You might also like
- Activity 1Document21 pagesActivity 1Oana RuxandraNo ratings yet
- Sport Injury Rehablitation JPMRDocument22 pagesSport Injury Rehablitation JPMRlilis pratiwiNo ratings yet
- Lower Extremity Perturbation Training.12Document8 pagesLower Extremity Perturbation Training.12Martiniano Vera EnriqueNo ratings yet
- Oints: First Patellar Dislocation: From Conservative Treatment To Return To SportDocument5 pagesOints: First Patellar Dislocation: From Conservative Treatment To Return To SportJuan PalomoNo ratings yet
- Resisted ExerciseDocument29 pagesResisted ExerciseVaraNo ratings yet
- Posture and Factor Affecting Posture in Physical TherapyDocument28 pagesPosture and Factor Affecting Posture in Physical TherapyAnand Vaghasiya100% (2)
- FUNDA - Group 3 Mobility and ActivityDocument30 pagesFUNDA - Group 3 Mobility and ActivityJannah Monaliza BambaNo ratings yet
- Info On AyurvedaDocument1 pageInfo On AyurvedaPriyank JivaniNo ratings yet
- Trunk Stability ProgramDocument16 pagesTrunk Stability ProgramMartinKozjanNo ratings yet
- Kinesiology Ii: Sadia Shaheen Reference Text: Dena Gardiner Semester: Spring 2019Document58 pagesKinesiology Ii: Sadia Shaheen Reference Text: Dena Gardiner Semester: Spring 2019abdulahNo ratings yet
- Physical EducationDocument3 pagesPhysical EducationEuan Marlee F. SampeloNo ratings yet
- Spasticity PPT by Black BabyDocument38 pagesSpasticity PPT by Black BabyChidube UkachukwuNo ratings yet
- Compre Notes!!!!!!!!!!!Document12 pagesCompre Notes!!!!!!!!!!!Cyenel DeiparineNo ratings yet
- Presentación 169 Gimnasia Artística Watercolor Rosa Pastel CoralDocument10 pagesPresentación 169 Gimnasia Artística Watercolor Rosa Pastel CoralLaura Melissa Bravo LaraNo ratings yet
- TX 5 - Short - BDocument29 pagesTX 5 - Short - BDr. Sidra Qureshi100% (1)
- Effect of Core Stabilization Training On Endurance of Trunk Extensor and Functional Capacity in Subjects With Mechanical Low Back PainDocument8 pagesEffect of Core Stabilization Training On Endurance of Trunk Extensor and Functional Capacity in Subjects With Mechanical Low Back PainDr. Krishna N. SharmaNo ratings yet
- Family-Name FITT ARTHRITIS-1Document2 pagesFamily-Name FITT ARTHRITIS-1Kc Mea Paran BorjaNo ratings yet
- Return To Play - A Common Sense Guide For CoachesDocument2 pagesReturn To Play - A Common Sense Guide For CoachesTeo100% (1)
- RESISTANCEDocument5 pagesRESISTANCEJessica LeeNo ratings yet
- Introduction To Physical FitnessDocument6 pagesIntroduction To Physical Fitnessangela raquinNo ratings yet
- NCP Rheumatoid Arthritis DX IpmDocument2 pagesNCP Rheumatoid Arthritis DX IpmPatty RomeroNo ratings yet
- Effect of Trunk Muscles Stabilization Exercises and General Exercises On Disability in Recurrent Non Specific Low Back AcheDocument9 pagesEffect of Trunk Muscles Stabilization Exercises and General Exercises On Disability in Recurrent Non Specific Low Back AcheDr. Krishna N. SharmaNo ratings yet
- Neurorestorasi Untuk Pasien Stroke Fase Post Akut (Pendekatan Konsep PNF)Document43 pagesNeurorestorasi Untuk Pasien Stroke Fase Post Akut (Pendekatan Konsep PNF)lizadwijanuaryanaNo ratings yet
- PNFDocument44 pagesPNFDwaipayan PalNo ratings yet
- Introduction To Orthopaedic Rehabilitation: by Mehar ShaikhDocument8 pagesIntroduction To Orthopaedic Rehabilitation: by Mehar Shaikhshaikhmehar29No ratings yet
- CECS ProtocolDocument6 pagesCECS ProtocolTsz Kwan CheungNo ratings yet
- Impaired Physical MobilityDocument9 pagesImpaired Physical MobilityNurse NotesNo ratings yet
- McKenzie CONCEPT AnilDocument12 pagesMcKenzie CONCEPT AnilSOUMYADEEP BHUINYANo ratings yet
- Pathfit 1Document6 pagesPathfit 1gabosara298No ratings yet
- Physical EducationDocument7 pagesPhysical EducationKristine Anne IgotNo ratings yet
- Strengthening or Resistance ExercisesDocument103 pagesStrengthening or Resistance Exercisesphysio careNo ratings yet
- SpondylolisthesisDocument5 pagesSpondylolisthesisAnuj ShresthaNo ratings yet
- Resistance Exercise For Impaired Muscle Performance - Copy-1Document64 pagesResistance Exercise For Impaired Muscle Performance - Copy-1Messyandelaputrii100% (1)
- PeHealth 1st QTR ReviewerDocument4 pagesPeHealth 1st QTR ReviewerMikaela VargasNo ratings yet
- Strengthening ExerciseDocument34 pagesStrengthening Exercisebdangar677No ratings yet
- Physiotheraphy Role in Pain ManagementDocument63 pagesPhysiotheraphy Role in Pain Management姐姐雯No ratings yet
- General Principle of Sports Injuries Rehabilitation UpdateDocument58 pagesGeneral Principle of Sports Injuries Rehabilitation Updatesuryatmajadr100% (1)
- PNF PrincipalsDocument15 pagesPNF PrincipalsPratibha SalkarNo ratings yet
- Additional Patient PopulationsDocument4 pagesAdditional Patient PopulationsNicole ReidNo ratings yet
- Restoring Rangeof Motionand Improving FlexibilityDocument35 pagesRestoring Rangeof Motionand Improving FlexibilitysharenNo ratings yet
- Finted ExerciseDocument78 pagesFinted ExerciseShivam RavalNo ratings yet
- Introduction To Sports InjuriesDocument31 pagesIntroduction To Sports Injuriesمحمد عقلNo ratings yet
- Muscle Energy TechniqueDocument42 pagesMuscle Energy Techniquebdangar677No ratings yet
- Mattacola & Dwyer (2002) Rehabilitation of The Ankle After Acute Sprain or Chronic Instability PDFDocument17 pagesMattacola & Dwyer (2002) Rehabilitation of The Ankle After Acute Sprain or Chronic Instability PDFisanewtoonNo ratings yet
- Journals Ijatt 11 5 Article-P15-PreviewDocument2 pagesJournals Ijatt 11 5 Article-P15-Previewashlyn granthamNo ratings yet
- A Comparative Study of Standing Balanceperformance Between Oa Knee Patients Compared With Normal Age Matched ControlsDocument11 pagesA Comparative Study of Standing Balanceperformance Between Oa Knee Patients Compared With Normal Age Matched ControlsDr. Krishna N. SharmaNo ratings yet
- Orthopedic Rehabilitation 1 2Document14 pagesOrthopedic Rehabilitation 1 2nanahossam12345No ratings yet
- Groin Pain in Football Players: A Systematic Diagnostic ApproachDocument5 pagesGroin Pain in Football Players: A Systematic Diagnostic ApproachCherbiti Mohammed Amine100% (1)
- Principles of Exercises andDocument14 pagesPrinciples of Exercises andRica Pearl ZorillaNo ratings yet
- Pe & Health Reviewer (1 Periodical) Module 1 Lesson 1: Physical FitnessDocument7 pagesPe & Health Reviewer (1 Periodical) Module 1 Lesson 1: Physical FitnessFitri CeradoNo ratings yet
- Chap 5 Assissted and Resisted ExcercisesDocument19 pagesChap 5 Assissted and Resisted ExcercisesaroojNo ratings yet
- Basic Principles of ExerciseDocument47 pagesBasic Principles of ExerciseAgatha Shaine SanchezNo ratings yet
- Physical Fitness Notes Second AssessmentDocument116 pagesPhysical Fitness Notes Second AssessmentElena JordanovaNo ratings yet
- Group Fitness Instructor University Curriculum: Chapter 8: The Prevention and Management of Common InjuriesDocument34 pagesGroup Fitness Instructor University Curriculum: Chapter 8: The Prevention and Management of Common InjuriesLouis TrầnNo ratings yet
- PNF BasicsDocument38 pagesPNF Basicsbpt2100% (3)
- HOPE-REVIEWER-1STQ (Patricia Doctor)Document4 pagesHOPE-REVIEWER-1STQ (Patricia Doctor)crypt06112No ratings yet
- Intervention: ExerciseDocument9 pagesIntervention: ExerciseAbeer AlasmyNo ratings yet
- A Simple Test For Gauging Recovery & Workout “Readiness” - Based On The Teachings Of Dr. Andrew Huberman: Ready For ActionFrom EverandA Simple Test For Gauging Recovery & Workout “Readiness” - Based On The Teachings Of Dr. Andrew Huberman: Ready For ActionNo ratings yet
- The Mindful Spine: A Holistic Approach to Healing Back PainFrom EverandThe Mindful Spine: A Holistic Approach to Healing Back PainNo ratings yet
- Brain Breakthrough: The Art of Neurological Rehabilitation: Easy and Innovative Techniques, #1From EverandBrain Breakthrough: The Art of Neurological Rehabilitation: Easy and Innovative Techniques, #1No ratings yet
- OptimizedDocument49 pagesOptimizedAlfiya HasnaNo ratings yet
- Fsoc 03 00004Document5 pagesFsoc 03 00004Alfiya HasnaNo ratings yet
- TES Harian: Bahasa InggrisDocument2 pagesTES Harian: Bahasa InggrisSyifaa ZulfikarNo ratings yet
- Jumlah Soal: 10 Butir Passage 1Document4 pagesJumlah Soal: 10 Butir Passage 1Alfiya HasnaNo ratings yet
- TES Harian: Bahasa InggrisDocument2 pagesTES Harian: Bahasa InggrisSyifaa ZulfikarNo ratings yet
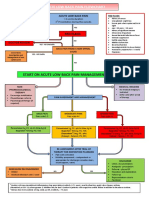
- Acute Low Back Pain Flowchart March 2016Document1 pageAcute Low Back Pain Flowchart March 2016Alfiya HasnaNo ratings yet
- Garuda 971288Document15 pagesGaruda 971288Alfiya HasnaNo ratings yet
- 07 RefrencesDocument4 pages07 RefrencesAlfiya HasnaNo ratings yet
- Soal SIMAK UI 2017 - Bahasa InggrisDocument3 pagesSoal SIMAK UI 2017 - Bahasa InggrisTikNo ratings yet
- SIMAKUI2015ING999 580f768c PDFDocument3 pagesSIMAKUI2015ING999 580f768c PDFxxxanythingxxxNo ratings yet
- SIMAK UI 2018 Bahasa Inggris: Name Doc: SIMAKUI2018ING999 Version: 2019 - 06Document4 pagesSIMAK UI 2018 Bahasa Inggris: Name Doc: SIMAKUI2018ING999 Version: 2019 - 06Noragami Aragoto100% (1)
- SIMAK UI 2013 Bahasa Inggris: Kode SoalDocument4 pagesSIMAK UI 2013 Bahasa Inggris: Kode SoalAlfiya HasnaNo ratings yet
- Bing 2014Document4 pagesBing 2014Novita AnugraheniNo ratings yet
- Soal Simak Ui Inggris 2011Document3 pagesSoal Simak Ui Inggris 2011Alfiya HasnaNo ratings yet
- SIMAK UI 2016 Bahasa Inggris: Text 31-34Document3 pagesSIMAK UI 2016 Bahasa Inggris: Text 31-34Saya SendiriNo ratings yet
- Sima Kui 2010 Ing 307Document4 pagesSima Kui 2010 Ing 307Ratna WiwaraNo ratings yet
- p6 Specific Geriatric Problem 3 (Urinary IncontinenceDocument28 pagesp6 Specific Geriatric Problem 3 (Urinary IncontinenceAlfiya HasnaNo ratings yet
- European Physiotherapy Guideline For Parkinson's PDFDocument191 pagesEuropean Physiotherapy Guideline For Parkinson's PDFAnonymous Da2Idf100% (3)
- Pert 5 - Soft Tissue Damage and HealingDocument41 pagesPert 5 - Soft Tissue Damage and HealingAlfiya HasnaNo ratings yet
- Xpedia Bahasa Inggris: Latihan Soal - SIMAK 1Document4 pagesXpedia Bahasa Inggris: Latihan Soal - SIMAK 1Alfiya HasnaNo ratings yet
- SIMAK UI 2012 Bahasa Inggris: Kode SoalDocument4 pagesSIMAK UI 2012 Bahasa Inggris: Kode SoalsalimNo ratings yet
- Xpedia Bahasa Inggris: Latihan Soal - SIMAK 2Document4 pagesXpedia Bahasa Inggris: Latihan Soal - SIMAK 2Saya SendiriNo ratings yet
- Pert 10 - Core Stability ExerciseDocument30 pagesPert 10 - Core Stability ExerciseAlfiya HasnaNo ratings yet
- Pert 3 - Fisiologi Latihan IIDocument34 pagesPert 3 - Fisiologi Latihan IIAlfiya HasnaNo ratings yet
- SIMAK UI 2016 Bahasa Inggris: Text 31-34Document3 pagesSIMAK UI 2016 Bahasa Inggris: Text 31-34Saya SendiriNo ratings yet
- Soal SIMAK UI 2017 - Bahasa InggrisDocument3 pagesSoal SIMAK UI 2017 - Bahasa InggrisTikNo ratings yet
- 4 - Congenital Heart DefectDocument42 pages4 - Congenital Heart DefectAlfiya HasnaNo ratings yet
- Pert 7 - Pemeriksaan Pada Cedera OlahragaDocument31 pagesPert 7 - Pemeriksaan Pada Cedera OlahragaAlfiya HasnaNo ratings yet
- Bing 2014Document4 pagesBing 2014Novita AnugraheniNo ratings yet
- The Singapore Success StoryDocument14 pagesThe Singapore Success StoryMaria SchiporNo ratings yet
- Joshi - Quant Job InterviewDocument329 pagesJoshi - Quant Job InterviewPiciBivNo ratings yet
- Progresive DPKDocument7 pagesProgresive DPKAmol WalunjNo ratings yet
- Human Relations TheoriesDocument28 pagesHuman Relations TheoriesHarold100% (1)
- M Pump - Plunger 300Document30 pagesM Pump - Plunger 300hebert perezNo ratings yet
- List of ROs Under VODocument74 pagesList of ROs Under VOvivek mishraNo ratings yet
- Egcuwa - Butterworth Profile PDFDocument84 pagesEgcuwa - Butterworth Profile PDFsbuja7No ratings yet
- Principles of Engineering Thermodynamics - SI Version 8th EditionDocument47 pagesPrinciples of Engineering Thermodynamics - SI Version 8th EditionanabNo ratings yet
- Influences of Le Corbusier and Louis I Kahn in IndiaDocument10 pagesInfluences of Le Corbusier and Louis I Kahn in IndiaRashi Chugh88% (8)
- IHS Markit - The Global Ultrasound MarketDocument2 pagesIHS Markit - The Global Ultrasound MarketwwtqfgtpNo ratings yet
- Learning Curves in Manufacturing IndustriesDocument3 pagesLearning Curves in Manufacturing Industriessubhash221103No ratings yet
- Performance Evaluation of TDL Channels For Downlink 5G MIMO SystemsDocument4 pagesPerformance Evaluation of TDL Channels For Downlink 5G MIMO SystemspruxmanNo ratings yet
- Cablemaster RLC - ManualDocument8 pagesCablemaster RLC - ManualGlendinning Products, LLC.No ratings yet
- Action and Event ListenerDocument6 pagesAction and Event ListenerFionaLimYongXinNo ratings yet
- Contrastive Morphology The Morpheme Is The Smallest Unit of A Language That Has A Binary Nature (That CanDocument6 pagesContrastive Morphology The Morpheme Is The Smallest Unit of A Language That Has A Binary Nature (That CanIrynaNo ratings yet
- SACS TrainingDocument4 pagesSACS Trainingasma100% (1)
- GAP Guidelines: Management Programs (Overview)Document27 pagesGAP Guidelines: Management Programs (Overview)LleiLlei100% (1)
- Data Privacy Notice TemplateDocument1 pageData Privacy Notice TemplateangeloNo ratings yet
- Street Rehabilitation Program ReportDocument2 pagesStreet Rehabilitation Program ReportWCPO 9 NewsNo ratings yet
- Sitronix ST7565RDocument72 pagesSitronix ST7565RStuart CouttsNo ratings yet
- CitiBank ApplicationDocument15 pagesCitiBank ApplicationJordan P HunterNo ratings yet
- WESCAM MX-15-0503AA-SpecDocument2 pagesWESCAM MX-15-0503AA-SpecAIT FARIDNo ratings yet
- Application Letter: Jl. Kayu Aya No. 10 A, Kerobokan, Kuta Utara, Badung, BaliDocument3 pagesApplication Letter: Jl. Kayu Aya No. 10 A, Kerobokan, Kuta Utara, Badung, BaliIRMA DAMAYANTINo ratings yet
- Micro SplatDocument17 pagesMicro SplatCarlosAndresGarnicaSalazarNo ratings yet
- Fire Warden Training: Richard Hagger - ConsultantDocument61 pagesFire Warden Training: Richard Hagger - ConsultantRichard Hagger100% (2)
- Er9000en 21204 1.00Document106 pagesEr9000en 21204 1.00Alexandru AnghelNo ratings yet
- Soal Bahasa Inggris KELAS 7 - Uk 9Document2 pagesSoal Bahasa Inggris KELAS 7 - Uk 9Ruli CandraNo ratings yet
- Catalogue - FM-200 PFS - Masteco PDFDocument8 pagesCatalogue - FM-200 PFS - Masteco PDFNguyễn Minh ThiệuNo ratings yet
- Denso Mitsubishi L200 Common Rail PDFDocument53 pagesDenso Mitsubishi L200 Common Rail PDFAlex Renne Chambi100% (8)
- 2D1N Night Nueva VizcayaDocument3 pages2D1N Night Nueva VizcayaKaye RoldanNo ratings yet