You might also like
- Anemia NotesDocument6 pagesAnemia NotesElstella Eguavoen Ehicheoya100% (2)
- Dr. Sailendra Nayak Assistant Professor MedicineDocument49 pagesDr. Sailendra Nayak Assistant Professor MedicineAishwarya JeeNo ratings yet
- 209-Hematology Review - Case StudiesDocument129 pages209-Hematology Review - Case StudiesKhalid Khalidi100% (2)
- Self Esteem and The Real Body ImageDocument12 pagesSelf Esteem and The Real Body ImageChy Alcarde50% (2)
- Hematology OncologyDocument476 pagesHematology OncologySukumar SubramaniNo ratings yet
- Everything You Need to Know About Anemia: Causes, Symptoms, Diagnosis and TreatmentDocument60 pagesEverything You Need to Know About Anemia: Causes, Symptoms, Diagnosis and TreatmentPriyanka MhNo ratings yet
- Hematologic Pathology p36-47Document12 pagesHematologic Pathology p36-47zeroun24No ratings yet
- Anemia - AmbossDocument10 pagesAnemia - AmbossGuga XachidzeNo ratings yet
- Hematology Mudit Khanna PDFDocument40 pagesHematology Mudit Khanna PDFSylvia DiamondNo ratings yet
- Classification of Anemias: What Is Anemia, How Do You Diagnose Anemia, and How Are The Different Anemias Classified?Document78 pagesClassification of Anemias: What Is Anemia, How Do You Diagnose Anemia, and How Are The Different Anemias Classified?Kaushik BhuvaNo ratings yet
- Hematology Notes for Medical StudentsFrom EverandHematology Notes for Medical StudentsRating: 5 out of 5 stars5/5 (1)
- Dgca Module 06 Part 02Document15 pagesDgca Module 06 Part 02Deepak Choudhary DCNo ratings yet
- Bi Metallic Corrosion PDFDocument34 pagesBi Metallic Corrosion PDFDerek OngNo ratings yet
- Spectralis Touch Panel Upgrade GuideDocument10 pagesSpectralis Touch Panel Upgrade GuideMohamed AbdulaalNo ratings yet
- Haemolytic Anemia: DR Dumitha Govindapala MBBS, MD (Col), MRCP (London), FRCPDocument53 pagesHaemolytic Anemia: DR Dumitha Govindapala MBBS, MD (Col), MRCP (London), FRCPLilaksha Hasaranga100% (1)
- Erythrocyte DisordersDocument113 pagesErythrocyte Disordersbewildered-escapist-4301No ratings yet
- Manual de Reparacion TXV75Document16 pagesManual de Reparacion TXV75Ovh MaquinariasNo ratings yet
- Sds d201 Diatro - Lyse-Diff v4.1Document7 pagesSds d201 Diatro - Lyse-Diff v4.1Fauzia BudimanNo ratings yet
- Anemia 1Document104 pagesAnemia 1maryam ijazNo ratings yet
- DR Bambang - Anemia OverviewDocument263 pagesDR Bambang - Anemia OverviewOkta Dwi Kusuma AyuNo ratings yet
- By Pass System in The Dry ProcessDocument34 pagesBy Pass System in The Dry Processfaheemqc100% (1)
- Hospital Acquired Infections-IIDocument52 pagesHospital Acquired Infections-IIFATHIMA ANo ratings yet
- Anemia OsamaDocument57 pagesAnemia Osamaosamafoud7710No ratings yet
- Anemia OsamaDocument57 pagesAnemia Osamaosamafoud7710No ratings yet
- Red Cell Disorders: Excellent in Quality, Competitiveness, and CareDocument43 pagesRed Cell Disorders: Excellent in Quality, Competitiveness, and CareDeriven Teweng0% (1)
- Lecture 3rd. AnemiaDocument39 pagesLecture 3rd. Anemiaعمیرسعید قاضیNo ratings yet
- Dr. Mahmmoud Ayish Lecture on AnemiaDocument21 pagesDr. Mahmmoud Ayish Lecture on AnemiaRashed ShatnawiNo ratings yet
- Approach To Anemia and PolycythemiaDocument7 pagesApproach To Anemia and PolycythemiaambutlangnimoNo ratings yet
- Man with Fatigue and Abdominal Pain Diagnosed with Iron-Deficiency AnemiaDocument45 pagesMan with Fatigue and Abdominal Pain Diagnosed with Iron-Deficiency AnemiaMark GironNo ratings yet
- RBC DISORDERS StudentsDocument84 pagesRBC DISORDERS Studentskimberly abianNo ratings yet
- Understanding AnemiaDocument22 pagesUnderstanding Anemiasatvindar_muNo ratings yet
- Anaemi A: Joshi Abhishek Ashvinbhai F.Y.P.B.B.Sc - Nursing Govt - College of Nursing JamnagarDocument82 pagesAnaemi A: Joshi Abhishek Ashvinbhai F.Y.P.B.B.Sc - Nursing Govt - College of Nursing JamnagarReshu ThakuriNo ratings yet
- Anemia Type Pathogenesis Clinical Manifestations Diagnosis Peripheral Blood Lab FindingsDocument15 pagesAnemia Type Pathogenesis Clinical Manifestations Diagnosis Peripheral Blood Lab FindingsDanielle FosterNo ratings yet
- Anemia and Its Oral MenifestationsDocument74 pagesAnemia and Its Oral MenifestationsBushra FaheemNo ratings yet
- Kuliah AnemiaaDocument44 pagesKuliah AnemiaaAhmad Umar AfNo ratings yet
- Understanding Red Cell DisordersDocument43 pagesUnderstanding Red Cell DisordersYuliusDenisChrismaajiNo ratings yet
- Anaemia NNNNDocument82 pagesAnaemia NNNNAbdirahman Abdillahi Farah100% (1)
- Pharmacotherapy of Hematological Disorders by Hailu C. (Asst - Prof)Document132 pagesPharmacotherapy of Hematological Disorders by Hailu C. (Asst - Prof)Esubalew TeshomeNo ratings yet
- Introduction To HematologyDocument23 pagesIntroduction To HematologyReba PhiliposeNo ratings yet
- Anemia (: /Ə Ni Miə/ Also Spelled Greek Red Blood Cells HemoglobinDocument13 pagesAnemia (: /Ə Ni Miə/ Also Spelled Greek Red Blood Cells HemoglobinAryana BudiawanNo ratings yet
- 3304 37128 Anemia DefisiensiDocument36 pages3304 37128 Anemia DefisiensifatihahannisahumairaNo ratings yet
- Megaloblastic AneamiaDocument74 pagesMegaloblastic AneamiaPhysiology by Dr RaghuveerNo ratings yet
- Types of Anaemia and How To Remember Them: With Sophie BroughtonDocument28 pagesTypes of Anaemia and How To Remember Them: With Sophie BroughtonurtikikeNo ratings yet
- Understanding the Classification and Mechanisms of AnemiaDocument36 pagesUnderstanding the Classification and Mechanisms of AnemiafatihahannisahumairaNo ratings yet
- Red and White Blood Cell DisordersDocument11 pagesRed and White Blood Cell DisordersVittorio Di PaoloNo ratings yet
- Introduction To Clinical ExaminationDocument153 pagesIntroduction To Clinical ExaminationBnB UsmleNo ratings yet
- Interpretation of FBC Part 1Document15 pagesInterpretation of FBC Part 1reuel nareshNo ratings yet
- 21 Anaemia and PancytopeniaDocument42 pages21 Anaemia and PancytopeniaLeon Hui MingNo ratings yet
- HaematopathologyDocument253 pagesHaematopathologyamyNo ratings yet
- Anemia (Pronounced: o o o o o o oDocument12 pagesAnemia (Pronounced: o o o o o o opamela100181No ratings yet
- Hema II Chapter 3 - Anemiarev - ATDocument154 pagesHema II Chapter 3 - Anemiarev - AThannigadah7No ratings yet
- Evaluation of The Anemic PatientDocument44 pagesEvaluation of The Anemic PatientShobana KmNo ratings yet
- Approach To Anemia: Bisrat DDocument45 pagesApproach To Anemia: Bisrat Dyared getachewNo ratings yet
- MK Hematology-AnemiasDocument86 pagesMK Hematology-AnemiasMoses Jr KazevuNo ratings yet
- Chapter Two Anemiarev - ATDocument153 pagesChapter Two Anemiarev - ATAemro TadeleNo ratings yet
- Anemia: Prof. Dr. Rafita Ramayati, Spa (K) Prof. Dr..Rusdidjas, Spa (K) Dr. Oke Rina Ramayani, Spa BGN Ilmu Kes. Anak Fk-UsuDocument44 pagesAnemia: Prof. Dr. Rafita Ramayati, Spa (K) Prof. Dr..Rusdidjas, Spa (K) Dr. Oke Rina Ramayani, Spa BGN Ilmu Kes. Anak Fk-UsuleniNo ratings yet
- Everything You Need to Know About AnemiaDocument14 pagesEverything You Need to Know About AnemiaHermawan HmnNo ratings yet
- HIS 7 - Haemopoiesis and Blood ComponentsDocument3 pagesHIS 7 - Haemopoiesis and Blood ComponentsKristin DouglasNo ratings yet
- Anemia DIC NotesDocument6 pagesAnemia DIC NotesJeanna ChongNo ratings yet
- Clasification of Anemia: Prof. Dr. Adi Koesoema Aman SPPK (KH) Dr. Malayana Nasutioan Mked - SPPKDocument46 pagesClasification of Anemia: Prof. Dr. Adi Koesoema Aman SPPK (KH) Dr. Malayana Nasutioan Mked - SPPKrubyniNo ratings yet
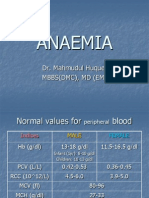
- Anaemia: Dr. Mahmudul Huque. Mbbs (DMC), MD (Em)Document32 pagesAnaemia: Dr. Mahmudul Huque. Mbbs (DMC), MD (Em)Junayed Safar MahmudNo ratings yet
- Systematic Plan For The Diagnosis of AnaemiaDocument31 pagesSystematic Plan For The Diagnosis of AnaemiaAriyike OmoobaNo ratings yet
- A Practical Approach to Diagnosing and Treating AnemiaDocument99 pagesA Practical Approach to Diagnosing and Treating AnemiaNipun AgrawalNo ratings yet
- AnaemiaDocument34 pagesAnaemiadakshpanchal26369No ratings yet
- Classification and Causes of Anemia ExplainedDocument30 pagesClassification and Causes of Anemia ExplainedhercolaniumNo ratings yet
- AnemiaDocument21 pagesAnemiaMarie WagasNo ratings yet
- Class 3: Anemia Outline I. Anemia OverviewDocument4 pagesClass 3: Anemia Outline I. Anemia OverviewTonyNo ratings yet
- Urine Eaxmintaion ReportDocument7 pagesUrine Eaxmintaion Reportapi-3745021No ratings yet
- A Review of Empathy Education in NursingDocument11 pagesA Review of Empathy Education in Nursinglora ardyaNo ratings yet
- F 856 - 97 - Rjg1ni05nw - PDFDocument7 pagesF 856 - 97 - Rjg1ni05nw - PDFRománBarciaVazquezNo ratings yet
- Comparative Population Growth and Losses Cause by Beetle Trogoderama Granarium (Everts) To Selected Past and Present Wheat GenotypesDocument12 pagesComparative Population Growth and Losses Cause by Beetle Trogoderama Granarium (Everts) To Selected Past and Present Wheat GenotypesInternational Network For Natural SciencesNo ratings yet
- Me, Myself, and My Dream CareerDocument12 pagesMe, Myself, and My Dream CareerJed CameronNo ratings yet
- Optimized Die Steel Reference GuideDocument16 pagesOptimized Die Steel Reference GuideKeattikhun ChaichanaNo ratings yet
- Tarbucks: Starbucks Corporation Is An International Coffee and Coffeehouse Chain BasedDocument12 pagesTarbucks: Starbucks Corporation Is An International Coffee and Coffeehouse Chain BasedVenu GopalNo ratings yet
- PPR - LISTS - Registered Medicine Price List - 20221127 BahrainDocument318 pagesPPR - LISTS - Registered Medicine Price List - 20221127 BahrainvdvedNo ratings yet
- History of Herbal TritmentDocument10 pagesHistory of Herbal TritmentTorentSpyNo ratings yet
- Klee PTLDocument3 pagesKlee PTLapi-590350469No ratings yet
- Michigan Western District Stay On State Supreme Court Response On Whitmer Emergency Powers 061920Document7 pagesMichigan Western District Stay On State Supreme Court Response On Whitmer Emergency Powers 061920Beverly TranNo ratings yet
- Airworthiness Directives Record ControlDocument4 pagesAirworthiness Directives Record ControlJuan builesNo ratings yet
- Alloy 5754 - Aimg3: Key FeaturesDocument1 pageAlloy 5754 - Aimg3: Key FeaturessatnamNo ratings yet
- Knime SeventechniquesdatadimreductionDocument266 pagesKnime SeventechniquesdatadimreductionramanadkNo ratings yet
- Health Facilities and Services Regulatory Bureau: Republic of The Philippines Department of HealthDocument3 pagesHealth Facilities and Services Regulatory Bureau: Republic of The Philippines Department of Healthal gulNo ratings yet
- PN15CS1S01Document4 pagesPN15CS1S01joadNo ratings yet
- 18 National Indicator Framework For Monitoring Evaluation Myanmar Ye Naing HtetDocument9 pages18 National Indicator Framework For Monitoring Evaluation Myanmar Ye Naing HtetKo KyawNo ratings yet
- Experiment # 04: Short-Circuit Test of Single Phase TransformerDocument5 pagesExperiment # 04: Short-Circuit Test of Single Phase TransformerNasir Ali / Lab Engineer, Electrical Engineering DepartmentNo ratings yet
- S35MC Engine Layout and Load DiagramsDocument17 pagesS35MC Engine Layout and Load DiagramsMuhammad AlfaniNo ratings yet
- District Potential Analysis of PilibhitDocument57 pagesDistrict Potential Analysis of PilibhitJasraj SinghNo ratings yet
- Museum functional areas guideDocument8 pagesMuseum functional areas guideChelle CruzNo ratings yet
- Serving TechniquesDocument4 pagesServing TechniquesSindy FadyaNo ratings yet