You might also like
- Traction: Cervical & LumbarDocument21 pagesTraction: Cervical & LumbarBoud ElhassanNo ratings yet
- Spinal TraumaDocument81 pagesSpinal TraumaharilNo ratings yet
- Wilson, D.S., Hayes, S.C. & Biglan, A. (2018). Evolution and contextual behavioral science an integrated framework for understanding, predicting and influencing human behavior. Oakland Context Press..pdfDocument390 pagesWilson, D.S., Hayes, S.C. & Biglan, A. (2018). Evolution and contextual behavioral science an integrated framework for understanding, predicting and influencing human behavior. Oakland Context Press..pdfjesus100% (3)
- Body Mechanics: Fundamental of Nursing IDocument55 pagesBody Mechanics: Fundamental of Nursing Irlinao100% (3)
- The Best Abdominal Exercises You've Never Heard Of: 77 Unique Ab-Blasting ExercisesFrom EverandThe Best Abdominal Exercises You've Never Heard Of: 77 Unique Ab-Blasting ExercisesRating: 5 out of 5 stars5/5 (3)
- Cervical & Lumbar Traction GuideDocument21 pagesCervical & Lumbar Traction Guidevinayman100% (1)
- Closed Chain Exercises: Dominic S. Adolfo, PTRPDocument56 pagesClosed Chain Exercises: Dominic S. Adolfo, PTRPEric Carlos YumulNo ratings yet
- Enhancing the Benefits of Nauli with a Key Exercise for Abdominal Muscle StrengthFrom EverandEnhancing the Benefits of Nauli with a Key Exercise for Abdominal Muscle StrengthRating: 5 out of 5 stars5/5 (1)
- Range of Motion ExerciseDocument8 pagesRange of Motion ExerciseAmit Martin83% (6)
- Primary and Secondary Adhesive Capsulitis Etiology, Stages, Signs, Tests and ManagementDocument8 pagesPrimary and Secondary Adhesive Capsulitis Etiology, Stages, Signs, Tests and ManagementVanessa Yvonne Gurtiza100% (1)
- Active Isolated Stretching The Mattes Method 61 90Document33 pagesActive Isolated Stretching The Mattes Method 61 90Nazareth Varas AlonsoNo ratings yet
- Coreandlumbopelvic Stabilizationinrunners: Carlos E. RiveraDocument19 pagesCoreandlumbopelvic Stabilizationinrunners: Carlos E. RiveraAndrea PimentelNo ratings yet
- Spinal StabilizationDocument32 pagesSpinal StabilizationLakshita PrajapatiNo ratings yet
- Diabetes and Insulin Signaling Case StudyDocument3 pagesDiabetes and Insulin Signaling Case StudyJoey Ma100% (2)
- TractionDocument42 pagesTractionThasheela V0% (2)
- Range of MotionDocument59 pagesRange of MotionIsrael Jiel Fedelicio100% (1)
- International Monetary Financial Economics 1st Edition Daniels Test BankDocument26 pagesInternational Monetary Financial Economics 1st Edition Daniels Test BankStacieSharpnocje100% (52)
- Maitland Joint MobilizationDocument40 pagesMaitland Joint Mobilizationkitu_alagappan472060% (5)
- Laws of Organization in Perceptual Forms Max Wertheimer (1923) Classics in The History of Psychology - Wertheimer 1923Document14 pagesLaws of Organization in Perceptual Forms Max Wertheimer (1923) Classics in The History of Psychology - Wertheimer 1923redavhtradNo ratings yet
- Chapter 2 - General Characteristics of The SpineDocument50 pagesChapter 2 - General Characteristics of The SpineveronicalovirgenNo ratings yet
- Pharmaceutical Care Plan - Sample Version: (Dispensing and Medication Safety)Document4 pagesPharmaceutical Care Plan - Sample Version: (Dispensing and Medication Safety)Angela Pabico RosarioNo ratings yet
- Spinal TractionDocument45 pagesSpinal TractionArun Tamilvanan100% (3)
- Range of Motion and Mobility ExercisesDocument64 pagesRange of Motion and Mobility ExercisesMae Arra Gilbao Lecobu-anNo ratings yet
- MobilisationDocument97 pagesMobilisationMegha Patani100% (1)
- Range of Motion Exercises &Document47 pagesRange of Motion Exercises &Nikita Sharma100% (1)
- Traction: Presented by - Pooja BhowadDocument26 pagesTraction: Presented by - Pooja BhowadManpreet KaurNo ratings yet
- Proprioceptive Neuromuscular Facilitation Techniques in RehabilitationDocument19 pagesProprioceptive Neuromuscular Facilitation Techniques in Rehabilitationapi-241271253100% (1)
- Functional Reach TestDocument1 pageFunctional Reach TestMuhammad JuniarsyahNo ratings yet
- Suspension TherapyDocument39 pagesSuspension TherapyFarrukh Shahzad100% (5)
- Traction: Cervical & LumbarDocument21 pagesTraction: Cervical & LumbarSEGERD01No ratings yet
- TractionDocument21 pagesTractionMuhammad FahmyNo ratings yet
- Rotator Cuff TendinitisDocument23 pagesRotator Cuff TendinitisVrushali NikamNo ratings yet
- WINDLASS MECHANISMDocument3 pagesWINDLASS MECHANISMmuhammad kaleemNo ratings yet
- Hip, Knee, Ankle PROMDocument28 pagesHip, Knee, Ankle PROMsxsparsh2305No ratings yet
- Traction in ORTHOPAEDICSDocument16 pagesTraction in ORTHOPAEDICSJuswa ViasonNo ratings yet
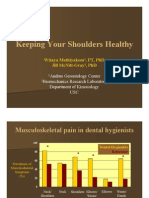
- Keeping Your Shoulders HealthyDocument38 pagesKeeping Your Shoulders Healthyxyz84No ratings yet
- Suspension Therapy of Upper and Lower LimbDocument23 pagesSuspension Therapy of Upper and Lower LimbM Farrukh shahzad100% (6)
- Spanish SquatDocument7 pagesSpanish Squatapi-551757456No ratings yet
- Balance, Posture and Body AlignmentDocument6 pagesBalance, Posture and Body AlignmenthahahahaaaaaaaNo ratings yet
- LECT 8 Relieving The Discomforts of Pregnancy Part 1Document27 pagesLECT 8 Relieving The Discomforts of Pregnancy Part 1Umer RafiqNo ratings yet
- Proper Lifting Techniques and Risk Factors for Back InjuriesDocument38 pagesProper Lifting Techniques and Risk Factors for Back InjurieszainabnoorNo ratings yet
- Angle of Pull and Pulley by Hamza MirDocument25 pagesAngle of Pull and Pulley by Hamza MirAmeer HamzaNo ratings yet
- FUNDA REVIEW 2 Body MechanicsDocument27 pagesFUNDA REVIEW 2 Body Mechanicslovie dooNo ratings yet
- PNF TechniquesDocument26 pagesPNF Techniquesabdul haseebNo ratings yet
- Mobility and ActivityDocument39 pagesMobility and ActivityneehoshiNo ratings yet
- Lafarge Construction Ergonomics in The WorkplaceDocument48 pagesLafarge Construction Ergonomics in The WorkplacehksNo ratings yet
- Manual Muscle TestingDocument13 pagesManual Muscle TestingPásztai ZoltánNo ratings yet
- Postural Prescriptions for Peak PerformanceDocument29 pagesPostural Prescriptions for Peak PerformanceLeon SamadiNo ratings yet
- Range of Muscle Work.Document54 pagesRange of Muscle Work.Salman KhanNo ratings yet
- Positioning ChartDocument11 pagesPositioning CharttifferschangNo ratings yet
- Microprocessor Knee UnitsDocument54 pagesMicroprocessor Knee UnitsKumar BalramNo ratings yet
- TractionDocument39 pagesTractionLu IsNo ratings yet
- Selecting Appropriate and Effective EquipmentDocument63 pagesSelecting Appropriate and Effective EquipmentTransverse Myelitis AssociationNo ratings yet
- Transfer and AmbulationDocument108 pagesTransfer and AmbulationGladys YaresNo ratings yet
- StartingPositions Derived PositionsDocument53 pagesStartingPositions Derived PositionsTobit Andre CaballoNo ratings yet
- JP JP JP JPDocument7 pagesJP JP JP JPLean Ashly Tuddao MacarubboNo ratings yet
- Traction & Application of p0pDocument19 pagesTraction & Application of p0pSham NazrinNo ratings yet
- Traction Day 2Document3 pagesTraction Day 2shushmaNo ratings yet
- Topic 14 PT 201 - Upright Motor Control, Infant, Toddler and ChildrenDocument50 pagesTopic 14 PT 201 - Upright Motor Control, Infant, Toddler and ChildrenEJ GejonNo ratings yet
- Active Isolated Stretching The Mattes Method 151 184Document38 pagesActive Isolated Stretching The Mattes Method 151 184Nazareth Varas AlonsoNo ratings yet
- Body Posture & Lifting-8Document89 pagesBody Posture & Lifting-8Shafiq Mohd NorNo ratings yet
- 5 Calisthenics: SupplementsDocument13 pages5 Calisthenics: SupplementsPranavNo ratings yet
- Groin InjuryDocument17 pagesGroin Injurymateh ur rehmanNo ratings yet
- Body Posture and LiftingDocument88 pagesBody Posture and LiftingShafiq Mohd NorNo ratings yet
- SCI and TBI ManagementDocument40 pagesSCI and TBI ManagementAlif AndiniNo ratings yet
- TKR ProtocolDocument8 pagesTKR ProtocolSandeep SoniNo ratings yet
- Physical Agents & Electrotherapy II: DR - Muhammad Shahid Shabbir DPT, Ms - NMPTDocument38 pagesPhysical Agents & Electrotherapy II: DR - Muhammad Shahid Shabbir DPT, Ms - NMPTMISS. COMNo ratings yet
- HW-7 Female Athlete TriadDocument13 pagesHW-7 Female Athlete TriadMISS. COMNo ratings yet
- Stress and ManagementDocument32 pagesStress and ManagementMISS. COMNo ratings yet
- GCU Faisalabad DPT 6th Semester Fall 2022 Time TableDocument1 pageGCU Faisalabad DPT 6th Semester Fall 2022 Time TableMISS. COMNo ratings yet
- Manual Therapy: Dr. Amna Haider Lecturer ZIHSDocument76 pagesManual Therapy: Dr. Amna Haider Lecturer ZIHSMISS. COMNo ratings yet
- Ultraviolet Radiation 2Document28 pagesUltraviolet Radiation 2MISS. COMNo ratings yet
- Genetic Disorders Lec # 6Document43 pagesGenetic Disorders Lec # 6MISS. COMNo ratings yet
- IntegratedDocument47 pagesIntegratedMISS. COMNo ratings yet
- Infra Red Radiation: Iqra - Ishaq@tuf - Edu.pkDocument49 pagesInfra Red Radiation: Iqra - Ishaq@tuf - Edu.pkMISS. COMNo ratings yet
- Ultrasound Therapy Guide Under 40 CharactersDocument52 pagesUltrasound Therapy Guide Under 40 CharactersMISS. COMNo ratings yet
- Lecture 7-Cervical BiomechanicsDocument32 pagesLecture 7-Cervical BiomechanicsMISS. COMNo ratings yet
- HW 2Document16 pagesHW 2MISS. COMNo ratings yet
- Ethics in Health ServicesDocument16 pagesEthics in Health ServicesMISS. COMNo ratings yet
- HW 2Document16 pagesHW 2MISS. COMNo ratings yet
- Hexose Monophosphate Pathway or Shunt (HMP ShuntDocument28 pagesHexose Monophosphate Pathway or Shunt (HMP ShuntMISS. COMNo ratings yet
- ArthroplastyDocument21 pagesArthroplastyMISS. COMNo ratings yet
- BERG BALANCE TESTS AND RATING SCALEDocument4 pagesBERG BALANCE TESTS AND RATING SCALEINDO' NURULNo ratings yet
- Health and Wellness: Key Concepts of FitnessDocument40 pagesHealth and Wellness: Key Concepts of FitnessMISS. COMNo ratings yet
- Biomechanics of Fracture FixationDocument21 pagesBiomechanics of Fracture FixationMISS. COMNo ratings yet
- Ex Prescrition For Speacial PopulationDocument54 pagesEx Prescrition For Speacial PopulationMISS. COMNo ratings yet
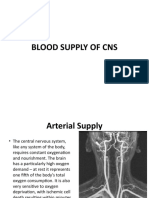
- NEUROANATOMY Lecture # 07 (BLOOD SUPPLY OF CNS)Document26 pagesNEUROANATOMY Lecture # 07 (BLOOD SUPPLY OF CNS)MISS. COMNo ratings yet
- Pancreas Structure and FunctionsDocument11 pagesPancreas Structure and FunctionsCheng XinvennNo ratings yet
- Notice: Environmental Statements Notice of Intent: U. S. Navy Surveillance Towed Array Sensor System Low Frequency Active Sonar OperationsDocument2 pagesNotice: Environmental Statements Notice of Intent: U. S. Navy Surveillance Towed Array Sensor System Low Frequency Active Sonar OperationsJustia.comNo ratings yet
- Foundation of Professional Nursing PracticeDocument5 pagesFoundation of Professional Nursing PracticeIvan LouiseNo ratings yet
- Podocyturia As A DiagnosticMarker For Preeclampsia 2012Document6 pagesPodocyturia As A DiagnosticMarker For Preeclampsia 2012Diapositivas08No ratings yet
- Time 120Document3 pagesTime 120ardhra pNo ratings yet
- Parent2007-Adult Neurogenesis Dentate GyrusDocument13 pagesParent2007-Adult Neurogenesis Dentate Gyrusiulia andreeaNo ratings yet
- ReportDocument2 pagesReportCherey BaguioNo ratings yet
- Reviews: Lipid Nanoparticles For mRNA DeliveryDocument77 pagesReviews: Lipid Nanoparticles For mRNA DeliverySeah Jia huiNo ratings yet
- ThesisDocument36 pagesThesisjeff clude torrenoNo ratings yet
- Heredity and EvolutionDocument29 pagesHeredity and EvolutionAnisha ThomasNo ratings yet
- S1 DPG Jeffrey A 2014 Bordtella Pertussis PathogenesisDocument15 pagesS1 DPG Jeffrey A 2014 Bordtella Pertussis PathogenesisAyerim Valeria Rojas DiazNo ratings yet
- Pendahuluan, Metabolit Primer Dan Sekunder PDFDocument85 pagesPendahuluan, Metabolit Primer Dan Sekunder PDFViena CynthiaNo ratings yet
- MSDS Praepagen HYDocument92 pagesMSDS Praepagen HYAngelicaNo ratings yet
- Kahoot 1Document6 pagesKahoot 1Nida RidzuanNo ratings yet
- Perspectives For Using Rna Sequencing Analysis of The Genome To Understand The Mechanisms of AgingDocument3 pagesPerspectives For Using Rna Sequencing Analysis of The Genome To Understand The Mechanisms of AgingHerald Scholarly Open AccessNo ratings yet
- Potato Spindle Tuber Viroid (PSTVD)Document4 pagesPotato Spindle Tuber Viroid (PSTVD)Leydi Yudith Angarita BautistaNo ratings yet
- Dinosaur Field Guide Supplement 2nd EdDocument111 pagesDinosaur Field Guide Supplement 2nd EdAdamNo ratings yet
- Jeopardy Game 5-Topic Template TaigaDocument54 pagesJeopardy Game 5-Topic Template TaigaDylan SleasmanNo ratings yet
- WHO 4th Intl Standard For HCVDocument2 pagesWHO 4th Intl Standard For HCVSagir AlvaNo ratings yet
- Gastric TypeDocument4 pagesGastric TypeleartaNo ratings yet
- Biol3451 Ch4 LectDocument60 pagesBiol3451 Ch4 LectcolabrinkNo ratings yet
- Application of "Dispersive Liquid-Liquid Micro Extraction Technique" For The Analysis of Piroxicam in Human Urine and Drug FormulationDocument16 pagesApplication of "Dispersive Liquid-Liquid Micro Extraction Technique" For The Analysis of Piroxicam in Human Urine and Drug FormulationInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Blood (Notes)Document12 pagesBlood (Notes)Angel Rose BrillanteNo ratings yet