You might also like
- Cardiology - CVS OSCE ChecklistDocument5 pagesCardiology - CVS OSCE ChecklistPraveenaNo ratings yet
- 1 OMD, Indikasi, Dan Mekanisme Rujukan PanoramicDocument57 pages1 OMD, Indikasi, Dan Mekanisme Rujukan PanoramicDian KafahasindayaNo ratings yet
- Peritoneum and Peritoneal CavityDocument26 pagesPeritoneum and Peritoneal CavitytuhinsinghNo ratings yet
- Oesophagus Maag DuodenographyDocument49 pagesOesophagus Maag DuodenographyEvan DionesiaNo ratings yet
- Coass OmdDocument47 pagesCoass OmdKevin SurjadiNo ratings yet
- 14 - Barium Studies For GIT With NotesDocument50 pages14 - Barium Studies For GIT With NotesSunil ThomasNo ratings yet
- UgiDocument61 pagesUgiandisibaNo ratings yet
- Radio BoxDocument112 pagesRadio BoxFranclene MillaNo ratings yet
- PEMERIKSAAN RADIOLOGI PADA GASTRITIS DAN ULKUS-edited2017Document51 pagesPEMERIKSAAN RADIOLOGI PADA GASTRITIS DAN ULKUS-edited2017shrt gtNo ratings yet
- Pa of Abdomen PrintDocument14 pagesPa of Abdomen PrintAnj LTNo ratings yet
- Surface TopographyDocument8 pagesSurface Topographyferdinand padillaNo ratings yet
- Barium Studies For GIT With NotesDocument50 pagesBarium Studies For GIT With NotesfaradisahadniNo ratings yet
- GIT OSCE (Week 9) : Mention You Would Observe General Appearance and Take VitalsDocument3 pagesGIT OSCE (Week 9) : Mention You Would Observe General Appearance and Take Vitalsrenae_vardNo ratings yet
- 1.01 Esophagus and Diaphragmatic HerniaDocument10 pages1.01 Esophagus and Diaphragmatic HerniaZazaNo ratings yet
- The Abdomen: E Sther Sunday C. Faller, RMT, MDDocument7 pagesThe Abdomen: E Sther Sunday C. Faller, RMT, MDMarimiel PagulayanNo ratings yet
- Mahadevan, V. (2017) - Anatomy of The Stomach. Surgery (Oxford)Document4 pagesMahadevan, V. (2017) - Anatomy of The Stomach. Surgery (Oxford)anastasijaNo ratings yet
- Abdomen II: Handout VersionDocument68 pagesAbdomen II: Handout VersionTdoc TonyNo ratings yet
- Abdomen ExamDocument2 pagesAbdomen ExamGeryl Mikka VillanuevaNo ratings yet
- TheOrganizedMedic Free Respiratory OSCE GuideDocument12 pagesTheOrganizedMedic Free Respiratory OSCE GuideMOHAMMED ASHIFNo ratings yet
- Abdominal SignDocument85 pagesAbdominal Signnovitafitri123No ratings yet
- Saint Louis University School of Medicine Mmxxii: Dr. Laygo - October 22, 2020Document37 pagesSaint Louis University School of Medicine Mmxxii: Dr. Laygo - October 22, 2020Djan Kurvie ValencerinaNo ratings yet
- Abdominal WallDocument4 pagesAbdominal WallAwais Usman MirzaNo ratings yet
- 02 General SurgeryDocument34 pages02 General SurgerySarathi IrisNo ratings yet
- LEC 1 - Abdomen 1 2009 OLDDocument3 pagesLEC 1 - Abdomen 1 2009 OLDElle ReyesNo ratings yet
- Compiled - Abdomen, S&E, NeuroDocument77 pagesCompiled - Abdomen, S&E, Neuronovelynembarte.medsNo ratings yet
- Abdominal PainDocument6 pagesAbdominal PainHynne Jhea EchavezNo ratings yet
- HO - SplanchnologyDocument29 pagesHO - SplanchnologyEugene Osei AmoakoNo ratings yet
- Spine & Extremities / Abdomen / Neurologic Exam: PalpationDocument8 pagesSpine & Extremities / Abdomen / Neurologic Exam: PalpationBrent DizonNo ratings yet
- Anatomi Radiologi Barium Studies For GITDocument52 pagesAnatomi Radiologi Barium Studies For GITRio ArbiansyahNo ratings yet
- Intro To Abdominal Cavity (Merrick)Document35 pagesIntro To Abdominal Cavity (Merrick)Sidiq AboobakerNo ratings yet
- Radiography of The Pharnyx & Esophagus: Film CritiqueDocument30 pagesRadiography of The Pharnyx & Esophagus: Film CritiqueRika WulandariNo ratings yet
- ESPU-N Paediatric Physical Assessment Within Continence Care-Bowel and BladderDocument6 pagesESPU-N Paediatric Physical Assessment Within Continence Care-Bowel and BladderYonathan SanjayaNo ratings yet
- M1207 GIT E2 ForegutDocument29 pagesM1207 GIT E2 Foregutkavinduherath2000No ratings yet
- Abdominal UltrasoundDocument40 pagesAbdominal UltrasoundfatimaNo ratings yet
- Anatomy of G.I.TDocument8 pagesAnatomy of G.I.Talokpalresha100% (2)
- ABDOMENDocument2 pagesABDOMENJames MoralesNo ratings yet
- (Surgery) Midterms PediatricsDocument5 pages(Surgery) Midterms Pediatricsalmira.s.mercadoNo ratings yet
- Abdominal Assessment HA LectureDocument44 pagesAbdominal Assessment HA LectureKatrina BeltranNo ratings yet
- Allll Exams Combinedd FinalDocument14 pagesAllll Exams Combinedd FinalAnshuNo ratings yet
- 3 - Female PelvisDocument27 pages3 - Female PelvisKandula KasunNo ratings yet
- Stomach, Duodenum, Pancreas, and Spleen (Valera)Document4 pagesStomach, Duodenum, Pancreas, and Spleen (Valera)Joshua MandaweNo ratings yet
- BD Chaurasia's Human Anatomy, VoDocument11 pagesBD Chaurasia's Human Anatomy, VoGanjuNo ratings yet
- Retdem Checklist: Abdomen Lopez, Marjorie Joy C.: Refer To Picture inDocument4 pagesRetdem Checklist: Abdomen Lopez, Marjorie Joy C.: Refer To Picture inAT4-11 HUMSS 2 CEDRICK ILAONo ratings yet
- Gastrointestinal - AnatomyDocument10 pagesGastrointestinal - AnatomyFirmanHidayatNo ratings yet
- How To Read Chest Abdomen CT Scan X-RayDocument86 pagesHow To Read Chest Abdomen CT Scan X-RaymuhammadfyNo ratings yet
- MCN Module 3Document9 pagesMCN Module 3Fatrick BernardinoNo ratings yet
- Trans 1Document4 pagesTrans 1Honey VargasNo ratings yet
- Semi Finals Coverage H.ADocument28 pagesSemi Finals Coverage H.AdiarosedoloresbsncNo ratings yet
- Respi 2Document11 pagesRespi 2Jeno SigamaniNo ratings yet
- X - Ray Dr. Allam 2021Document26 pagesX - Ray Dr. Allam 2021little miss scare-allNo ratings yet
- Presentation1 IleusDocument57 pagesPresentation1 IleusSetiawan SukmadjaNo ratings yet
- The Spleen Meridian of Foot-Taiyin For Certificate Course1Document16 pagesThe Spleen Meridian of Foot-Taiyin For Certificate Course1Brian Chi Yan Cheng 鄭智仁No ratings yet
- Osce AbdomenDocument33 pagesOsce AbdomenistiNo ratings yet
- Pemeriksaan AbdomenDocument46 pagesPemeriksaan AbdomenPrystia_RNo ratings yet
- Abdominal ExaminationDocument56 pagesAbdominal ExaminationAnggreani PutriNo ratings yet
- Review Notes - Radiographic Positioning and Radiologic Procedures I PDFDocument30 pagesReview Notes - Radiographic Positioning and Radiologic Procedures I PDFCziara JustineNo ratings yet
- Yyyyycrash Course Anatomy - AbdomenDocument31 pagesYyyyycrash Course Anatomy - Abdomen黃芳昌No ratings yet
- Digestive SystemDocument2 pagesDigestive SystemRANGSINEE SUWANNASUKNo ratings yet
- Anatomy Large IntestineDocument4 pagesAnatomy Large IntestinetristineNo ratings yet
- ENT RadiologiDocument70 pagesENT RadiologiyowwwNo ratings yet
- Guidance On Designing Healthcare External Evaluation Programmes Including Accreditation-1Document84 pagesGuidance On Designing Healthcare External Evaluation Programmes Including Accreditation-1greg_enricoNo ratings yet
- Spec - MINDRAY Digital Radiography System - Digieye 760Document2 pagesSpec - MINDRAY Digital Radiography System - Digieye 760greg_enricoNo ratings yet
- RADIOLOGI MATA Modul 5.2Document42 pagesRADIOLOGI MATA Modul 5.2greg_enricoNo ratings yet
- Assessment of Patient's Waiting Time in The RadiologyDocument7 pagesAssessment of Patient's Waiting Time in The Radiologygreg_enricoNo ratings yet
- Imaging of Osteonecrosis of The Femoral HeadDocument28 pagesImaging of Osteonecrosis of The Femoral Headgreg_enricoNo ratings yet
- Prostate and Seminal VesiclesDocument83 pagesProstate and Seminal Vesiclesgreg_enricoNo ratings yet
- Evaluation of Lymphedema in Upper Extremities by MR Lymphangiography Comparison With LymphoscintigraphyDocument26 pagesEvaluation of Lymphedema in Upper Extremities by MR Lymphangiography Comparison With Lymphoscintigraphygreg_enricoNo ratings yet
- Ingles Medico Ii - TP 4Document4 pagesIngles Medico Ii - TP 4Rodrigo Anelli De OliveiraNo ratings yet
- Kapita Selekta ImunologiDocument29 pagesKapita Selekta ImunologiAsyha KantifaNo ratings yet
- HymenectomyDocument5 pagesHymenectomyShamaine limNo ratings yet
- A Simple Classification and A Simplified Treatment's Algorithm For Ptotic BreastsDocument9 pagesA Simple Classification and A Simplified Treatment's Algorithm For Ptotic Breastsmahmoud makramNo ratings yet
- ANGIOLOGYDocument32 pagesANGIOLOGYFaisal IqbalNo ratings yet
- Excretion Human BeingsDocument3 pagesExcretion Human BeingsRahul Ecka100% (1)
- Nursing History and Assessment: A. IntroductionDocument18 pagesNursing History and Assessment: A. IntroductionAmanda ScarletNo ratings yet
- Cranial Nerves Summary PDFDocument9 pagesCranial Nerves Summary PDFMudassar SattarNo ratings yet
- UK UHN Man 2014Document165 pagesUK UHN Man 2014jj_weinsteinNo ratings yet
- Enteric Nervous SystemDocument5 pagesEnteric Nervous Systemmehdi mafakheriNo ratings yet
- Trans Chapter 16Document5 pagesTrans Chapter 16رجمه ديوانNo ratings yet
- The Physiologic Support SystemDocument45 pagesThe Physiologic Support SystemModesto MasangkayNo ratings yet
- Life Processes - Class Notes - Warrior-Life Processes (Samridhi Mam) WarriorDocument162 pagesLife Processes - Class Notes - Warrior-Life Processes (Samridhi Mam) Warriorsiddhesht104No ratings yet
- Full Download Human Physiology From Cells To Systems 7th Edition Sherwood Test Bank Cells To Systems 7th Edition Sherwood Test BankDocument36 pagesFull Download Human Physiology From Cells To Systems 7th Edition Sherwood Test Bank Cells To Systems 7th Edition Sherwood Test Bankgambolrapinous.ggqcdr100% (27)
- Drug ClearanceDocument3 pagesDrug ClearanceARqam MaQsoodNo ratings yet
- 2 NDLPDocument14 pages2 NDLPJennifer Lopez Guiao-Catacutan0% (1)
- Anaphy - Digestive-System-NotesDocument8 pagesAnaphy - Digestive-System-NotesKert trocioNo ratings yet
- Human HeartDocument7 pagesHuman HeartAsher Eby VargeeseNo ratings yet
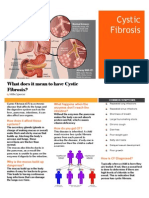
- Cystic Fibrosis Fact SheetDocument2 pagesCystic Fibrosis Fact Sheetmilyspencer86No ratings yet
- AUBF Chapter 3-ReviewerDocument4 pagesAUBF Chapter 3-ReviewerSalvani, Shane JudeNo ratings yet
- Breastfeeding GuidelinesDocument24 pagesBreastfeeding GuidelinesJayanti100% (1)
- General Biology 2: 2 Quarter - Module 2Document2 pagesGeneral Biology 2: 2 Quarter - Module 2Veronica RojasNo ratings yet
- The Autonomic Nervous System and Its Central ControlDocument15 pagesThe Autonomic Nervous System and Its Central Controlpuchio100% (1)
- In Case of Appeal, Go To The Link: Final Result: 80.00 % M/qsy-Zagf-QqhDocument15 pagesIn Case of Appeal, Go To The Link: Final Result: 80.00 % M/qsy-Zagf-QqhnNo ratings yet
- Objective Test - 1: TOPIC: 1. Respiratory System 2. Circulatory System MM:50Document6 pagesObjective Test - 1: TOPIC: 1. Respiratory System 2. Circulatory System MM:50Jaskirat SinghNo ratings yet
- Las 1Document5 pagesLas 1rosemarie lingonNo ratings yet
- Vaginal MassDocument12 pagesVaginal MassShem DelolaNo ratings yet
- Lesson 4 - Circulatory SystemDocument21 pagesLesson 4 - Circulatory Systemapi-307592530No ratings yet
- Urinary System: Tsedalu Yirsa (DVM, MSC, Assist Prof.)Document18 pagesUrinary System: Tsedalu Yirsa (DVM, MSC, Assist Prof.)Mohammed OumerNo ratings yet