You might also like
- Case 21Document45 pagesCase 21Mark GironNo ratings yet
- The Credibility of Newspapers TV News and Online News PDFDocument35 pagesThe Credibility of Newspapers TV News and Online News PDFSimina Stana100% (1)
- Applied Mechanics: by Dr. H. J. Shah & S. B. JunnarkarDocument4 pagesApplied Mechanics: by Dr. H. J. Shah & S. B. Junnarkarvu minhNo ratings yet
- Wolfson Eup3 Ch26 Test BankDocument43 pagesWolfson Eup3 Ch26 Test BankifghelpdeskNo ratings yet
- Career Day Proposal 2Document8 pagesCareer Day Proposal 2Anonymous f3dmav61M100% (1)
- Anemia Dan Klasifikasi (Pada Orang Dewasa)Document60 pagesAnemia Dan Klasifikasi (Pada Orang Dewasa)okta sariya putriNo ratings yet
- Lecture 3rd. AnemiaDocument39 pagesLecture 3rd. Anemiaعمیرسعید قاضیNo ratings yet
- AnaesthesiaDocument121 pagesAnaesthesiaSandeep Bhangale100% (1)
- Week 1: Feeling Tired: Haematopoietic SystemDocument6 pagesWeek 1: Feeling Tired: Haematopoietic SystemPatrick TanNo ratings yet
- Anemia (: /Ə Ni Miə/ Also Spelled Greek Red Blood Cells HemoglobinDocument13 pagesAnemia (: /Ə Ni Miə/ Also Spelled Greek Red Blood Cells HemoglobinAryana BudiawanNo ratings yet
- Systematic Plan For The Diagnosis of AnaemiaDocument31 pagesSystematic Plan For The Diagnosis of AnaemiaAriyike OmoobaNo ratings yet
- 21 Anaemia and PancytopeniaDocument42 pages21 Anaemia and PancytopeniaLeon Hui MingNo ratings yet
- PejowebApproach To Anemia by Dr. Joel Solorzani RomeroDocument57 pagesPejowebApproach To Anemia by Dr. Joel Solorzani RomeroAshraf FaragNo ratings yet
- Anemia (Pronounced: o o o o o o oDocument12 pagesAnemia (Pronounced: o o o o o o opamela100181No ratings yet
- AnaemiaDocument34 pagesAnaemiadakshpanchal26369No ratings yet
- Approach To Anemia and PolycythemiaDocument7 pagesApproach To Anemia and PolycythemiaambutlangnimoNo ratings yet
- Red Cell DisorderDocument43 pagesRed Cell DisorderYuliusDenisChrismaajiNo ratings yet
- Case 18 Anemia-1Document10 pagesCase 18 Anemia-1ngNo ratings yet
- Anaemia: What Is Anemia?Document21 pagesAnaemia: What Is Anemia?Rashed ShatnawiNo ratings yet
- AnemiaDocument14 pagesAnemiaHermawan HmnNo ratings yet
- Anemia NotesDocument6 pagesAnemia NotesElstella Eguavoen Ehicheoya100% (2)
- Red Cell Disorders: Excellent in Quality, Competitiveness, and CareDocument43 pagesRed Cell Disorders: Excellent in Quality, Competitiveness, and CareDeriven Teweng0% (1)
- AnemiaDocument21 pagesAnemiaMarie WagasNo ratings yet
- LP AnemiaDocument10 pagesLP AnemiaDwiyanthi KartikaNo ratings yet
- Hematologic System, Oncologic Disorders & Anemias: Oded Sumarna M KepDocument68 pagesHematologic System, Oncologic Disorders & Anemias: Oded Sumarna M KepUlfalutfiaNo ratings yet
- Automatical Counting Units Measure-Ment Normal Level Short FormDocument35 pagesAutomatical Counting Units Measure-Ment Normal Level Short FormCarolina TulanNo ratings yet
- NCM103 9th Hema IDocument10 pagesNCM103 9th Hema IKamx MohammedNo ratings yet
- Anemia, Disorders of Platelets, Blood Vessels and CoagulationsDocument154 pagesAnemia, Disorders of Platelets, Blood Vessels and CoagulationsVanessa ChavezNo ratings yet
- Anemia and Its Oral MenifestationsDocument74 pagesAnemia and Its Oral MenifestationsBushra FaheemNo ratings yet
- AnemiaDocument6 pagesAnemiaGladz DomingoNo ratings yet
- Normocytic AnemiaDocument16 pagesNormocytic AnemiaPaula ArayaNo ratings yet
- Fbs Anemia 2011Document18 pagesFbs Anemia 2011bagir_dm10No ratings yet
- Anemia in SurgeryDocument29 pagesAnemia in SurgeryEdwin OkonNo ratings yet
- Advanced Med Surg Final Part 2 Everything ElseDocument25 pagesAdvanced Med Surg Final Part 2 Everything Elsejenn1722100% (1)
- Drowsiness Lethargy Tiredness Malaise Listlessness Weakness Muscular WeaknessDocument4 pagesDrowsiness Lethargy Tiredness Malaise Listlessness Weakness Muscular WeaknessCiariz CharisseNo ratings yet
- Hemolytic AnemiaDocument9 pagesHemolytic AnemiaTheeya QuigaoNo ratings yet
- Abnormalities of Haematopoiesis and Blood DisordersDocument51 pagesAbnormalities of Haematopoiesis and Blood DisordersRenad AlharbiNo ratings yet
- Anemia OsamaDocument57 pagesAnemia Osamaosamafoud7710No ratings yet
- An Approach To Anemic PatientDocument79 pagesAn Approach To Anemic PatientHussain AzharNo ratings yet
- Red Blood Cell DisordersDocument56 pagesRed Blood Cell DisordersMunawar Adhar100% (4)
- Anemia: Anemia (Pronounced /Ə Ni Miə/, Also Spelled Anaemia or Anæmia From AncientDocument14 pagesAnemia: Anemia (Pronounced /Ə Ni Miə/, Also Spelled Anaemia or Anæmia From AncientSarvesh JaiswalNo ratings yet
- Chapter Two Anemiarev - ATDocument153 pagesChapter Two Anemiarev - ATAemro TadeleNo ratings yet
- Anemia GDocument47 pagesAnemia GkalfNo ratings yet
- Lecture 3Document11 pagesLecture 3Jireh Vien AtienzaNo ratings yet
- Hemolytic AnemiaDocument6 pagesHemolytic AnemiaLupita Yessica Tarigan0% (1)
- Approach To Anemia in ChildrenDocument16 pagesApproach To Anemia in Childrenduoltut11No ratings yet
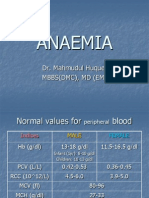
- Anaemia: Dr. Mahmudul Huque. Mbbs (DMC), MD (Em)Document32 pagesAnaemia: Dr. Mahmudul Huque. Mbbs (DMC), MD (Em)Junayed Safar MahmudNo ratings yet
- Hema II Chapter 3 - Anemiarev - ATDocument154 pagesHema II Chapter 3 - Anemiarev - AThannigadah7No ratings yet
- Case Study #1Document35 pagesCase Study #1Muhammad yahyaNo ratings yet
- Anemia 1Document104 pagesAnemia 1maryam ijazNo ratings yet
- KMU Blood DisorderDocument43 pagesKMU Blood DisorderSHAFIQNo ratings yet
- Adrian Hardec Nasdal Modul 6 LBM 2Document9 pagesAdrian Hardec Nasdal Modul 6 LBM 2Rizqon Yassir KuswondoNo ratings yet
- Aplastic AnemiaDocument10 pagesAplastic Anemiagroup1iiistomatologyNo ratings yet
- Aplastic AnemiaDocument11 pagesAplastic AnemiaToni Shiraishi-Aque RuizNo ratings yet
- Anemia: Dr. Tanbira Alam MBBS, M.PhilDocument22 pagesAnemia: Dr. Tanbira Alam MBBS, M.Philsatvindar_muNo ratings yet
- Hematology: Hematocrit (HCT)Document4 pagesHematology: Hematocrit (HCT)Myron RoseNo ratings yet
- Erythrocyte DisordersDocument113 pagesErythrocyte Disordersbewildered-escapist-4301No ratings yet
- AnemiaDocument10 pagesAnemiaGulzada ShadymanovaNo ratings yet
- MK Hematology-AnemiasDocument86 pagesMK Hematology-AnemiasMoses Jr KazevuNo ratings yet
- Pharmacotherapy of Hematological Disorders by Hailu C. (Asst - Prof)Document132 pagesPharmacotherapy of Hematological Disorders by Hailu C. (Asst - Prof)Esubalew TeshomeNo ratings yet
- Anemia OsamaDocument57 pagesAnemia Osamaosamafoud7710No ratings yet
- A Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Air & Gases1 PDFDocument9 pagesAir & Gases1 PDFAnonymous 7CnBF0cjNo ratings yet
- Cohen's Kappa: Measurement in Health and DiseaseDocument11 pagesCohen's Kappa: Measurement in Health and DiseaseAnonymous 7CnBF0cjNo ratings yet
- Journal ClubDocument5 pagesJournal ClubAnonymous 7CnBF0cjNo ratings yet
- September PresentationsDocument1 pageSeptember PresentationsAnonymous 7CnBF0cjNo ratings yet
- Salutogenic Concept of HealthDocument15 pagesSalutogenic Concept of HealthAnonymous 7CnBF0cj100% (1)
- Blood and Blood-Forming Organs Diseases and DisordersDocument48 pagesBlood and Blood-Forming Organs Diseases and DisordersAnonymous 7CnBF0cj100% (1)
- Cot 1 EnglishDocument5 pagesCot 1 EnglishLeonila BaronaNo ratings yet
- Mystic Monk CoffeeDocument4 pagesMystic Monk CoffeeVignesh KivickyNo ratings yet
- (SPROUTFROMGROUND) Đề Chuyên Anh Vĩnh Phúc 2020 2021Document6 pages(SPROUTFROMGROUND) Đề Chuyên Anh Vĩnh Phúc 2020 2021Hội LêNo ratings yet
- Molecular Basis of InheritanceDocument7 pagesMolecular Basis of InheritancePralex PrajapatiNo ratings yet
- A Letter Present Simple or Contionuous Grammar Drills Reading Comprehension Exercises Tes - 76626Document1 pageA Letter Present Simple or Contionuous Grammar Drills Reading Comprehension Exercises Tes - 76626romina acostaNo ratings yet
- A New MasculinityDocument7 pagesA New Masculinityfunkcombu100% (1)
- Paige Decker ResumeDocument1 pagePaige Decker Resumeapi-544654960No ratings yet
- Letter Feeding ProgramDocument3 pagesLetter Feeding ProgramLADY FAME ABUGANNo ratings yet
- State-Wise Result (Written) of Rimc Entrance Examination Dec 2021 For The Term Commencing Jul 2022Document62 pagesState-Wise Result (Written) of Rimc Entrance Examination Dec 2021 For The Term Commencing Jul 2022Pradeep KumarNo ratings yet
- PunzalanJulia RRLDocument5 pagesPunzalanJulia RRLJulia PunzalanNo ratings yet
- LiteratureDocument76 pagesLiteratureMhel FelicesNo ratings yet
- Violation of Ra 9165 Durag LawDocument20 pagesViolation of Ra 9165 Durag LawPortia En Shakespeare IINo ratings yet
- EndnoteDocument4 pagesEndnoteManisha SinghNo ratings yet
- The Kalachakra Shambhala Library PDFDocument28 pagesThe Kalachakra Shambhala Library PDFMichaelNo ratings yet
- COMPEN Reflective Arifah PDFDocument10 pagesCOMPEN Reflective Arifah PDFSyazwani OmarNo ratings yet
- Grammar in The Real Have You Ever Reconnected With Someone From Your Past?Document4 pagesGrammar in The Real Have You Ever Reconnected With Someone From Your Past?Jhonnyer AlvarezNo ratings yet
- 書培建光住診Document42 pages書培建光住診peipeipoorNo ratings yet
- After School Satan Club Permission SlipDocument1 pageAfter School Satan Club Permission SlipBen BraschNo ratings yet
- Homework Es Countable or UncountableDocument5 pagesHomework Es Countable or Uncountableafetqlyme100% (1)
- SFEDI Level 2 Certificate in Preparing To Start Your Own BusinessDocument2 pagesSFEDI Level 2 Certificate in Preparing To Start Your Own Businessapi-152988431No ratings yet
- Operation List SPEED7 Studio PDFDocument1,079 pagesOperation List SPEED7 Studio PDFalinupNo ratings yet
- Pulp Fiction I PDFDocument4 pagesPulp Fiction I PDFPedro GuimarãesNo ratings yet
- Scalpture WikiDocument117 pagesScalpture WikimagusradislavNo ratings yet
- Local Retailer AgreementDocument10 pagesLocal Retailer AgreementIvy Maines DiazNo ratings yet
- Law of ContractDocument20 pagesLaw of ContractUtsav VermaNo ratings yet
- PreliminaryDocument187 pagesPreliminaryJuani Erica GastónNo ratings yet