonsupanNo ratings yet
- Fundamental Concepts of Anesthesiology: Dr. Weiwei LiuDocument31 pagesFundamental Concepts of Anesthesiology: Dr. Weiwei Liusimple livingNo ratings yet
- The Respiratory SystemDocument2 pagesThe Respiratory SystemconnievelardeNo ratings yet
- Ncert Solution Breathing and Exchange of GasesDocument10 pagesNcert Solution Breathing and Exchange of GasesAyush DuttaNo ratings yet
- Respiratory SystemDocument5 pagesRespiratory SystemJay QuilnetNo ratings yet
- Reflection Respiratory SystemDocument4 pagesReflection Respiratory SystemAin Sufiza0% (1)
- Sistem PernafasanDocument87 pagesSistem Pernafasantaufik HidayatNo ratings yet
- Respiratory Physiology PostedDocument25 pagesRespiratory Physiology PostedYeni PuspitaNo ratings yet
- Respiratory SystemDocument53 pagesRespiratory SystemRotan CirebonNo ratings yet
- General Physiology II - Transport of Oxygen & Carbon - SIUST, College of DentistryDocument7 pagesGeneral Physiology II - Transport of Oxygen & Carbon - SIUST, College of DentistryNoor Al-Deen MaherNo ratings yet
- Oxygen InsufficiencyDocument24 pagesOxygen InsufficiencyRatna VimalNo ratings yet
- Respiratory System: Critical Care Nurse Training Program R.A.I.S.E. Nepal ProjectDocument240 pagesRespiratory System: Critical Care Nurse Training Program R.A.I.S.E. Nepal ProjectTika RawatNo ratings yet
- Breathing and Exchange of Gases: A Guide to RespirationDocument4 pagesBreathing and Exchange of Gases: A Guide to RespirationSreeyansu RajNo ratings yet
- Chapter 17 - BREATHING AND EXCHANGE OF GASESDocument7 pagesChapter 17 - BREATHING AND EXCHANGE OF GASESprernatiwary508No ratings yet
- Normal Oxygen Transport: Susanne A ClarkDocument256 pagesNormal Oxygen Transport: Susanne A Clarkghoncheh0% (1)
- PDBreathing and Exchange of Gases Class 11 Notes CBSE Biology Chapter 17FDocument15 pagesPDBreathing and Exchange of Gases Class 11 Notes CBSE Biology Chapter 17Fgandhitirth147No ratings yet
- Pulmonary Endocrine Pathology: Endocrine Cells and Endocrine Tumours of the LungFrom EverandPulmonary Endocrine Pathology: Endocrine Cells and Endocrine Tumours of the LungNo ratings yet
- ENGWhy Dolores SuffocateDocument3 pagesENGWhy Dolores SuffocateMohammed Faizuddin siddiquiNo ratings yet
- ENG Theme 4 Real Chemical LoadDocument8 pagesENG Theme 4 Real Chemical LoadMohammed Faizuddin siddiquiNo ratings yet
- Blood & Circulation HistologyDocument45 pagesBlood & Circulation HistologyMohammed Faizuddin siddiquiNo ratings yet
- BiochemistryDocument113 pagesBiochemistryMohammed Faizuddin siddiqui100% (1)
- Jurimetrics 1Document24 pagesJurimetrics 1Maiko Lesmana D0% (1)
- JadualDocument4 pagesJadualhouseNo ratings yet
- TM 11-6665-224-15Document113 pagesTM 11-6665-224-15SiviNo ratings yet
- Find Correlation and Regression Between TV Ad Spend and SalesDocument5 pagesFind Correlation and Regression Between TV Ad Spend and SalesTARVEEN DuraiNo ratings yet
- Manual Tupia MAKITA 2301Document16 pagesManual Tupia MAKITA 2301proftononNo ratings yet
- ArchModels Volume - 126 PDFDocument40 pagesArchModels Volume - 126 PDFgombestralalaNo ratings yet
- ECE 2303 Soil Mech 1 GR A Batch 1 PDFDocument32 pagesECE 2303 Soil Mech 1 GR A Batch 1 PDFCalebNo ratings yet
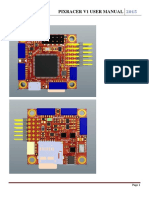
- Pixracer V1 User Manual EN PDFDocument8 pagesPixracer V1 User Manual EN PDFChrisNo ratings yet
- Force Gauge Datalogger 100kg ReviewDocument2 pagesForce Gauge Datalogger 100kg ReviewWilly AndretyNo ratings yet
- Relational Database: Storing and Manipulating RecordsDocument34 pagesRelational Database: Storing and Manipulating RecordsaNo ratings yet
- Course Work 1Document4 pagesCourse Work 1Alice PreciousNo ratings yet
- Paper Lncs PDFDocument57 pagesPaper Lncs PDFNeilNo ratings yet
- Introduction To Human Anatomy and Physiology: Joher B. Mendez, JR., R.N., M.DDocument65 pagesIntroduction To Human Anatomy and Physiology: Joher B. Mendez, JR., R.N., M.DJoherNo ratings yet
- ChlorantraniliproleDocument3 pagesChlorantraniliproleLaura GuarguatiNo ratings yet
- Unit 3 Tree StructureDocument19 pagesUnit 3 Tree StructureNida AhmedNo ratings yet
- Amarillo 1000 1800 Repair ManualDocument32 pagesAmarillo 1000 1800 Repair ManualmuazmaslanNo ratings yet
- Introduction To Structural AnalysisDocument15 pagesIntroduction To Structural AnalysisShereen RodrigoNo ratings yet
- Docu46403 White Paper EMC Documentum D2 4.1 InteroperabilityDocument16 pagesDocu46403 White Paper EMC Documentum D2 4.1 InteroperabilityHariprasad ManchiNo ratings yet
- Active Heave Drilling Drawworks Improve Rig EfficiencyDocument5 pagesActive Heave Drilling Drawworks Improve Rig Efficiencygplese0No ratings yet
- Discussion Sa QualiDocument2 pagesDiscussion Sa QualiAngel Rose SalinasalNo ratings yet
- Equations Needed Full Answers and Working Redox Reaction Theory Qualitative AnalysisDocument13 pagesEquations Needed Full Answers and Working Redox Reaction Theory Qualitative AnalysisEmmaNo ratings yet
- West LP - M3 U6 L9Document10 pagesWest LP - M3 U6 L9Gretchen WestNo ratings yet
- GPIB Communication and Hardware SpecificationsDocument5 pagesGPIB Communication and Hardware Specificationsshofika SelvarajNo ratings yet