You might also like
- Stroke Topic DiscussionDocument19 pagesStroke Topic Discussionapi-648714317No ratings yet
- Rolling Stock Design CriteriaDocument17 pagesRolling Stock Design CriteriahamzaNo ratings yet
- Which Statement On Physical Development of Infants and Toddlers Is TRUEDocument9 pagesWhich Statement On Physical Development of Infants and Toddlers Is TRUEKristylle Renz100% (1)
- Sds d201 Diatro - Lyse-Diff v4.1Document7 pagesSds d201 Diatro - Lyse-Diff v4.1Fauzia BudimanNo ratings yet
- DR Huma NstemiDocument114 pagesDR Huma NstemiArzalan BaigNo ratings yet
- Dual Antiplatelet Therapy After PCI in Patients atDocument32 pagesDual Antiplatelet Therapy After PCI in Patients atyamonaelgamNo ratings yet
- Clopidogrel Plus Aspirin Vs Aspirin Alone For Acute Minor Ischaemic Stroke or High Risk TIA: Systematic Review and Meta-AnalysisDocument25 pagesClopidogrel Plus Aspirin Vs Aspirin Alone For Acute Minor Ischaemic Stroke or High Risk TIA: Systematic Review and Meta-AnalysisMaryam RehmanNo ratings yet
- BrilintaDocument16 pagesBrilintaWilliam ClarkNo ratings yet
- BMJ l2211 Full PDFDocument11 pagesBMJ l2211 Full PDFdhea handyaraNo ratings yet
- Clopidogrel Clinical Evidence in Cerebrovascular Disease and PCIDocument51 pagesClopidogrel Clinical Evidence in Cerebrovascular Disease and PCIward2713No ratings yet
- Beta Blocker in Heart Failure TrailDocument31 pagesBeta Blocker in Heart Failure Trailgovind rajNo ratings yet
- POINT TrialDocument27 pagesPOINT TrialRutaNo ratings yet
- Ticagrelor PDFDocument7 pagesTicagrelor PDFNurul Masyithah100% (1)
- White 2012 Champion PooledDocument13 pagesWhite 2012 Champion PooledRadu CiprianNo ratings yet
- BMJ l2211 FullDocument11 pagesBMJ l2211 FullOeij Henri WijayaNo ratings yet
- Nejmoa 010746Document9 pagesNejmoa 010746Mmle BlaséNo ratings yet
- CYP450 System and Not BeingDocument5 pagesCYP450 System and Not BeingArfa'i LaksamanaNo ratings yet
- Perioperative Management of Antiplatelet Therapy in Patients With Coronary Artery StentsDocument31 pagesPerioperative Management of Antiplatelet Therapy in Patients With Coronary Artery StentskitsilcNo ratings yet
- MIMS Doctor November 2016 RGDocument36 pagesMIMS Doctor November 2016 RGDarmawan HariyantoNo ratings yet
- Acs 11 190524110746Document46 pagesAcs 11 190524110746Obakeng MandaNo ratings yet
- Clopidogrel: 26% More Effective than AspirinDocument30 pagesClopidogrel: 26% More Effective than AspirinMuhammad Yolandi SumadioNo ratings yet
- DAPA HF Journal ClubDocument29 pagesDAPA HF Journal ClubRIJO CHERIANNo ratings yet
- Journal Reading Clopi Aspirin FinalDocument49 pagesJournal Reading Clopi Aspirin FinalWenny AnggonoNo ratings yet
- Thrombolytic Therapy in Emergency MedicineDocument8 pagesThrombolytic Therapy in Emergency MedicinemedeviNo ratings yet
- Bivalirudin Versus Unfractionated Heparin During Percutaneous Coronary InterventionDocument22 pagesBivalirudin Versus Unfractionated Heparin During Percutaneous Coronary InterventionHafeesh FazuluNo ratings yet
- Journal Club Handout FinalDocument5 pagesJournal Club Handout Finaltcd_usaNo ratings yet
- Nejmc 0909586Document4 pagesNejmc 0909586theboy14juneNo ratings yet
- Brjclinpharm00184 0007Document6 pagesBrjclinpharm00184 0007Helmi AdisafitriNo ratings yet
- Intensive Versus Moderate Lipid Lowering With Statins After Acute Coronary SyndromesDocument43 pagesIntensive Versus Moderate Lipid Lowering With Statins After Acute Coronary Syndromeskjrunner2No ratings yet
- CLOPIDOGRELDocument4 pagesCLOPIDOGRELHuseikha VelayazulfahdNo ratings yet
- Neuro - Jurding - TIA Minor StrokeDocument23 pagesNeuro - Jurding - TIA Minor StrokesalfarinaNo ratings yet
- Editorial 2Document4 pagesEditorial 2david1086No ratings yet
- Prologhed TherapyDocument5 pagesProloghed TherapyNagatzulNo ratings yet
- Version of Record:: ManuscriptDocument23 pagesVersion of Record:: Manuscriptmiko balisiNo ratings yet
- Acute non-ST-elevation acute coronary syndromes: Early antiplatelet therapy (UPTODATE)Document27 pagesAcute non-ST-elevation acute coronary syndromes: Early antiplatelet therapy (UPTODATE)kabulkabulovich5No ratings yet
- Circinterventions 113 000512Document9 pagesCircinterventions 113 000512jackytungadiNo ratings yet
- COMMIT ClopidogrelDocument15 pagesCOMMIT ClopidogrelCristina PazmiñoNo ratings yet
- Antithrombotic Dilemmas in Stroke MedicineDocument43 pagesAntithrombotic Dilemmas in Stroke MedicineGopi Krishnan RNo ratings yet
- Antiplatelet Therapy: New Antiplatelet Drugs in PerspectiveDocument4 pagesAntiplatelet Therapy: New Antiplatelet Drugs in Perspectivegeo_mmsNo ratings yet
- Interventional Cardiology Board Review (PDFDrive)Document62 pagesInterventional Cardiology Board Review (PDFDrive)wasimNo ratings yet
- Antiplatelet Agents in Acute Non-ST Elevation Acute Coronary SyndromesDocument31 pagesAntiplatelet Agents in Acute Non-ST Elevation Acute Coronary SyndromesCésar Santis FuentesNo ratings yet
- 1 s2.0 S0735109708008656 MainDocument10 pages1 s2.0 S0735109708008656 MainraniahNo ratings yet
- Anti-Platelet Agents: A Review of Aspirin, P2Y12 Inhibitors, and GpIIb/IIIa InhibitorsDocument61 pagesAnti-Platelet Agents: A Review of Aspirin, P2Y12 Inhibitors, and GpIIb/IIIa InhibitorsKshitizma GiriNo ratings yet
- Eficacia Del Clopidogrel en Pacientes Con Fibrilacion Auricular y Sindrome Coronario AgudoDocument7 pagesEficacia Del Clopidogrel en Pacientes Con Fibrilacion Auricular y Sindrome Coronario AgudoElva MonserrathNo ratings yet
- Pegasus TIMI 54 TrialDocument13 pagesPegasus TIMI 54 TrialIsaac Aaron Enriquez MonsalvoNo ratings yet
- Furtado 2016Document10 pagesFurtado 2016zzzzNo ratings yet
- Steroids in Cardiac SurgeryDocument52 pagesSteroids in Cardiac SurgeryKarthik RamanNo ratings yet
- Stemi Vs NstemiDocument31 pagesStemi Vs NstemiFadhilAfifNo ratings yet
- Antithrombotic Treatment of Acute Ischemic Stroke and Transient Ischemic Attack - UpToDateDocument24 pagesAntithrombotic Treatment of Acute Ischemic Stroke and Transient Ischemic Attack - UpToDateFerasNo ratings yet
- Acute Coronary SyndrommeDocument50 pagesAcute Coronary SyndrommeAndriani Kemala SariNo ratings yet
- CapricornDocument6 pagesCapricornMarkanthony256No ratings yet
- MRCP 2 Clinical Trial Data MRCP 2Document5 pagesMRCP 2 Clinical Trial Data MRCP 2Yong Fang YueNo ratings yet
- JC Stroke FinalDocument55 pagesJC Stroke FinalPleng WipolkulNo ratings yet
- JNC8 & ChlorthalidoneDocument69 pagesJNC8 & ChlorthalidoneAkansha KalraNo ratings yet
- Thrombectomy Within 8 Hours After Symptom Onset in Ischemic StrokeDocument13 pagesThrombectomy Within 8 Hours After Symptom Onset in Ischemic StrokesirrfsNo ratings yet
- Anti Platelet PreopDocument6 pagesAnti Platelet Preopbrigde_xNo ratings yet
- Evidence Based Stroke Medicine. Evaluating Treatments For Acute Ischaemic Stroke - What Works and What Doesn't?Document32 pagesEvidence Based Stroke Medicine. Evaluating Treatments For Acute Ischaemic Stroke - What Works and What Doesn't?maluku barat dayaNo ratings yet
- Acute Coronary Syndrome & The PLATO Trial: Ticagrelor vs. ClopidogrelDocument42 pagesAcute Coronary Syndrome & The PLATO Trial: Ticagrelor vs. ClopidogrelDedeSumantraNo ratings yet
- 309 Novel Anti-Platelet Agents and AnticoagulantsDocument13 pages309 Novel Anti-Platelet Agents and AnticoagulantsPhani NadellaNo ratings yet
- Antiplatelet Regimens in The Long-Term Secondary Prevention of Transient Ischaemic Attack and Ischaemic Stroke: An Updated Network Meta-AnalysisDocument28 pagesAntiplatelet Regimens in The Long-Term Secondary Prevention of Transient Ischaemic Attack and Ischaemic Stroke: An Updated Network Meta-Analysisnurafriani2No ratings yet
- AtlsDocument32 pagesAtlsMahesh RajwalNo ratings yet
- Clopedrogril MODIFYDocument7 pagesClopedrogril MODIFYUday ChauhanNo ratings yet
- Spectralis Touch Panel Upgrade GuideDocument10 pagesSpectralis Touch Panel Upgrade GuideMohamed AbdulaalNo ratings yet
- Knime SeventechniquesdatadimreductionDocument266 pagesKnime SeventechniquesdatadimreductionramanadkNo ratings yet
- Dezurik Balancing Valves Flow Curve 12quot 300mm 12-30-1jDocument1 pageDezurik Balancing Valves Flow Curve 12quot 300mm 12-30-1jgm_revankar3942No ratings yet
- FB6100 DSCDocument132 pagesFB6100 DSCTahir FadhilNo ratings yet
- Audi A6 Allroad Model 2013 Brochure - 2012.08Document58 pagesAudi A6 Allroad Model 2013 Brochure - 2012.08Arkadiusz KNo ratings yet
- Factors, Impact, Symptoms of NPADocument7 pagesFactors, Impact, Symptoms of NPAMahesh ChandankarNo ratings yet
- Plastipak PresentationDocument28 pagesPlastipak Presentationapi-608970005No ratings yet
- Klubermatic Lubricant DispensersDocument13 pagesKlubermatic Lubricant Dispenserstatankise100% (1)
- Literature Review of ZnoDocument7 pagesLiterature Review of Znoea6mkqw2100% (1)
- Tarbucks: Starbucks Corporation Is An International Coffee and Coffeehouse Chain BasedDocument12 pagesTarbucks: Starbucks Corporation Is An International Coffee and Coffeehouse Chain BasedVenu GopalNo ratings yet
- Glycerol PDFDocument3 pagesGlycerol PDFTushar GaikarNo ratings yet
- How to Compost at Home: A Guide to the BasicsDocument10 pagesHow to Compost at Home: A Guide to the BasicsYeo Choon SengNo ratings yet
- Previews 2013360 PreDocument13 pagesPreviews 2013360 PreEko Setyo BudiNo ratings yet
- Syllabus of Modules FOR THE Electrician Domestic (ELE701)Document6 pagesSyllabus of Modules FOR THE Electrician Domestic (ELE701)udi969100% (1)
- D & C G T G N A. R E S P A, NY 12242: Esign Onstruction Roup HE Overnor Elson Ockefeller Mpire Tate Laza LbanyDocument18 pagesD & C G T G N A. R E S P A, NY 12242: Esign Onstruction Roup HE Overnor Elson Ockefeller Mpire Tate Laza LbanyAlexNo ratings yet
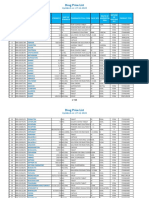
- PPR - LISTS - Registered Medicine Price List - 20221127 BahrainDocument318 pagesPPR - LISTS - Registered Medicine Price List - 20221127 BahrainvdvedNo ratings yet
- MONO POWER AMPLIFIER SERVICE MANUALDocument34 pagesMONO POWER AMPLIFIER SERVICE MANUALAlexey OnishenkoNo ratings yet
- Personal Development Course for Senior High StudentsDocument7 pagesPersonal Development Course for Senior High StudentsLucelle PalarisNo ratings yet
- Chapter 6Document2 pagesChapter 6Zhane CruzNo ratings yet
- Bonding BB1Document3 pagesBonding BB1DeveshNo ratings yet
- Fy em - 1 Question Bank 2023-24Document9 pagesFy em - 1 Question Bank 2023-24raju.sharmqNo ratings yet
- Beta Analytic Presentation at NNFCC Conference - Linking Bio-Based Materials To Renewable Energy ProductionDocument25 pagesBeta Analytic Presentation at NNFCC Conference - Linking Bio-Based Materials To Renewable Energy ProductionBeta AnalyticNo ratings yet
- Urine Eaxmintaion ReportDocument7 pagesUrine Eaxmintaion Reportapi-3745021No ratings yet
- Veena Singh-176-189 - Findings, Implications and ConclusionsDocument14 pagesVeena Singh-176-189 - Findings, Implications and ConclusionsValerine SNo ratings yet
- Refrac 2Document20 pagesRefrac 2PawanNo ratings yet
- AA3 My Favorite City - Comparing Places Ejercicio FinalDocument6 pagesAA3 My Favorite City - Comparing Places Ejercicio FinalCesar Augusto Triana AyalaNo ratings yet
- By Pass System in The Dry ProcessDocument34 pagesBy Pass System in The Dry Processfaheemqc100% (1)