You might also like
- HAZOP ExerciseDocument12 pagesHAZOP Exerciseshawalina07No ratings yet
- FMEA TrainingDocument45 pagesFMEA TrainingSanjay Parekh100% (2)
- GOLDEN DAWN 5 6, Magical EucharistDocument5 pagesGOLDEN DAWN 5 6, Magical EucharistF_RC100% (3)
- PFMEA AdvancedDocument22 pagesPFMEA AdvancedslagmercuryNo ratings yet
- Advanced PFMEADocument22 pagesAdvanced PFMEAHassan KhanNo ratings yet
- FMEA: Failure Modes and Effects AnalysisDocument24 pagesFMEA: Failure Modes and Effects AnalysisAlvaro CotaquispeNo ratings yet
- FMEADocument10 pagesFMEAsriramoj100% (1)
- Problem Solving and Analysis Tools Failure Modes and Effects Analysis - FmeaDocument7 pagesProblem Solving and Analysis Tools Failure Modes and Effects Analysis - FmeaAhmed M. HashimNo ratings yet
- Process Failure Mode Effect Analysis: CA/PA-RCA: Advanced ToolDocument22 pagesProcess Failure Mode Effect Analysis: CA/PA-RCA: Advanced ToolshivendrakumarNo ratings yet
- Analyze Opportunity Part 1: Failure Modes Effect Analysis (FMEA)Document36 pagesAnalyze Opportunity Part 1: Failure Modes Effect Analysis (FMEA)Viswanathan SrkNo ratings yet
- Failure Mode and Effects Analysis (Design) : Importance in NPD ProcessDocument12 pagesFailure Mode and Effects Analysis (Design) : Importance in NPD Processsushant3240No ratings yet
- FMEA DeckDocument20 pagesFMEA Deckgogisetty100% (1)
- Analyze Opportunity Part 1: Failure Modes Effect Analysis (FMEA)Document36 pagesAnalyze Opportunity Part 1: Failure Modes Effect Analysis (FMEA)Viswanathan SrkNo ratings yet
- FMEA Failure Modes Effects Analysis PDFDocument32 pagesFMEA Failure Modes Effects Analysis PDFVILLANUEVA_DANIEL2064100% (1)
- EMT 480 Reliability & Failure AnalysisDocument38 pagesEMT 480 Reliability & Failure AnalysisK ULAGANATHANNo ratings yet
- FMEA - ASQ&APICS Joint MeetingDocument31 pagesFMEA - ASQ&APICS Joint Meetingjagger zgNo ratings yet
- FMEA ProcessDocument7 pagesFMEA ProcessRANJITHNo ratings yet
- 10 Steps To Conduct A DFMEADocument5 pages10 Steps To Conduct A DFMEAkirthi83No ratings yet
- TQM Unit 4 FMEA Lecture 6Document17 pagesTQM Unit 4 FMEA Lecture 6tamilselvansambathNo ratings yet
- Yale FMEA IntroDocument24 pagesYale FMEA Introhazwan2283No ratings yet
- FMEA TrainingDocument25 pagesFMEA Trainingmelimaulani-1No ratings yet
- Failure Mode and Effects Analysis in Reliability CenteredDocument41 pagesFailure Mode and Effects Analysis in Reliability CenteredAkanksha KumariNo ratings yet
- 203 LSS Gbo - FmeaDocument47 pages203 LSS Gbo - FmeaRocker byNo ratings yet
- The Purpose of An FMEADocument22 pagesThe Purpose of An FMEAKishanNo ratings yet
- 1 CT AmefDocument23 pages1 CT AmefCuenta PokemonNo ratings yet
- Fmea and FmecaDocument14 pagesFmea and FmecaLindsay SleijpenNo ratings yet
- FMEADocument24 pagesFMEARaajha MunibathiranNo ratings yet
- MainFEMA SKH PDFDocument46 pagesMainFEMA SKH PDFswapan kumar hazraNo ratings yet
- Introduction To Failure ModeDocument10 pagesIntroduction To Failure ModeAMIT THAKKARNo ratings yet
- Hazen Alrasyid (3333160102)Document14 pagesHazen Alrasyid (3333160102)Ihadz CleverleyNo ratings yet
- Prem Kumar SDocument24 pagesPrem Kumar SPrem KumarNo ratings yet
- Failure Mode: Professor: IE Johnnathan Fernando Gutiérrez CruzDocument39 pagesFailure Mode: Professor: IE Johnnathan Fernando Gutiérrez CruzCuenta PokemonNo ratings yet
- Qgem Management Solution: Welcomes You To Failure Mode & Effects Analysis (Fmea) Training Course 4 EditionDocument103 pagesQgem Management Solution: Welcomes You To Failure Mode & Effects Analysis (Fmea) Training Course 4 EditionVINOTH100% (2)
- 2020 Failure Mode and Effects AnalysisDocument40 pages2020 Failure Mode and Effects AnalysisEvri LiaNo ratings yet
- 20bba0194 TQM Da 1 FmeaDocument9 pages20bba0194 TQM Da 1 Fmeavani sureshNo ratings yet
- FMEADocument20 pagesFMEARonillo PormonNo ratings yet
- Presentation Class FMEADocument37 pagesPresentation Class FMEACuenta PokemonNo ratings yet
- 2010 RAMS Lessons Learned Effective FmeasDocument29 pages2010 RAMS Lessons Learned Effective FmeasEduardo BrásNo ratings yet
- 2.failure Mode and Effective Analysis - 1 SlideDocument36 pages2.failure Mode and Effective Analysis - 1 SlideAriq CahyantoNo ratings yet
- How To Use The Failure Modes and Effects Analysis Template: A Benchmarking and Improvements ToolDocument4 pagesHow To Use The Failure Modes and Effects Analysis Template: A Benchmarking and Improvements ToolsahirlyesNo ratings yet
- TRIZ Method by Genrich AltshullerDocument5 pagesTRIZ Method by Genrich AltshullerAnonymous JyrLl3RNo ratings yet
- Konferensi PerawatDocument159 pagesKonferensi PerawatdroenNo ratings yet
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument9 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsEduardo Pérez R.No ratings yet
- PFMEADocument13 pagesPFMEASarigameNo ratings yet
- Presentation On FmeaDocument15 pagesPresentation On FmeaA Veda SagarNo ratings yet
- FMEADocument36 pagesFMEAAnoop PrajapatiNo ratings yet
- Failure Mode and Effects Analysis (FMEA)Document37 pagesFailure Mode and Effects Analysis (FMEA)Charlie Tubaon100% (3)
- 2011 RAMS Lessons Learned For Effective FmeasDocument9 pages2011 RAMS Lessons Learned For Effective FmeasAbuzar AliNo ratings yet
- FMEA Failure Mode Effect AnalysisDocument61 pagesFMEA Failure Mode Effect AnalysisAbhijeet RandhirNo ratings yet
- Failure Mode & Effect Analysis: Haroon ChughtaiDocument16 pagesFailure Mode & Effect Analysis: Haroon ChughtaiOwaisNo ratings yet
- TQM Live Lecture 11 Apr 2021 1618022055727Document27 pagesTQM Live Lecture 11 Apr 2021 1618022055727Kumar AbhishekNo ratings yet
- Appendix: Failure Mode and Effects Analysis (FMEA) and House of QualityDocument16 pagesAppendix: Failure Mode and Effects Analysis (FMEA) and House of QualityJan GeerkensNo ratings yet
- FMEA ObjectiveDocument2 pagesFMEA ObjectivenyanaprgasamNo ratings yet
- TQM, Lecture-11+12Document18 pagesTQM, Lecture-11+12Shakeel AhmadNo ratings yet
- Bug Defect Triage ProcessDocument20 pagesBug Defect Triage Processraulnq50% (2)
- TOT FMEA Presentation 4th April 2024Document21 pagesTOT FMEA Presentation 4th April 2024aungmyokyaw300386No ratings yet
- Experiment No 7 MEMDocument11 pagesExperiment No 7 MEMImdad JalaliNo ratings yet
- Troubleshooting and Root Cause Failure Analysis: Equipment Problem SolvingFrom EverandTroubleshooting and Root Cause Failure Analysis: Equipment Problem SolvingRating: 4.5 out of 5 stars4.5/5 (3)
- Practical Guide to FMEA : A Proactive Approach to Failure AnalysisFrom EverandPractical Guide to FMEA : A Proactive Approach to Failure AnalysisRating: 5 out of 5 stars5/5 (1)
- Machine Reliability and Condition Monitoring: A Comprehensive Guide to Predictive Maintenance PlanningFrom EverandMachine Reliability and Condition Monitoring: A Comprehensive Guide to Predictive Maintenance PlanningRating: 4.5 out of 5 stars4.5/5 (2)
- FMEA konkret: Preventive risk analysis concretely with FMEA plus. The series of successful developers, trainers and presenters.From EverandFMEA konkret: Preventive risk analysis concretely with FMEA plus. The series of successful developers, trainers and presenters.No ratings yet
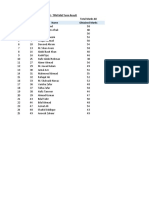
- TPM - MId Term ResultDocument1 pageTPM - MId Term ResultZeeshan ElahiNo ratings yet
- TPM Mid Term Exam 21st July 2022 - Zeeshan ElahiDocument4 pagesTPM Mid Term Exam 21st July 2022 - Zeeshan ElahiZeeshan ElahiNo ratings yet
- TPM Mid Term Exam 21st July 2022 - Zeeshan ElahiDocument4 pagesTPM Mid Term Exam 21st July 2022 - Zeeshan ElahiZeeshan ElahiNo ratings yet
- TPM Lecture 12Document12 pagesTPM Lecture 12Zeeshan ElahiNo ratings yet
- TPM Lecture 10Document19 pagesTPM Lecture 10Zeeshan Elahi100% (1)
- TPM Lecture 09Document21 pagesTPM Lecture 09Zeeshan ElahiNo ratings yet
- Lec # 05Document24 pagesLec # 05Zeeshan ElahiNo ratings yet
- Lec 06Document26 pagesLec 06Zeeshan ElahiNo ratings yet
- Antenna LecDocument20 pagesAntenna Lecjosesag518No ratings yet
- Platinum Gazette 21 MayDocument16 pagesPlatinum Gazette 21 MayAnonymous w8NEyXNo ratings yet
- Assignment 2.1soap 1Document5 pagesAssignment 2.1soap 1Anonymous mX5wWmGNo ratings yet
- Thegaslawscomplete 120227061412 Phpapp01Document51 pagesThegaslawscomplete 120227061412 Phpapp01Bustami Muhammad Sidik100% (1)
- Ca-P IFU 897N203599A enDocument2 pagesCa-P IFU 897N203599A enenrique santillanNo ratings yet
- DLL - Mapeh 4 - Q2 - W3Document6 pagesDLL - Mapeh 4 - Q2 - W3Janet Escosura Espinosa MadayagNo ratings yet
- Matt Zwier - Freelance - Metropolitan Radiation Oncology BrochureDocument2 pagesMatt Zwier - Freelance - Metropolitan Radiation Oncology BrochureMattNo ratings yet
- Exercise and SclerodermaDocument22 pagesExercise and SclerodermaLupin TohNo ratings yet
- Powerware 9: FeaturesDocument2 pagesPowerware 9: Featuresandy175No ratings yet
- BEE SafetyManualDocument196 pagesBEE SafetyManualAmeenudeenNo ratings yet
- Sahaj - MedicalDocument5 pagesSahaj - Medical'Living DollNo ratings yet
- E CA19-9ms en 20Document3 pagesE CA19-9ms en 20Hassan GillNo ratings yet
- Energy Argus Petroleum Coke PDFDocument20 pagesEnergy Argus Petroleum Coke PDFChandan Jst100% (1)
- Brochure Isolation Valves Product Overview en en 5253576Document36 pagesBrochure Isolation Valves Product Overview en en 5253576Muthu Kumar RNo ratings yet
- 8454 - Formulir Tanpa Judul (Respons)Document32 pages8454 - Formulir Tanpa Judul (Respons)Yelina KusumaNo ratings yet
- Indicador NT 200aDocument53 pagesIndicador NT 200alisita23_182No ratings yet
- Thought Translation DeviceDocument2 pagesThought Translation DeviceArun SudanNo ratings yet
- News Items Test Baru 3Document6 pagesNews Items Test Baru 3Afif FatahNo ratings yet
- Lymph Node Removal (Lymphadenectomy) - Health Information - Bupa UKDocument10 pagesLymph Node Removal (Lymphadenectomy) - Health Information - Bupa UKFanti Aldesia HafildNo ratings yet
- Amri Dodo!Document12 pagesAmri Dodo!Alfred PatrickNo ratings yet
- KAMP Syllabus Nova FinalDocument4 pagesKAMP Syllabus Nova FinalShailendra100% (1)
- Direct Dyes What Is Direct Dye?Document3 pagesDirect Dyes What Is Direct Dye?MD. Tofazzal HossainNo ratings yet
- Green Fingers Organic FarmsDocument17 pagesGreen Fingers Organic FarmsajdeclandNo ratings yet
- Entanglement-Based Secure Quantum Cryptography Over 1,120 KilometresDocument18 pagesEntanglement-Based Secure Quantum Cryptography Over 1,120 KilometresFredy OrjuelaNo ratings yet
- Transport Phenomena 2Document9 pagesTransport Phenomena 2Kaify PeshmergaNo ratings yet
- Trans-Boundary Fisheries Resources Management (Compatibility Mode)Document16 pagesTrans-Boundary Fisheries Resources Management (Compatibility Mode)KruNont MatchPointNo ratings yet
- 1 s2.0 S0960148122010187 MainDocument16 pages1 s2.0 S0960148122010187 MainJuan VeraNo ratings yet
- Battery Charger Series: PowerbaseDocument1 pageBattery Charger Series: PowerbaseCristopher Jason Lopez CansinoNo ratings yet
- Infectious or Communicable Diseases: TuberculosisDocument7 pagesInfectious or Communicable Diseases: TuberculosischandraNo ratings yet