You might also like
- Performance Improvement Plan Template 1 - 908445459Document3 pagesPerformance Improvement Plan Template 1 - 908445459api-534828007No ratings yet
- Self Assessment Form (SAF)Document25 pagesSelf Assessment Form (SAF)aringkinkingNo ratings yet
- 2003-2004 Polaris MSX 110 MSX 150 Personal WatercraftDocument241 pages2003-2004 Polaris MSX 110 MSX 150 Personal WatercraftJisu Kim100% (1)
- Pepperfry Turning The Tables of DisruptionDocument9 pagesPepperfry Turning The Tables of DisruptionVijayalakshmi PVNo ratings yet
- Power Point On MU 7-29-10Document24 pagesPower Point On MU 7-29-10dboundsNo ratings yet
- Planning For Successful EHR Adoption: Russell B Leftwich, MDDocument27 pagesPlanning For Successful EHR Adoption: Russell B Leftwich, MDrbleftNo ratings yet
- Interim Final SummaryDocument9 pagesInterim Final SummarycdirksNo ratings yet
- EHR and Meaningful UseDocument4 pagesEHR and Meaningful UseNkeletseng MakakaNo ratings yet
- Meaningful Use of EHR'sDocument4 pagesMeaningful Use of EHR'sAnthony Olushegun OloniNo ratings yet
- AchievingMeaningfulUse Stage2 PDFDocument13 pagesAchievingMeaningfulUse Stage2 PDFAnonymous c0zdLnNo ratings yet
- EMR and Integration April2011 Lynne Zucker enDocument19 pagesEMR and Integration April2011 Lynne Zucker enSteveEpsteinNo ratings yet
- Medicare & Medicaid EHR Incentive Program: Meaningful Use Stage 1 Requirements OverviewDocument33 pagesMedicare & Medicaid EHR Incentive Program: Meaningful Use Stage 1 Requirements OverviewDodie DelosaNo ratings yet
- Meaningful Use Stage 3 Recommendations - 2014!03!11Document17 pagesMeaningful Use Stage 3 Recommendations - 2014!03!11bgrabberNo ratings yet
- Test Procedure For 170.314 (B) (7) Data PortabilityDocument19 pagesTest Procedure For 170.314 (B) (7) Data PortabilitySpit FireNo ratings yet
- Quality AssuranceDocument43 pagesQuality Assurancekanika100% (1)
- What Is Meaningful Use: Core Set: All 15 Measures RequiredDocument3 pagesWhat Is Meaningful Use: Core Set: All 15 Measures Requiredapi-101814919No ratings yet
- Draft For Hit Policy Committee ApprovalDocument12 pagesDraft For Hit Policy Committee Approvalapi-30170511No ratings yet
- Team Application Project 1 - GRP 5Document32 pagesTeam Application Project 1 - GRP 5api-660362440No ratings yet
- QUality Officer and Audit Officer Roles ResponsibilitiesDocument4 pagesQUality Officer and Audit Officer Roles ResponsibilitiesSrinivas PolikepatiNo ratings yet
- 10clinicalqualitymeasures CqmsDocument1 page10clinicalqualitymeasures Cqmsapi-101814919No ratings yet
- 2015 Edition Proposed RuleDocument59 pages2015 Edition Proposed RuleVaibhav RaiNo ratings yet
- Chapter 8Document30 pagesChapter 8ankitmanash0% (1)
- The PhilCAT Certification Self-Assessment and Survey Tool (Repaired) FinALDocument25 pagesThe PhilCAT Certification Self-Assessment and Survey Tool (Repaired) FinALMark Johnuel Duavis93% (14)
- ONC Notice of Proposed Ruling Making Stage 2 Certification Rule Fact SheetDocument3 pagesONC Notice of Proposed Ruling Making Stage 2 Certification Rule Fact SheetEmilioCruzFernandezNo ratings yet
- Behnke 4Document87 pagesBehnke 4Thuy NguyenNo ratings yet
- Dr. Ashraf Ismail PresentationDocument85 pagesDr. Ashraf Ismail PresentationBudi YunantoNo ratings yet
- Orientation On Hospital Scorecard Indicators, Rating Scale and Performance Data 11152021Document39 pagesOrientation On Hospital Scorecard Indicators, Rating Scale and Performance Data 11152021Genn Medrano GirayNo ratings yet
- Dr.I.Selvaraj, I.R.M.S: B.SC., M.B.B.S., (M.D, Community Medicine) ., D.P.H.,D.I.H.,PGCH&FW (NIHFW, New Delhi)Document61 pagesDr.I.Selvaraj, I.R.M.S: B.SC., M.B.B.S., (M.D, Community Medicine) ., D.P.H.,D.I.H.,PGCH&FW (NIHFW, New Delhi)Mushtaq MalikNo ratings yet
- Policy and Procedure With The Steps Involved in Jcaho's CycleDocument15 pagesPolicy and Procedure With The Steps Involved in Jcaho's Cycleالمعتزبالله جاب اللهNo ratings yet
- ISO 22000-2018 Workshop Newh PDFDocument114 pagesISO 22000-2018 Workshop Newh PDFNewhame DagneNo ratings yet
- Why Is It Important To Get The PatientDocument3 pagesWhy Is It Important To Get The PatienthodaNo ratings yet
- 2015 Fdacms JWDocument30 pages2015 Fdacms JWDholakiaNo ratings yet
- ISB - Mount Auburn - D8Document2 pagesISB - Mount Auburn - D8Kushal KothariNo ratings yet
- Health Facility Surveys and Quantified Supervisory ChecklistsDocument26 pagesHealth Facility Surveys and Quantified Supervisory ChecklistsEzra AnyalaNo ratings yet
- Ched Memorandum ORDER 06 S. 2008: Medical Technology LawsDocument15 pagesChed Memorandum ORDER 06 S. 2008: Medical Technology LawsAngelica Parreñas BayonaNo ratings yet
- Prognocis Meaningful Use GuidelinesDocument57 pagesPrognocis Meaningful Use GuidelinesKay MercadoNo ratings yet
- Electronic Laboratory Reporting (ELR)Document3 pagesElectronic Laboratory Reporting (ELR)Spit FireNo ratings yet
- Module Title: - Applying Quality Control TTLM Code: TTLM 0919V1Document60 pagesModule Title: - Applying Quality Control TTLM Code: TTLM 0919V1ahmed tofikNo ratings yet
- Quality ImprovementDocument3 pagesQuality ImprovementViky SinghNo ratings yet
- EHR Meaningful Use Guide PDFDocument24 pagesEHR Meaningful Use Guide PDFSpit FireNo ratings yet
- ICH Q12 (Pharmaceutical Product Lifecycle Management) : Current Status and Future PerspectivesDocument23 pagesICH Q12 (Pharmaceutical Product Lifecycle Management) : Current Status and Future PerspectivesrezaNo ratings yet
- Standard Operating ProcedureDocument39 pagesStandard Operating ProcedureAndrew Charles0% (1)
- Nauman Khan CV May 2022Document5 pagesNauman Khan CV May 2022nomankhanNo ratings yet
- Brenda Creaney PresentationDocument21 pagesBrenda Creaney Presentationmonir61No ratings yet
- Notice of Sampling Rules For BTEC Standards Verification 2Document3 pagesNotice of Sampling Rules For BTEC Standards Verification 2wellingqnNo ratings yet
- ISO 15189 - 2012 Management RequirementsDocument56 pagesISO 15189 - 2012 Management RequirementsAhmed AdemNo ratings yet
- Introduction and Update On ICH Q12 GuidelineDocument16 pagesIntroduction and Update On ICH Q12 GuidelineDimitris PapamatthaiakisNo ratings yet
- Materi 10 Indicator Dan Kriteria RSDocument26 pagesMateri 10 Indicator Dan Kriteria RSapi-3756301100% (2)
- Eligible Professional Meaningful Use Core Measures Measure 12 of 13Document3 pagesEligible Professional Meaningful Use Core Measures Measure 12 of 13Sui NarcanNo ratings yet
- General Principles: EvaluationDocument5 pagesGeneral Principles: EvaluationShania SarciaNo ratings yet
- CBAHIDocument54 pagesCBAHIHappy Deal100% (2)
- Rekam Medis ElektronikDocument3 pagesRekam Medis ElektronikDwi JokoNo ratings yet
- Standart Alpha 2Document15 pagesStandart Alpha 2Andreas AraydiaNo ratings yet
- Eligible Professional Meaningful Use Core Measures Measure 10 of 14Document3 pagesEligible Professional Meaningful Use Core Measures Measure 10 of 14kamayani_prNo ratings yet
- Project FinalDocument9 pagesProject FinalPriyanka WankhedeNo ratings yet
- Transducers-Point of Control InstrumentationDocument8 pagesTransducers-Point of Control InstrumentationAnkit AsatiNo ratings yet
- 3) FAAS 608 - Week 5Document56 pages3) FAAS 608 - Week 5Online NinaNo ratings yet
- Assessment Checklist For Laboratory AccreditationDocument46 pagesAssessment Checklist For Laboratory AccreditationJeji HirboraNo ratings yet
- CPMACourse SyllabusDocument3 pagesCPMACourse Syllabuschaitanya varmaNo ratings yet
- 10 Verification of Model FacilitiesDocument21 pages10 Verification of Model FacilitiesayeleNo ratings yet
- 3 Tuazon J p67136 1Document43 pages3 Tuazon J p67136 1Yin ApuradaNo ratings yet
- Measuring Quality Improvement in Healthcare: A Guide to Statistical Process Control ApplicationsFrom EverandMeasuring Quality Improvement in Healthcare: A Guide to Statistical Process Control ApplicationsNo ratings yet
- Understanding and Engaging Today's Real Estate AgentDocument25 pagesUnderstanding and Engaging Today's Real Estate AgentDan KellyNo ratings yet
- Is What We Do: Updating YouDocument17 pagesIs What We Do: Updating YouDan KellyNo ratings yet
- Project Name: Project Logo or Icon, If DesiredDocument17 pagesProject Name: Project Logo or Icon, If DesiredDan KellyNo ratings yet
- How To Implement EcmDocument54 pagesHow To Implement EcmDan KellyNo ratings yet
- 2014 Fsa ArcplcDocument79 pages2014 Fsa ArcplcDan KellyNo ratings yet
- Project Kick Off: Development of Administrative Systems IT Master PlanDocument12 pagesProject Kick Off: Development of Administrative Systems IT Master PlanDan KellyNo ratings yet
- HF Job Support 30 60 90 Day Plan 02282015Document22 pagesHF Job Support 30 60 90 Day Plan 02282015happiest1No ratings yet
- Money Management Skills: - Must Be Coordinated With Needs, Goals, and Personal SituationDocument24 pagesMoney Management Skills: - Must Be Coordinated With Needs, Goals, and Personal SituationDan KellyNo ratings yet
- ArchitectureDocument58 pagesArchitectureDan KellyNo ratings yet
- Business Case ProcessDocument15 pagesBusiness Case ProcessDan KellyNo ratings yet
- Architectural Drawing: Class Orientation/Intro To ArchitectureDocument10 pagesArchitectural Drawing: Class Orientation/Intro To ArchitectureDan KellyNo ratings yet
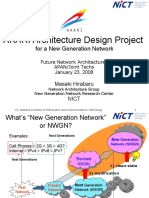
- AKARI Architecture Design Project: For A New Generation NetworkDocument10 pagesAKARI Architecture Design Project: For A New Generation NetworkDan KellyNo ratings yet
- Design PortfolioDocument20 pagesDesign PortfolioArda ÖzdemirNo ratings yet
- C Programm FilesDocument34 pagesC Programm FilesFaizul RazaNo ratings yet
- How To - Oscam Compile TutorialDocument5 pagesHow To - Oscam Compile TutorialDot-InsightNo ratings yet
- Cal311 MCQDocument4 pagesCal311 MCQsanjeevNo ratings yet
- Md. Iftekharul Islam Sakib: Lecturer Cse, BuetDocument38 pagesMd. Iftekharul Islam Sakib: Lecturer Cse, BuetMd. MoniruzzamanNo ratings yet
- Steel-Concrete Composite Bridges: Design, Life Cycle Assessment, Maintenance, and Decision-MakingDocument14 pagesSteel-Concrete Composite Bridges: Design, Life Cycle Assessment, Maintenance, and Decision-MakingNicholas FeatherstonNo ratings yet
- Programmable Controller MCX20B: Technical BrochureDocument6 pagesProgrammable Controller MCX20B: Technical Brochurexie samNo ratings yet
- Fintechinternshipdefenseslides2000 180511165636 PDFDocument40 pagesFintechinternshipdefenseslides2000 180511165636 PDFSadman Abrar RaiyanNo ratings yet
- Restart Class 4 Term 2Document2 pagesRestart Class 4 Term 2sebastinNo ratings yet
- 01 BUQS3011 IntroductionDocument6 pages01 BUQS3011 IntroductionMark EliasNo ratings yet
- MacBook Pro - Apple (UK)Document5 pagesMacBook Pro - Apple (UK)Costinel NeguraNo ratings yet
- Android Application Security Testing Guide-1Document13 pagesAndroid Application Security Testing Guide-1jrcNo ratings yet
- LPV MuliplierDocument22 pagesLPV Muliplierprathap_somaNo ratings yet
- SLX 9540 Switch Data SheetDocument8 pagesSLX 9540 Switch Data SheetKharisma MuhammadNo ratings yet
- Present Professional ExperienceDocument3 pagesPresent Professional Experiencerahul srivastavaNo ratings yet
- Dunn ComplaintDocument144 pagesDunn ComplaintHunter CookeNo ratings yet
- B Qradar Users GuideDocument226 pagesB Qradar Users GuideSandeepKumarNo ratings yet
- @vtucode - in Model Paper 2018 Scheme Set 2 DBMSDocument3 pages@vtucode - in Model Paper 2018 Scheme Set 2 DBMSAstra DemonNo ratings yet
- Performance Benchmarking With Big Data: A Case Study On Fleet Benchmarking With TelematicsDocument23 pagesPerformance Benchmarking With Big Data: A Case Study On Fleet Benchmarking With TelematicsDario Cardona SosaNo ratings yet
- Performance Task No. 1 (50 PTS.) : Category Excellent (10 - 9) Good (8 - 7) Fair (6 - 4) Poor (3 - 1) ScoreDocument2 pagesPerformance Task No. 1 (50 PTS.) : Category Excellent (10 - 9) Good (8 - 7) Fair (6 - 4) Poor (3 - 1) ScoreJeffrey NegroNo ratings yet
- Nx-3060-G7 Specification: Model Nutanix: Per Node ( (4) Per Block) NX-3060-G7 (Configure To Order)Document2 pagesNx-3060-G7 Specification: Model Nutanix: Per Node ( (4) Per Block) NX-3060-G7 (Configure To Order)Aldo PalominoNo ratings yet
- Ccent Icnd 1Document2 pagesCcent Icnd 1Dandy GonzálezNo ratings yet
- Nybc Graphic 2005Document26 pagesNybc Graphic 2005Durga Sai AluriNo ratings yet
- Grade 12 Step Ahead L.O. LEARNER SUPPORT MATERIAL FOR 2021 4Document47 pagesGrade 12 Step Ahead L.O. LEARNER SUPPORT MATERIAL FOR 2021 4SphumeleleNo ratings yet
- SMEA Narrative ReportDocument2 pagesSMEA Narrative ReportTam FerrolNo ratings yet
- Az 900Document2 pagesAz 900Vadivel KmNo ratings yet
- BoyceODEch2s2p27 PDFDocument3 pagesBoyceODEch2s2p27 PDFHelalNo ratings yet
- A319/A320/A321 Airbus: Power Plant 71 80Document318 pagesA319/A320/A321 Airbus: Power Plant 71 80Geovanni Riquelme LooNo ratings yet