You might also like
- Hematopoiesis Reading NotesDocument7 pagesHematopoiesis Reading NotesMemeowwNo ratings yet
- DSM-5 Changes to Psychotic and Mood Disorder CriteriaDocument9 pagesDSM-5 Changes to Psychotic and Mood Disorder CriteriaMonika LangngagNo ratings yet
- Our Eye As A Camera Refraction, Errors and Solutions.: DR - Ali.A.Taqi Fifth Year StudentsDocument44 pagesOur Eye As A Camera Refraction, Errors and Solutions.: DR - Ali.A.Taqi Fifth Year Studentsabigail100% (1)
- Error of RefractionDocument37 pagesError of RefractionIka KrastanayaNo ratings yet
- 12 - Objective RefractionDocument11 pages12 - Objective RefractionSumon SarkarNo ratings yet
- 2004 2005 Magnetom Flash 2 2Document64 pages2004 2005 Magnetom Flash 2 2Herick SavioneNo ratings yet
- Clinical RefractionDocument46 pagesClinical RefractionMuhammed Abdulmajeed100% (1)
- Activated Charcoal UseDocument6 pagesActivated Charcoal UseRodney LangleyNo ratings yet
- Maurice Nicoll The Mark PDFDocument4 pagesMaurice Nicoll The Mark PDFErwin KroonNo ratings yet
- 03 Refractive SurgeryDocument99 pages03 Refractive SurgeryWaqar Ahmad Khan100% (3)
- Chemtrails EffectsDocument1 pageChemtrails EffectsGary CloseNo ratings yet
- Refractive Mgmt/Intervention: Question 1 of 90Document39 pagesRefractive Mgmt/Intervention: Question 1 of 90NoorNo ratings yet
- Ortho ExamDocument9 pagesOrtho ExamPrince Rener Velasco Pera100% (2)
- Mapping Out Corneal TopographyDocument4 pagesMapping Out Corneal Topographyriggi lunaNo ratings yet
- Oculopathy: Disproves the orthodox and theoretical bases upon which glasses are so freely prescribed, and puts forward natural remedial methods of treatment for what are sometimes termed incurable visual defectsFrom EverandOculopathy: Disproves the orthodox and theoretical bases upon which glasses are so freely prescribed, and puts forward natural remedial methods of treatment for what are sometimes termed incurable visual defectsNo ratings yet
- Refractive Errors: Dr. Kemal DikiciDocument77 pagesRefractive Errors: Dr. Kemal DikiciFirman CappoNo ratings yet
- Aspheric IOLs Fact vs MythDocument8 pagesAspheric IOLs Fact vs MythAnonymous h0DxuJTNo ratings yet
- NLE 2015 Questions SampleDocument8 pagesNLE 2015 Questions SampleJona Suarez100% (4)
- GastricDocument207 pagesGastricfavo riteNo ratings yet
- Aao Irregular AstigmatismDocument16 pagesAao Irregular AstigmatismnurulrezqiaNo ratings yet
- Clinical Applications of Wavefront Aberrometry - A ReviewDocument12 pagesClinical Applications of Wavefront Aberrometry - A ReviewMashhoor AlfayezNo ratings yet
- Cacat Lensa (Aberration)Document46 pagesCacat Lensa (Aberration)PaulinaNo ratings yet
- AstigmatismDocument5 pagesAstigmatismTaimur RashidNo ratings yet
- Pemeriksaan ObejktifDocument12 pagesPemeriksaan ObejktifMuhammad FadhilNo ratings yet
- Optical AberrationDocument20 pagesOptical AberrationShubhangi ShuklaNo ratings yet
- 07 AstigmatismDocument20 pages07 AstigmatismMwanja MosesNo ratings yet
- Add Slide AbberationDocument119 pagesAdd Slide AbberationRaissaNo ratings yet
- The Aberrometer - Measuring Aberrations of The Eye: Retina CorneaDocument3 pagesThe Aberrometer - Measuring Aberrations of The Eye: Retina CorneaEdvania AlvesNo ratings yet
- Measuring Lens Focal Length with Wavefront AnalysisDocument13 pagesMeasuring Lens Focal Length with Wavefront AnalysisZafar IqbalNo ratings yet
- citation-233414409Document8 pagescitation-233414409drjatinvaziraniNo ratings yet
- Journal Article RetinosDocument4 pagesJournal Article RetinosJenny VillanuevaNo ratings yet
- Corneal Topography: Presented by Maj Anjani Kumar Resident (Ophth)Document71 pagesCorneal Topography: Presented by Maj Anjani Kumar Resident (Ophth)Yaman MuhaisenNo ratings yet
- Refractive ErrorsDocument38 pagesRefractive ErrorszahraaNo ratings yet
- 08 Optical AberrationsDocument19 pages08 Optical AberrationsMwanja MosesNo ratings yet
- ASTIGMATISM1Document31 pagesASTIGMATISM1sath3028No ratings yet
- Useful For Fixation and FoggingDocument12 pagesUseful For Fixation and FogginganggastavasthiNo ratings yet
- Monochromatic Aberrations and Point-Spread FunctioDocument9 pagesMonochromatic Aberrations and Point-Spread FunctioFozlerabbi AnandoNo ratings yet
- Problems With Wavefront Aberrations Applied To Refractive Surgery: Developing StandardsDocument10 pagesProblems With Wavefront Aberrations Applied To Refractive Surgery: Developing Standardsmvs_newNo ratings yet
- Measuring corneal and ocular aberrationsDocument65 pagesMeasuring corneal and ocular aberrationsPaulEstrellaNo ratings yet
- 05a) Pupils and Stops - 1 - 25Document9 pages05a) Pupils and Stops - 1 - 25Rosa VelázquezNo ratings yet
- Retinal Image Quality of A Human Eye Model - OSLO LT SoftwareDocument11 pagesRetinal Image Quality of A Human Eye Model - OSLO LT SoftwareRadu BabauNo ratings yet
- KERATOMETRYDocument3 pagesKERATOMETRYMarjune DimayugaNo ratings yet
- DownloadDocument8 pagesDownloadVersatile VpNo ratings yet
- EF Lens Work Book 10 enDocument25 pagesEF Lens Work Book 10 enSilvana HadžićNo ratings yet
- Understanding Corneal TopographyDocument12 pagesUnderstanding Corneal TopographyWagner de AvizNo ratings yet
- Salmon 2003Document9 pagesSalmon 2003Andrea GilNo ratings yet
- v3 2 07 PDFDocument15 pagesv3 2 07 PDFArif MohammadNo ratings yet
- 10 Aberration Theory Part IDocument42 pages10 Aberration Theory Part IxbNo ratings yet
- Presentation 0310192016Document103 pagesPresentation 0310192016itsme.chandlermbingNo ratings yet
- Anterior Chamber Angle Assessment TechniquesDocument7 pagesAnterior Chamber Angle Assessment TechniquesSabyasachiNo ratings yet
- Chapter 4 CameraDocument9 pagesChapter 4 CameraAbiñon Clark Kevin T.No ratings yet
- Oblique astigmatism explainedDocument1 pageOblique astigmatism explainedajay anandNo ratings yet
- Phase Contrast MicrosDocument7 pagesPhase Contrast Micros9791617898No ratings yet
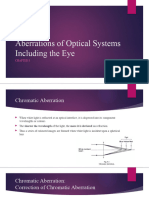
- Aberrations of Optical Systems Including The EyeDocument20 pagesAberrations of Optical Systems Including The EyeCherry OrtegaNo ratings yet
- Aberration of LightDocument9 pagesAberration of LightNaymur RahmanNo ratings yet
- Aberration: Aberration Is Something That Deviates From The Normal Way But Has Several Specifically DefinedDocument16 pagesAberration: Aberration Is Something That Deviates From The Normal Way But Has Several Specifically Definedyash_yadav85No ratings yet
- Akurasi Total Pengukuran Kornea Pada Astigmat Dengan Gambaran Scheimpflug Dan Menyinarkan Cahaya Warna Diode Topografi KorneaDocument16 pagesAkurasi Total Pengukuran Kornea Pada Astigmat Dengan Gambaran Scheimpflug Dan Menyinarkan Cahaya Warna Diode Topografi Kornearia mutiaraNo ratings yet
- Etiology and Clinical Presentation of Astigmatism: February 2012Document19 pagesEtiology and Clinical Presentation of Astigmatism: February 2012dean evansNo ratings yet
- Ho 2010Document6 pagesHo 2010Sarah Camacho PinedaNo ratings yet
- CH 9Document13 pagesCH 9dadingafgiNo ratings yet
- Astigmatism 140302140740 Phpapp01Document22 pagesAstigmatism 140302140740 Phpapp01Claudia SerbanNo ratings yet
- Refraction, Correction of Refractive ErrorsDocument16 pagesRefraction, Correction of Refractive ErrorsAgung Rizka PratamaNo ratings yet
- Seidel AberrationsDocument2 pagesSeidel AberrationsalvaroNo ratings yet
- Wavefront Sensor Using Shack-Hartmann PrincipleDocument33 pagesWavefront Sensor Using Shack-Hartmann PrinciplePrince John PrincipeNo ratings yet
- Cornealtopographybysuraj 160507151045Document112 pagesCornealtopographybysuraj 160507151045Ridho HariyadiNo ratings yet
- Update On Astigmatism ManagementDocument5 pagesUpdate On Astigmatism ManagementInggitaDarmawanNo ratings yet
- Primary Eye Examination: A Comprehensive Guide to DiagnosisFrom EverandPrimary Eye Examination: A Comprehensive Guide to DiagnosisJong-Soo LeeNo ratings yet
- Daftar PustakaDocument4 pagesDaftar PustakanurulrezqiaNo ratings yet
- Daftar Obat-ObatanDocument1 pageDaftar Obat-ObatannurulrezqiaNo ratings yet
- LOGBOOK REFRAKSI, LENSA KONTAK, LOW VISION (Kegiatan Diagnosis)Document7 pagesLOGBOOK REFRAKSI, LENSA KONTAK, LOW VISION (Kegiatan Diagnosis)nurulrezqiaNo ratings yet
- Daftar PustakaDocument1 pageDaftar PustakanurulrezqiaNo ratings yet
- Daftar ObatDocument1 pageDaftar ObatnurulrezqiaNo ratings yet
- Numbers Sheet Name Numbers Table NameDocument32 pagesNumbers Sheet Name Numbers Table NamenurulrezqiaNo ratings yet
- Ijcm 2014071513394601 PDFDocument9 pagesIjcm 2014071513394601 PDFnurulrezqiaNo ratings yet
- Time Out: Nama: RM: TGL Lahir: Diagnosa: Visus Pre Op: Tindakan: Power Iol: Gds / TD: Hbsag/ A. HCV: OperatorDocument1 pageTime Out: Nama: RM: TGL Lahir: Diagnosa: Visus Pre Op: Tindakan: Power Iol: Gds / TD: Hbsag/ A. HCV: OperatornurulrezqiaNo ratings yet
- 5.daftar PustakaDocument2 pages5.daftar PustakanurulrezqiaNo ratings yet
- Elektrokardiografi & AritmiaDocument78 pagesElektrokardiografi & AritmianurulrezqiaNo ratings yet
- 5.daftar PustakaDocument2 pages5.daftar PustakanurulrezqiaNo ratings yet
- MumpsDocument2 pagesMumpsnurulrezqiaNo ratings yet
- National Cardiovascular Center Harapan KitaDocument20 pagesNational Cardiovascular Center Harapan KitanurulrezqiaNo ratings yet
- Neonatal Breast Hypertrophy RevisitedDocument2 pagesNeonatal Breast Hypertrophy Revisitedabas karimNo ratings yet
- Journal of Health Global 2018Document344 pagesJournal of Health Global 2018Rizki Agung PrasetyoNo ratings yet
- YouTube Promotes BrandsDocument6 pagesYouTube Promotes BrandsSilpi YuliantiNo ratings yet
- ResumedieteticinternshipDocument1 pageResumedieteticinternshipapi-208833628No ratings yet
- Consolidated Activities LGCDD LGMEDDocument8 pagesConsolidated Activities LGCDD LGMEDRegion PersonnelNo ratings yet
- Gene TherapyDocument3 pagesGene TherapyGleeson Jay NiedoNo ratings yet
- Novi Lestari 1911304150 B3Document3 pagesNovi Lestari 1911304150 B3FarahNo ratings yet
- Biology 2nd Test CH Wise V1Document14 pagesBiology 2nd Test CH Wise V1ashfaq4985No ratings yet
- Nursing Student Documents Liver Disease CaseDocument2 pagesNursing Student Documents Liver Disease CaseQuinonez Anna MarieNo ratings yet
- Autacoids For Med.Document140 pagesAutacoids For Med.Feysal AhmedNo ratings yet
- 63D17 391 Nyi Mas Siti PurwaningsihDocument4 pages63D17 391 Nyi Mas Siti PurwaningsihAstridNo ratings yet
- Saltwater Power: Samal National High SchoolDocument47 pagesSaltwater Power: Samal National High SchoolKhloe EppohsNo ratings yet
- Solution Manual For An Integrated Approach To Health Sciences Anatomy and Physiology Math Chemistry and Medical Microbiology 2nd EditionDocument4 pagesSolution Manual For An Integrated Approach To Health Sciences Anatomy and Physiology Math Chemistry and Medical Microbiology 2nd EditionKaraWalkerixpe100% (38)
- Microparticle Clearence Theory of Mechansim of Wet Cupping Therapy (Al-Hijama)Document5 pagesMicroparticle Clearence Theory of Mechansim of Wet Cupping Therapy (Al-Hijama)AdmirNo ratings yet
- Schisto. in The Phils. & CaragaDocument56 pagesSchisto. in The Phils. & CaragaHoneylet Ü Ferol100% (2)
- FACTORS AFFECTING THE PUBLIC SPEAKING FA - OdtDocument16 pagesFACTORS AFFECTING THE PUBLIC SPEAKING FA - OdtKenneth BitunNo ratings yet
- Literature Review On BloodDocument7 pagesLiterature Review On Bloodafmzinuvouzeny100% (1)
- Ferulic Acid Alleviates Lipid Peroxidation in Diabetic RatsDocument5 pagesFerulic Acid Alleviates Lipid Peroxidation in Diabetic RatsrrukkumaniNo ratings yet
- Thinners MSDSDocument7 pagesThinners MSDSManuel CardosoNo ratings yet
- Maxillary Impacted Canines: A Clinical Review: DR Rajiv Yadav, DR Basanta K. ShresthaDocument6 pagesMaxillary Impacted Canines: A Clinical Review: DR Rajiv Yadav, DR Basanta K. Shresthadrzana78No ratings yet
- 1577un 2026-01Document79 pages1577un 2026-01ngovantienNo ratings yet
- U - Book-Studies 53no4-Robarge-Passages-Corrected1Mar PDFDocument104 pagesU - Book-Studies 53no4-Robarge-Passages-Corrected1Mar PDFMehmetZekeriyaÖztürkNo ratings yet