You might also like
- Hematology Mudit Khanna PDFDocument40 pagesHematology Mudit Khanna PDFSylvia DiamondNo ratings yet
- Hemolytic AnemiaDocument99 pagesHemolytic AnemiaSagar Chandrakant Mhetre100% (3)
- Understanding Anemia: Causes, Symptoms, Diagnosis and TreatmentDocument33 pagesUnderstanding Anemia: Causes, Symptoms, Diagnosis and TreatmentPurple basketNo ratings yet
- Lecture 3rd. AnemiaDocument39 pagesLecture 3rd. Anemiaعمیرسعید قاضیNo ratings yet
- Understanding Anemia: Causes, Symptoms, Diagnosis and TreatmentDocument60 pagesUnderstanding Anemia: Causes, Symptoms, Diagnosis and TreatmentSusi DesmaryaniNo ratings yet
- AnemiaDocument56 pagesAnemiaSivaNo ratings yet
- Shelly AnemiaDocument56 pagesShelly AnemiaSylda Rakmah Syarti IINo ratings yet
- Anemia: Iin Novita Nurhidayati Mahmuda FK Ums Rs Pku Muhammadiyah SurakartaDocument55 pagesAnemia: Iin Novita Nurhidayati Mahmuda FK Ums Rs Pku Muhammadiyah Surakartafenti nurul khafifahNo ratings yet
- Introduction To HematologyDocument23 pagesIntroduction To HematologyReba PhiliposeNo ratings yet
- 21 Anaemia and PancytopeniaDocument42 pages21 Anaemia and PancytopeniaLeon Hui MingNo ratings yet
- Update On (Approach To) AnemiaDocument44 pagesUpdate On (Approach To) AnemiaIsaac MwangiNo ratings yet
- Aplastic and Hypoplastic Anemias Including Mylodysplastic SyndromeDocument47 pagesAplastic and Hypoplastic Anemias Including Mylodysplastic SyndromeRahul Kumar VermaNo ratings yet
- SBRC HematologyOncology 1Document80 pagesSBRC HematologyOncology 1dalia khamoNo ratings yet
- Anaemia Types, Causes, Symptoms and TreatmentDocument33 pagesAnaemia Types, Causes, Symptoms and TreatmentGopi NathNo ratings yet
- Decreased Hemoglobin Available For Erythrocytes Microcytic, Hypochromic Anemia More Hemoglobin Available For Erythrocytes Macrocytic AnemiaDocument2 pagesDecreased Hemoglobin Available For Erythrocytes Microcytic, Hypochromic Anemia More Hemoglobin Available For Erythrocytes Macrocytic AnemiaIB leaksNo ratings yet
- PejowebApproach To Anemia by Dr. Joel Solorzani RomeroDocument57 pagesPejowebApproach To Anemia by Dr. Joel Solorzani RomeroAshraf FaragNo ratings yet
- Anemia Type Pathogenesis Clinical Manifestations Diagnosis Peripheral Blood Lab FindingsDocument15 pagesAnemia Type Pathogenesis Clinical Manifestations Diagnosis Peripheral Blood Lab FindingsDanielle FosterNo ratings yet
- Red Cell Disorders: Excellent in Quality, Competitiveness, and CareDocument43 pagesRed Cell Disorders: Excellent in Quality, Competitiveness, and CareDeriven Teweng0% (1)
- Penyakit HematologiDocument128 pagesPenyakit HematologiLintang SuroyaNo ratings yet
- Anemia OsamaDocument57 pagesAnemia Osamaosamafoud7710No ratings yet
- Tutori - Anemia MhsDocument38 pagesTutori - Anemia Mhszaky ariandyNo ratings yet
- Red Blood Cells PathologyDocument47 pagesRed Blood Cells PathologyRodriguez Vivanco Kevin DanielNo ratings yet
- Anemia OsamaDocument57 pagesAnemia Osamaosamafoud7710No ratings yet
- DR Vishu P Bhasin DCP Resident, Santosh Medical CollegeDocument30 pagesDR Vishu P Bhasin DCP Resident, Santosh Medical CollegeDabogski FranceNo ratings yet
- DR Vishu P Bhasin DCP Resident, Santosh Medical CollegeDocument30 pagesDR Vishu P Bhasin DCP Resident, Santosh Medical CollegeDabogski FranceNo ratings yet
- Anemia Gravis: Understanding Severe Anemia with Hb ≤ 7 g/dLDocument35 pagesAnemia Gravis: Understanding Severe Anemia with Hb ≤ 7 g/dLMufthifina AulahaqNo ratings yet
- DR Bambang - Anemia OverviewDocument263 pagesDR Bambang - Anemia OverviewOkta Dwi Kusuma AyuNo ratings yet
- อ - ชลลดา - Approach to AnemiaDocument44 pagesอ - ชลลดา - Approach to AnemiaSOPHIASTIA KUSBIANTI MHS 2017No ratings yet
- Anemia in SurgeryDocument29 pagesAnemia in SurgeryEdwin OkonNo ratings yet
- RBC Disorder Guide: Causes, Symptoms and TreatmentDocument56 pagesRBC Disorder Guide: Causes, Symptoms and TreatmentMunawar Adhar100% (4)
- Peripheral Smear Examination PDFDocument91 pagesPeripheral Smear Examination PDFtufis02No ratings yet
- Aplastic Hemolitic 2021 OlgaDocument43 pagesAplastic Hemolitic 2021 OlgalaibaNo ratings yet
- Anemia Types, Causes, Symptoms & Nursing CareDocument6 pagesAnemia Types, Causes, Symptoms & Nursing CareJennNo ratings yet
- Anemia: DR - Nadjwa Zamalek Dalimoenthe, SPPKDocument35 pagesAnemia: DR - Nadjwa Zamalek Dalimoenthe, SPPKNasyaDwiAriestantiNo ratings yet
- Clasification of Anemia: Prof. Dr. Adi Koesoema Aman SPPK (KH) Dr. Malayana Nasutioan Mked - SPPKDocument46 pagesClasification of Anemia: Prof. Dr. Adi Koesoema Aman SPPK (KH) Dr. Malayana Nasutioan Mked - SPPKrubyniNo ratings yet
- Evaluation of The Anemic PatientDocument44 pagesEvaluation of The Anemic PatientShobana KmNo ratings yet
- Clinical Approach To Anemia: Fakultas Kedokteran Universitas Prima IndonesiaDocument24 pagesClinical Approach To Anemia: Fakultas Kedokteran Universitas Prima IndonesiaDzil FikriNo ratings yet
- Approach To AnemiaDocument33 pagesApproach To AnemiaVaibhav KrishnaNo ratings yet
- Red and White Blood Cell DisordersDocument11 pagesRed and White Blood Cell DisordersVittorio Di PaoloNo ratings yet
- Basic Lab InvestigationsDocument121 pagesBasic Lab InvestigationsTheop Ayodele100% (1)
- Pediatric Hematology & Oncology: Muhammad RizaDocument17 pagesPediatric Hematology & Oncology: Muhammad RizareavondNo ratings yet
- AnemiaDocument51 pagesAnemiaAravind A SNo ratings yet
- COMPLETE BLOOD PICTURE Ok-1 PDFDocument78 pagesCOMPLETE BLOOD PICTURE Ok-1 PDFEmanuel100% (1)
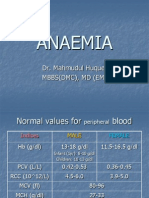
- Anaemia: Dr. Mahmudul Huque. Mbbs (DMC), MD (Em)Document32 pagesAnaemia: Dr. Mahmudul Huque. Mbbs (DMC), MD (Em)Junayed Safar MahmudNo ratings yet
- Anemia: Diagnostic ApproachDocument36 pagesAnemia: Diagnostic ApproachRizky LumalessilNo ratings yet
- Anemia SDocument42 pagesAnemia SCristinaGheorgheNo ratings yet
- Haemolytic Anemia by DR Gireesh Kumar K P, Department of Emergency Medicine, Amrita Institute of Medical Sciences, Kochi, KeralaDocument14 pagesHaemolytic Anemia by DR Gireesh Kumar K P, Department of Emergency Medicine, Amrita Institute of Medical Sciences, Kochi, KeralaAETCM Emergency medicineNo ratings yet
- Topic 2. CBC Part 1 2021-02-26 at 11.03.32 PMDocument113 pagesTopic 2. CBC Part 1 2021-02-26 at 11.03.32 PMSub 7 Grp 3No ratings yet
- Ha I by AbdifatahDocument109 pagesHa I by AbdifatahAbdifatah AhmedNo ratings yet
- C B C I: Omplete Lood Ount NterpretationsDocument44 pagesC B C I: Omplete Lood Ount NterpretationsridhoniNo ratings yet
- Hemolytic AnemiaDocument9 pagesHemolytic AnemiaTheeya QuigaoNo ratings yet
- Hematology 1Document61 pagesHematology 1katz_hotchickNo ratings yet
- S0850alug 1670953860959-SEU HDocument56 pagesS0850alug 1670953860959-SEU HAziz KhwajaNo ratings yet
- Types of Anaemia and How To Remember Them: With Sophie BroughtonDocument28 pagesTypes of Anaemia and How To Remember Them: With Sophie BroughtonurtikikeNo ratings yet
- Ana IfDocument101 pagesAna Ifshrikrishnapathlab100% (1)
- AnaemiaDocument7 pagesAnaemiaYousef El3alameyNo ratings yet
- HemolysisDocument22 pagesHemolysisMohamoud MohamedNo ratings yet
- Diet and thyroid myths and facts review articleDocument6 pagesDiet and thyroid myths and facts review articleAhmad Umar AfNo ratings yet
- POV Ingg PDFDocument9 pagesPOV Ingg PDFTheresa JulietNo ratings yet
- ISTC 3rdedDocument92 pagesISTC 3rdedmichaelqurtisNo ratings yet
- LBM 5 RespiDocument2 pagesLBM 5 RespiAhmad Umar AfNo ratings yet
- Journal BasingDocument13 pagesJournal BasingAhmad Umar AfNo ratings yet
- Jurnal 1Document8 pagesJurnal 1dita irvanaNo ratings yet
- Journal BasingDocument13 pagesJournal BasingAhmad Umar AfNo ratings yet
- Kuliah Tamu NAFLD Unissula 2016Document97 pagesKuliah Tamu NAFLD Unissula 2016wkwkwkhhhhNo ratings yet
- Journal BasingDocument13 pagesJournal BasingAhmad Umar AfNo ratings yet
- LBM 5 RespiDocument2 pagesLBM 5 RespiAhmad Umar AfNo ratings yet
- 442 1419 1 SM PDFDocument4 pages442 1419 1 SM PDFAhmad Umar AfNo ratings yet
- LBM 5 RespiDocument2 pagesLBM 5 RespiAhmad Umar AfNo ratings yet
- An Incidence of β-Thalassemia in South India - A Review: Suresh Babu TV, Manjula ShantaramDocument7 pagesAn Incidence of β-Thalassemia in South India - A Review: Suresh Babu TV, Manjula ShantaramAmy LalringhluaniNo ratings yet
- Olahan Data Spps AmandaDocument47 pagesOlahan Data Spps AmandaRiyan NurdiansyahNo ratings yet
- Iron Deficiency AnemiaDocument12 pagesIron Deficiency AnemiaAnkush GahlotNo ratings yet
- Fujino 2013Document4 pagesFujino 2013Carolina RiveraNo ratings yet
- Differential Diagnosis of Microcytic Anemia PDFDocument5 pagesDifferential Diagnosis of Microcytic Anemia PDFayms99No ratings yet
- Pendekatan Diagnosis AnemiaDocument7 pagesPendekatan Diagnosis AnemiaFerry GhifariNo ratings yet
- D10 Interpretation Training 2020 - CDocument36 pagesD10 Interpretation Training 2020 - CJose SirittNo ratings yet
- RED CELL MORPHOLOGY Tabulation SummaryDocument6 pagesRED CELL MORPHOLOGY Tabulation SummaryStephen YorNo ratings yet
- Poikilocytosis Review TableDocument5 pagesPoikilocytosis Review Tablekat100% (1)
- Penyuluhan Nutrisi Pada Ibu Hamil Untuk Mencegah Dan Menanggulangi Anemia Gizi Besi Melalui Komunikasi InterpersonalDocument11 pagesPenyuluhan Nutrisi Pada Ibu Hamil Untuk Mencegah Dan Menanggulangi Anemia Gizi Besi Melalui Komunikasi Interpersonalnurhaliza rakhamanNo ratings yet
- 7.2. Hemolytic AnemiaDocument29 pages7.2. Hemolytic AnemiaMichellyTjoaNo ratings yet
- ThalassemiaDocument44 pagesThalassemiaitsshaswatNo ratings yet
- Approach To Hemolytic AnemiaDocument63 pagesApproach To Hemolytic AnemiaSarath Menon R100% (2)
- Beta ThalassemiaDocument2 pagesBeta ThalassemiaNadia Zalfa RafillaNo ratings yet
- Hemoglobin Electrophoresis EditedDocument48 pagesHemoglobin Electrophoresis EditedBean TeNo ratings yet
- RBC IndicesDocument13 pagesRBC IndicespremNo ratings yet
- AnemiaDocument15 pagesAnemiaBeeBeeSethNo ratings yet
- Alpha ThalassemiaDocument4 pagesAlpha ThalassemiaNorman DamaaNo ratings yet
- Harr 5th EdDocument15 pagesHarr 5th EdTrixia UrsuaNo ratings yet
- Evaluasi Program Pemberian Tablet Tambah Darah Pada Remaja Putri Anemia Dan Non Anemia Di Wilayah Puskesmas AntapaniDocument9 pagesEvaluasi Program Pemberian Tablet Tambah Darah Pada Remaja Putri Anemia Dan Non Anemia Di Wilayah Puskesmas AntapaniAgung JayaNo ratings yet
- Tosoh HPLC G11 InstrumentDocument25 pagesTosoh HPLC G11 InstrumentHw XuNo ratings yet
- RBC Morph Ulka 2Document69 pagesRBC Morph Ulka 2Rushi WalgudeNo ratings yet
- Pengaruh Konsumsi Buah Naga (Hylocereus) Terhadap Kadar Hemoglobin Pada Siswi Dengan Anemia Di Sman 5 Kota Kediritahun 2019Document13 pagesPengaruh Konsumsi Buah Naga (Hylocereus) Terhadap Kadar Hemoglobin Pada Siswi Dengan Anemia Di Sman 5 Kota Kediritahun 2019Niken AyNo ratings yet
- Parameter Nilai RujukanDocument1 pageParameter Nilai RujukanRuben SipiNo ratings yet
- Hemolytic Anemia SDocument1 pageHemolytic Anemia Sdnutter012576No ratings yet
- Pappenheimer BodiesDocument12 pagesPappenheimer BodiesDennis ValdezNo ratings yet
- RBCs Abnormal Morphology FinalDocument33 pagesRBCs Abnormal Morphology FinalInahkoni Alpheus Sky OiragasNo ratings yet
- Tariq PresentationDocument24 pagesTariq PresentationHasnain AliNo ratings yet
- HEMA 1A 2nd Shift Reviewer RBC Morphology & InclusionsDocument9 pagesHEMA 1A 2nd Shift Reviewer RBC Morphology & InclusionsbiancsNo ratings yet