You might also like
- TST EngDocument44 pagesTST Engubaidullah78611No ratings yet
- QuantiFERON TB Gold in Tube Test For Diagnosis ofDocument19 pagesQuantiFERON TB Gold in Tube Test For Diagnosis ofConstantin PopescuNo ratings yet
- A Meta-Analysis of Lamivudine For Interruption of Mother-To-Child Transmission of Hepatitis B VirusDocument41 pagesA Meta-Analysis of Lamivudine For Interruption of Mother-To-Child Transmission of Hepatitis B VirusErlin NurhariansyahNo ratings yet
- Keertan Dheda (3) TB Test PDFDocument48 pagesKeertan Dheda (3) TB Test PDFphuong mai leNo ratings yet
- Retos en El Manejo de La Comorbilidad TB-DM: César Ugarte-Gil, MD MSC Cesar - Ugarte@Upch - PeDocument46 pagesRetos en El Manejo de La Comorbilidad TB-DM: César Ugarte-Gil, MD MSC Cesar - Ugarte@Upch - PePatricia CorralesNo ratings yet
- Shorter Treatment Duration For Selected Patients With Multidrug-Resistant TuberculosisDocument4 pagesShorter Treatment Duration For Selected Patients With Multidrug-Resistant Tuberculosispooja thanekarNo ratings yet
- Taxotere Docetaxel 80 mg/4 ML Concentrate For Solution For InfusionDocument52 pagesTaxotere Docetaxel 80 mg/4 ML Concentrate For Solution For InfusionArbiati Rahman100% (1)
- CTCA2 - IGRA in Young ChildrenDocument28 pagesCTCA2 - IGRA in Young ChildrenAnonymous HofOUrbNo ratings yet
- Human Genetic Variant E756del in The Ion Channel PDocument3 pagesHuman Genetic Variant E756del in The Ion Channel PDominic AmuzuNo ratings yet
- 2 TishleDocument38 pages2 TishleIRANo ratings yet
- Toxoplasma Gondii Infection in PregnantDocument5 pagesToxoplasma Gondii Infection in Pregnantdiaa skamNo ratings yet
- Paper Comparativa Sobrevida de PV, TE y MFP ComplementoDocument4 pagesPaper Comparativa Sobrevida de PV, TE y MFP ComplementoDani HaindlNo ratings yet
- WHO - Tuberculosis Philippines (2014)Document1 pageWHO - Tuberculosis Philippines (2014)golokipokNo ratings yet
- Diagnostic TestingDocument55 pagesDiagnostic TestingMoldovan Nicolae-AndreiNo ratings yet
- Increased Serum Hyaluronic Acid and Heparan Sulfate in Dengue Fever: Association With Plasma Leakage and Disease SeverityDocument9 pagesIncreased Serum Hyaluronic Acid and Heparan Sulfate in Dengue Fever: Association With Plasma Leakage and Disease SeverityLaura Zuñiga TorresNo ratings yet
- Research Journal4Document5 pagesResearch Journal4Jayhan AmbrocioNo ratings yet
- Kol Slide Kit Atac 100Document43 pagesKol Slide Kit Atac 100api-26302710No ratings yet
- CCO 2020 WCLC Downloadable 1Document106 pagesCCO 2020 WCLC Downloadable 1Florencia GuerraNo ratings yet
- Manuscrip Rajia (Traslet)Document6 pagesManuscrip Rajia (Traslet)muliyanaNo ratings yet
- 2013-02-12 Impact of First Line ART Resistance in Resource Limited Settings-Implications For Future Treatment OptionsDocument54 pages2013-02-12 Impact of First Line ART Resistance in Resource Limited Settings-Implications For Future Treatment OptionsTarun KannanNo ratings yet
- Trombólisis Tromboembolia Pulmonar Dosis Media Total 2022 CartaDocument4 pagesTrombólisis Tromboembolia Pulmonar Dosis Media Total 2022 CartaOscar BushNo ratings yet
- 54205-Article Text-94353-1-10-20100629Document7 pages54205-Article Text-94353-1-10-20100629JamesNo ratings yet
- Admin,+journal+manager,+53 AJPCR 18789 RADocument3 pagesAdmin,+journal+manager,+53 AJPCR 18789 RAgangeshwarmishraNo ratings yet
- Abstract Pregnancy Outcomes of In-Vitro Fertilization On Infertile Women With Adenomyosis-Retrospective Cohort StudyDocument6 pagesAbstract Pregnancy Outcomes of In-Vitro Fertilization On Infertile Women With Adenomyosis-Retrospective Cohort StudyLouis ReganNo ratings yet
- Supplementary Table 1. ICD-10 Diagnostic Codes of Autoimmune DiseasesDocument4 pagesSupplementary Table 1. ICD-10 Diagnostic Codes of Autoimmune DiseasesKustiani OnieNo ratings yet
- Correa ModelDocument21 pagesCorrea ModelPaulo Cesar Castañeda RuizNo ratings yet
- AJGH - Volume 6 - Issue 1 - Pages 1-18Document18 pagesAJGH - Volume 6 - Issue 1 - Pages 1-18Ivania MarquezNo ratings yet
- The Epidemiology and Diagnosis of Childhood Tuberculosis: Ma. Cecilia G. Ama, MD National TB Reference Laboratory, RITMDocument62 pagesThe Epidemiology and Diagnosis of Childhood Tuberculosis: Ma. Cecilia G. Ama, MD National TB Reference Laboratory, RITMriz04_fortitudessa5178100% (1)
- Shen 2018Document12 pagesShen 2018Muhammad Yusuf HanifNo ratings yet
- Yield of Thoracoscopic Biopsy Truenat in The Diagnosis of Tubercular Pleural EffusionDocument7 pagesYield of Thoracoscopic Biopsy Truenat in The Diagnosis of Tubercular Pleural EffusionThomas KurianNo ratings yet
- Ias 2011 PresentationDocument14 pagesIas 2011 PresentationSiva RamanNo ratings yet
- Sudan Tuberculosis ProfileDocument1 pageSudan Tuberculosis Profilemoilo8602No ratings yet
- Effectiveness of COVID-19 vaccines against hospital admission with the Delta variantDocument3 pagesEffectiveness of COVID-19 vaccines against hospital admission with the Delta variantFiona ValenciaNo ratings yet
- Supplementary Table 1 Life Expectancy Eliminating Death From Gastric Cancer in Late Elderly PatientsDocument3 pagesSupplementary Table 1 Life Expectancy Eliminating Death From Gastric Cancer in Late Elderly PatientsLady Marcela Cuenca BeltránNo ratings yet
- Final Article Rcog 31 Mei Jam 4 PagiDocument11 pagesFinal Article Rcog 31 Mei Jam 4 Pagikusumavk semarangNo ratings yet
- Safety of Topical Corticosteroids in Pregnancy: A Population-Based Cohort StudyDocument8 pagesSafety of Topical Corticosteroids in Pregnancy: A Population-Based Cohort Studyilma fitrianaNo ratings yet
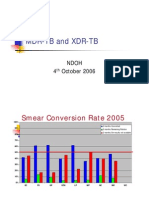
- MDR-TB and XDR-TB: Ndoh 4 October 2006Document40 pagesMDR-TB and XDR-TB: Ndoh 4 October 2006Eta Calvin ObenNo ratings yet
- Effect of Iron Supplementation On Infectious Morbidity and Mortality in ChildrenDocument52 pagesEffect of Iron Supplementation On Infectious Morbidity and Mortality in ChildrendropsyNo ratings yet
- BCG y TPI previenen TB SES, Lecca y otros Blue Journal 2014 supplementDocument10 pagesBCG y TPI previenen TB SES, Lecca y otros Blue Journal 2014 supplementVigilancia EpidemiologicaNo ratings yet
- Hassan Mohamed MudeyDocument10 pagesHassan Mohamed MudeymudeyNo ratings yet
- Yu2017 2Document11 pagesYu2017 2Mikael Reynardi SutantoNo ratings yet
- Us Ulan Proposal 3Document9 pagesUs Ulan Proposal 3Civic TypeRNo ratings yet
- Mother-child TB transmission: What we knowDocument50 pagesMother-child TB transmission: What we knowGiovanna Quiroz GuerraNo ratings yet
- Essay Komstat Farhan HF RahmanDocument5 pagesEssay Komstat Farhan HF RahmantaufikramadhaniNo ratings yet
- Factors Which Affect Mortality in Neonatal Sepsis: Original ArticleDocument6 pagesFactors Which Affect Mortality in Neonatal Sepsis: Original ArticleNabila NatasyaNo ratings yet
- AmendmentsDocument11 pagesAmendmentsLubna ZoubiNo ratings yet
- Genetic Association Between IL-21 Polymorphisms and Cryptorchidism in A Chinese Han PopulationDocument4 pagesGenetic Association Between IL-21 Polymorphisms and Cryptorchidism in A Chinese Han PopulationHugo AlvesNo ratings yet
- Gupta Et Al 2020 Evaluation of Quantiferon TB Gold Plus For Predicting Incident Tuberculosis Among Recent Contacts ADocument5 pagesGupta Et Al 2020 Evaluation of Quantiferon TB Gold Plus For Predicting Incident Tuberculosis Among Recent Contacts Awebsite-yokel-0eNo ratings yet
- EBM Therapy and Diagnosis-Interpretation of Results ExerciseDocument3 pagesEBM Therapy and Diagnosis-Interpretation of Results Exerciseomegasauron0gmailcomNo ratings yet
- FLAD1 Is Up-Regulated in Gastric Cancer and Is A Potential Prediction of PrognosisDocument10 pagesFLAD1 Is Up-Regulated in Gastric Cancer and Is A Potential Prediction of PrognosisAriani ArinNo ratings yet
- Taxenes in Breast Cancer (Sharm)Document76 pagesTaxenes in Breast Cancer (Sharm)safasayedNo ratings yet
- Vol. 223, No. 4S2, October 2016 Scientific Poster Presentations: 2016 Clinical Congress E113Document1 pageVol. 223, No. 4S2, October 2016 Scientific Poster Presentations: 2016 Clinical Congress E113asfwegereNo ratings yet
- 1 s2.0 S0006497121006340 MainDocument13 pages1 s2.0 S0006497121006340 Mainresi silviaNo ratings yet
- Soluble Trem-1 Levels in Familial Mediterranean Fever Related Aa-AmyloidosisDocument15 pagesSoluble Trem-1 Levels in Familial Mediterranean Fever Related Aa-AmyloidosisBuğra EgeliNo ratings yet
- Dengue Fever During Pregnancy: Original PaperDocument7 pagesDengue Fever During Pregnancy: Original Papermuhammad alfarisi sutrisnoNo ratings yet
- s41598-020-70514-zDocument13 pagess41598-020-70514-zlogan fioriNo ratings yet
- Human Genetics ResultsDocument6 pagesHuman Genetics ResultsHumma NayyarNo ratings yet
- HP Risc de Polip AdenomatosiDocument5 pagesHP Risc de Polip AdenomatosiOctavian DumitruNo ratings yet
- 576 Friday, 15 June 2018 Scientific AbstractsDocument2 pages576 Friday, 15 June 2018 Scientific AbstractsDanna Carvajal GaitanNo ratings yet
- Internet Based Interventions For Smoking CessationDocument132 pagesInternet Based Interventions For Smoking CessationConstantin PopescuNo ratings yet
- 21st-Century Hazards of Smoking and Benefits of Cessation in The United StatesDocument10 pages21st-Century Hazards of Smoking and Benefits of Cessation in The United StatesConstantin PopescuNo ratings yet
- Probability and Predictors of Relapse To Smoking Results of The National Epidemiologic Survey On Alcohol and Related Conditions (NESARC)Document23 pagesProbability and Predictors of Relapse To Smoking Results of The National Epidemiologic Survey On Alcohol and Related Conditions (NESARC)Constantin PopescuNo ratings yet
- Supporting Smoking Cessation PDFDocument83 pagesSupporting Smoking Cessation PDFOagnuj RrabNo ratings yet
- Optimizing Smoking Cessation Counseling in A University HospitalpdfDocument8 pagesOptimizing Smoking Cessation Counseling in A University HospitalpdfConstantin PopescuNo ratings yet
- Brief Opportunistic Interventions by General Practitioners To Promote Smoking Cessation A Conversation Analytic StudyDocument14 pagesBrief Opportunistic Interventions by General Practitioners To Promote Smoking Cessation A Conversation Analytic StudyConstantin PopescuNo ratings yet
- Exercise Interventions For Smoking CessationDocument66 pagesExercise Interventions For Smoking CessationConstantin PopescuNo ratings yet
- CD013183Document190 pagesCD013183Constantin PopescuNo ratings yet
- Mindfulness For Smoking CessationDocument99 pagesMindfulness For Smoking CessationConstantin PopescuNo ratings yet
- Table 1. Patient Characteristics and IGRA ResultsDocument1 pageTable 1. Patient Characteristics and IGRA ResultsConstantin PopescuNo ratings yet
- Modelling Continuous Abstinence Rates Over Time FromDocument11 pagesModelling Continuous Abstinence Rates Over Time FromConstantin PopescuNo ratings yet
- National Trends in Cessation Counseling, Prescription Medication UseDocument13 pagesNational Trends in Cessation Counseling, Prescription Medication UseConstantin PopescuNo ratings yet
- The Effect of e Cigarette Vapour On The Lungs of ADocument18 pagesThe Effect of e Cigarette Vapour On The Lungs of AConstantin PopescuNo ratings yet
- Seeing New Opportunities To Help Smokers Quit A Uk National Surv 2018Document8 pagesSeeing New Opportunities To Help Smokers Quit A Uk National Surv 2018Constantin PopescuNo ratings yet
- COVID-19 PneumoniaDocument15 pagesCOVID-19 PneumoniaConstantin PopescuNo ratings yet
- Martinez Garcia2017Document11 pagesMartinez Garcia2017Constantin PopescuNo ratings yet
- Application of Health Behavioral Models in Smoking CessationDocument8 pagesApplication of Health Behavioral Models in Smoking CessationConstantin PopescuNo ratings yet
- SCREENING FOR TUBERCULOSIS IN MS PATIENTSDocument1 pageSCREENING FOR TUBERCULOSIS IN MS PATIENTSConstantin PopescuNo ratings yet
- Risks of Ecig and Vape Use Powerpoint FactsheetDocument1 pageRisks of Ecig and Vape Use Powerpoint FactsheetConstantin PopescuNo ratings yet
- Subclinical ILD Is Frequent and Progresses AcrossDocument14 pagesSubclinical ILD Is Frequent and Progresses AcrossConstantin PopescuNo ratings yet
- Latent Tuberculosis Infection in Patients With Multiple SclerosisDocument8 pagesLatent Tuberculosis Infection in Patients With Multiple SclerosisConstantin PopescuNo ratings yet
- Mesotelioma ESMODocument9 pagesMesotelioma ESMOKarla PooleyNo ratings yet
- 14c - ESTRO 2018 - de Ruysscher - Mesothelioma-1Document9 pages14c - ESTRO 2018 - de Ruysscher - Mesothelioma-1Constantin PopescuNo ratings yet
- Stop Smoking Practitioner TrainingDocument51 pagesStop Smoking Practitioner TrainingConstantin PopescuNo ratings yet
- What Is The Latest Research On The Influence of CiDocument19 pagesWhat Is The Latest Research On The Influence of CiConstantin PopescuNo ratings yet
- Revista NR 4 - 2020 Cu Publicitate 1Document102 pagesRevista NR 4 - 2020 Cu Publicitate 1Constantin PopescuNo ratings yet
- Treating Mesothelioma in 2021 What Is The Role ofDocument24 pagesTreating Mesothelioma in 2021 What Is The Role ofConstantin PopescuNo ratings yet
- Epidemiologia Cancer Pulmonar Si MezoteliomDocument43 pagesEpidemiologia Cancer Pulmonar Si MezoteliomConstantin PopescuNo ratings yet
- Guided Noteboo Kin GED10 2 (Mathe Matics in The Modern World)Document5 pagesGuided Noteboo Kin GED10 2 (Mathe Matics in The Modern World)Aaronie DeguNo ratings yet
- Effecta WoodyDocument21 pagesEffecta WoodyMR XNo ratings yet
- Trade BW Logistic ExtractionDocument54 pagesTrade BW Logistic Extractionlittlebros100% (1)
- Shri Mata Vaishno Devi Shrine Board - Welcome To Online ServicesjjDocument2 pagesShri Mata Vaishno Devi Shrine Board - Welcome To Online Servicesjjeternal diagnosticsNo ratings yet
- Activity 2EE56L FINALDocument6 pagesActivity 2EE56L FINALLUAÑA ALMARTNo ratings yet
- Ec6303 Signals and SystemsDocument2 pagesEc6303 Signals and SystemsSam PaulNo ratings yet
- Jurnal SinusitisDocument49 pagesJurnal SinusitisAramanda Dian100% (1)
- Sources of Subject of ArtDocument32 pagesSources of Subject of ArtAlaina De GuzmanNo ratings yet
- Ideas For Income Generating Projects PDFDocument29 pagesIdeas For Income Generating Projects PDFheart AquinoNo ratings yet
- Mana Paribhsha RSBKDocument31 pagesMana Paribhsha RSBKlohiyakankshaNo ratings yet
- An Investigation Into The Effects of Unsteady Parameters On The Aerodynamics of A Low Reynolds Number Pitching AirfoilDocument15 pagesAn Investigation Into The Effects of Unsteady Parameters On The Aerodynamics of A Low Reynolds Number Pitching AirfoilMANNE SAHITHINo ratings yet
- HypertensionDocument26 pagesHypertensionAbdalrhman Zaqqa100% (1)
- CHAPTER 8 The Rise of Instrumental Music - 141-152Document8 pagesCHAPTER 8 The Rise of Instrumental Music - 141-152Aleksandre Roderick-LorenzNo ratings yet
- SO 1550 F3 User ManualDocument18 pagesSO 1550 F3 User ManualLidya SukendroNo ratings yet
- Asia Pacific Chemicals 181302Document52 pagesAsia Pacific Chemicals 181302sealaishaniNo ratings yet
- ZEOLITEDocument13 pagesZEOLITEShubham Yele100% (1)
- Dynamic Bearing Capacity of Shallow FoundationDocument31 pagesDynamic Bearing Capacity of Shallow FoundationLingeswarran NumbikannuNo ratings yet
- 5fc56cb37a6847288b78b547 - Using Kobo ToolboxDocument4 pages5fc56cb37a6847288b78b547 - Using Kobo Toolboxpouya rahmanyNo ratings yet
- Why Am I Getting Temperature Divergence in AMG SolverDocument7 pagesWhy Am I Getting Temperature Divergence in AMG SolverSulaimanNo ratings yet
- E - Efma Rbi Insp Interval Assess Projector - PP SimtechDocument10 pagesE - Efma Rbi Insp Interval Assess Projector - PP SimtechAbhimanyu SharmaNo ratings yet
- CPO Science Foundations of Physics: Unit 7, Chapter 24Document47 pagesCPO Science Foundations of Physics: Unit 7, Chapter 24dheerajbhagwatNo ratings yet
- School Canteen Satisfaction Survey ResultsDocument2 pagesSchool Canteen Satisfaction Survey ResultsElla PastorinNo ratings yet
- Lippo Karawaci Review 30 September 2019 FINAL PDFDocument149 pagesLippo Karawaci Review 30 September 2019 FINAL PDFAndy AghastaNo ratings yet
- Tracing Chronic Fatigue Syndrome Tsfunction Is Key To ME - CFS - B Day PDFDocument91 pagesTracing Chronic Fatigue Syndrome Tsfunction Is Key To ME - CFS - B Day PDFsanthigiNo ratings yet
- Contractor base list in UsaDocument8 pagesContractor base list in Usamytech206No ratings yet
- - Bài nghe gồm 20 câu chia làm 3 phần - Thí sinh được nghe 2 lần, đĩa CD tự chạy 2 lầnDocument11 pages- Bài nghe gồm 20 câu chia làm 3 phần - Thí sinh được nghe 2 lần, đĩa CD tự chạy 2 lầnHồng NhungNo ratings yet
- Lab Manual Ds&BdalDocument100 pagesLab Manual Ds&BdalSEA110 Kshitij BhosaleNo ratings yet
- Fire and Ice by Robert FrostDocument2 pagesFire and Ice by Robert Frostapi-561976496No ratings yet
- Role of Marketing Research - Management Decision MakingDocument35 pagesRole of Marketing Research - Management Decision MakingDr Rushen Singh100% (1)
- 2tak Vs 4takDocument3 pages2tak Vs 4takTaufiq AlhakimNo ratings yet