You might also like
- Growth AssessmentDocument190 pagesGrowth AssessmentAjay ChhetriNo ratings yet
- Methods of Studying Growth: Vivekandha Dental College For WomenDocument65 pagesMethods of Studying Growth: Vivekandha Dental College For WomennivethaseshaNo ratings yet
- Radiology in Pediatric DentistryDocument125 pagesRadiology in Pediatric DentistryHebah NawafNo ratings yet
- Growth AssessmentDocument65 pagesGrowth Assessmentdr parveen bathlaNo ratings yet
- Methods of Studying GrowthDocument17 pagesMethods of Studying GrowthMUSHAHID HASANNo ratings yet
- Introduksi Radiologi KonvensionalDocument47 pagesIntroduksi Radiologi KonvensionalYon AditamaNo ratings yet
- Dental RadiologyDocument30 pagesDental RadiologyRobertNo ratings yet
- Vivek PPT Mri Vs SDocument20 pagesVivek PPT Mri Vs SVivek ChNo ratings yet
- Supplementary DIagnostic AidsDocument186 pagesSupplementary DIagnostic AidsRajshekhar Banerjee100% (1)
- Intra-Oral Radiographic TechniquesDocument163 pagesIntra-Oral Radiographic TechniquesdrdeepsomrNo ratings yet
- Role of Radiology in Musculoskeletal System: Hawler Medical University College of Medicine Radiology UnitDocument37 pagesRole of Radiology in Musculoskeletal System: Hawler Medical University College of Medicine Radiology UnitHisham 6ChomanyNo ratings yet
- Principles and Application of Investigative and Imaging Techniques-1Document43 pagesPrinciples and Application of Investigative and Imaging Techniques-1Lal NandaniNo ratings yet
- Lec 8 Cep Halo MetricDocument12 pagesLec 8 Cep Halo MetricHuda AljaderiNo ratings yet
- Me 471-Bio-Engineering / Bio-Medical Topics: Ioninzing RadiationDocument7 pagesMe 471-Bio-Engineering / Bio-Medical Topics: Ioninzing RadiationehteshamalhanifNo ratings yet
- Recent Advances in Diagnostic AidsDocument59 pagesRecent Advances in Diagnostic AidsShubham NagrathNo ratings yet
- T2-Pemeriksaan Radiologis Kelainan Sistem MuskuloskeletalDocument48 pagesT2-Pemeriksaan Radiologis Kelainan Sistem MuskuloskeletalDesy Suryani PaisNo ratings yet
- Basic Concepts of Growth & Development: Presented byDocument31 pagesBasic Concepts of Growth & Development: Presented bySnehjyoti JhaNo ratings yet
- Septic ArthritisDocument94 pagesSeptic ArthritisCut Riska NovizaNo ratings yet
- K.19 Introduksi Co Ass CCDocument33 pagesK.19 Introduksi Co Ass CCSyafiraNo ratings yet
- Elastography in DentistryDocument33 pagesElastography in DentistryimmortalneoNo ratings yet
- Diagnostics in Dental ImplantologyDocument54 pagesDiagnostics in Dental ImplantologyDrkvpratheep Pratheep100% (2)
- Radiological Investigations: Mri & PetDocument59 pagesRadiological Investigations: Mri & PetDeeptanu GhoshNo ratings yet
- DMFR 20140229-1Document6 pagesDMFR 20140229-1aswad 0008No ratings yet
- Supplementary Diagnostic Aids in OrthodonticsDocument121 pagesSupplementary Diagnostic Aids in OrthodonticsSrinivasan Boovaraghavan0% (1)
- Lecture 1 (1) Introduction To Medical ImagingDocument18 pagesLecture 1 (1) Introduction To Medical Imagingalfredo gutierrezNo ratings yet
- Soft-Tissue Thickness Values UsingDocument5 pagesSoft-Tissue Thickness Values UsingAdrian ToalaNo ratings yet
- Role of IN Oral & Maxillofacial Surgery: Mri ImagingDocument34 pagesRole of IN Oral & Maxillofacial Surgery: Mri ImagingAKSHAYA SUBHASHINEE DNo ratings yet
- Three-Dimensional Cephalometry: Richard L. JacobsonDocument6 pagesThree-Dimensional Cephalometry: Richard L. Jacobsonsnes182No ratings yet
- 7368693Document56 pages7368693Mylena Ch100% (1)
- 7.1. Skeletal SystemDocument111 pages7.1. Skeletal Systemmirabel IvanaliNo ratings yet
- Introduction 2017Document118 pagesIntroduction 2017dindaNo ratings yet
- Cephalometric SrachaelDocument130 pagesCephalometric Srachaelابو العزNo ratings yet
- 2006 @dentallib Alexander Jacobson, Richard L Jacobson RadiographicDocument321 pages2006 @dentallib Alexander Jacobson, Richard L Jacobson Radiographicilter burak köse67% (6)
- Seminar Presentation On NeuroimagingDocument67 pagesSeminar Presentation On Neuroimagingdemeke tsegayeNo ratings yet
- Ceph Write Up / Orthodontic Courses by Indian Dental AcademyDocument36 pagesCeph Write Up / Orthodontic Courses by Indian Dental Academyindian dental academyNo ratings yet
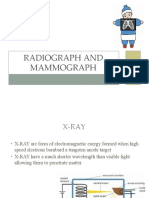
- Radiograph and MammographDocument23 pagesRadiograph and MammographHarsimran KaurNo ratings yet
- Intra Oral Radiography: - Presented byDocument34 pagesIntra Oral Radiography: - Presented byNehal MainaliNo ratings yet
- POD - 01a MSK RadiologyDocument34 pagesPOD - 01a MSK RadiologySara BasheerNo ratings yet
- Clinical Skill Diagnostic Imaging Approach SMST 2Document42 pagesClinical Skill Diagnostic Imaging Approach SMST 2Devi YuliantiNo ratings yet
- Introduction To Clinical RadiologyDocument38 pagesIntroduction To Clinical RadiologyMUBIRU SAMUEL EDWARDNo ratings yet
- Orthodontics: Cephalometric Analysis Cephalometric Landmarks, Planes & AnglesDocument11 pagesOrthodontics: Cephalometric Analysis Cephalometric Landmarks, Planes & AnglesQueen LiveNo ratings yet
- Sindrome de EagleDocument7 pagesSindrome de EagleEl GalenoNo ratings yet
- CBCT in OrthodonticsDocument73 pagesCBCT in OrthodonticsdrgreeshmahariniNo ratings yet
- Diagnosis in ImplantsDocument11 pagesDiagnosis in ImplantsAkshay GajakoshNo ratings yet
- Temporo-Mandibular Joint. Implantology and Paradontology: Catedra de Radiologie Și Imagistică MedicalăDocument125 pagesTemporo-Mandibular Joint. Implantology and Paradontology: Catedra de Radiologie Și Imagistică Medicalăovidiu.opreaNo ratings yet
- Growth PredictionDocument64 pagesGrowth PredictionMothi KrishnaNo ratings yet
- Lecture#1 1Document10 pagesLecture#1 1Afsheen ZaibNo ratings yet
- USS Imaging Techniques WA2018Document38 pagesUSS Imaging Techniques WA2018Jake MillerNo ratings yet
- The Role of Ioc in Sarcoma SurgeryDocument31 pagesThe Role of Ioc in Sarcoma SurgeryLILA RUSTIKANo ratings yet
- Radiology in EndodonticsDocument107 pagesRadiology in EndodonticsMohamed kamelNo ratings yet
- Three Dimensional DIAGNOSISDocument120 pagesThree Dimensional DIAGNOSISsakthivel ramNo ratings yet
- Methods of Study Bone Growth / Orthodontic Courses by Indian Dental AcademyDocument38 pagesMethods of Study Bone Growth / Orthodontic Courses by Indian Dental Academyindian dental academyNo ratings yet
- Dasar-Dasar Radiologi Musculoskeletal PDFDocument101 pagesDasar-Dasar Radiologi Musculoskeletal PDFIndra MahaputraNo ratings yet
- Diagnostic Aids in ProsthodonticsDocument60 pagesDiagnostic Aids in ProsthodonticsAME DENTAL COLLEGE RAICHUR, KARNATAKANo ratings yet
- Screenshot 2023-04-15 at 6.21.50 PM PDFDocument22 pagesScreenshot 2023-04-15 at 6.21.50 PM PDFMustafa S. JaberNo ratings yet
- Introduction to Diffusion Tensor Imaging: And Higher Order ModelsFrom EverandIntroduction to Diffusion Tensor Imaging: And Higher Order ModelsNo ratings yet
- Introduksi RadiologiDocument40 pagesIntroduksi RadiologiDeden SiswantoNo ratings yet
- IndicationDocument70 pagesIndicationPKS 1988No ratings yet
- Intrusion Arches ShinuDocument66 pagesIntrusion Arches ShinuYuvashreeNo ratings yet
- Muscle FunctionDocument28 pagesMuscle FunctionYuvashreeNo ratings yet
- Loops and RetractionDocument24 pagesLoops and RetractionYuvashreeNo ratings yet
- CALCIUM AND PHOSPHOROUS METABOLISM-finalDocument31 pagesCALCIUM AND PHOSPHOROUS METABOLISM-finalYuvashreeNo ratings yet
- Controversies in OrthodonticsDocument115 pagesControversies in OrthodonticsYuvashree100% (2)
- Common Sense MechanicsDocument36 pagesCommon Sense MechanicsYuvashreeNo ratings yet
- Bonding7 7 04.Document86 pagesBonding7 7 04.YuvashreeNo ratings yet
- 3.theories, Growth StudiesDocument66 pages3.theories, Growth StudiesYuvashreeNo ratings yet
- Bonding MaterialsDocument178 pagesBonding MaterialsYuvashreeNo ratings yet
- 6) Space AnalysisDocument135 pages6) Space AnalysisYuvashree50% (2)
- Cranial BaseDocument47 pagesCranial BaseYuvashreeNo ratings yet
- Classification of MalocclusionDocument51 pagesClassification of MalocclusionYuvashreeNo ratings yet
- 1.G&D-basic Concepts NewDocument35 pages1.G&D-basic Concepts NewYuvashreeNo ratings yet
- 1.concepts of Growth & DevelopmentDocument107 pages1.concepts of Growth & DevelopmentYuvashreeNo ratings yet
- Theories of GrowthDocument137 pagesTheories of GrowthYuvashreeNo ratings yet
- Vertical Maxillary ExcessDocument125 pagesVertical Maxillary ExcessYuvashreeNo ratings yet
- Neural Crest CellsDocument33 pagesNeural Crest CellsYuvashreeNo ratings yet
- Sample Events Operation PlanDocument18 pagesSample Events Operation PlanPhuong NhungNo ratings yet
- Prema V Opalustre MIHDocument8 pagesPrema V Opalustre MIHbrigidgaffneyNo ratings yet
- BioMedical Waste Management Issues ChallengesDocument23 pagesBioMedical Waste Management Issues ChallengesArun Shree RNo ratings yet
- Lab Clin Clin Tasks Attempted 1 2 3 4 5 6 7: ST ND RD TH TH TH THDocument4 pagesLab Clin Clin Tasks Attempted 1 2 3 4 5 6 7: ST ND RD TH TH TH THRichard Patterson100% (1)
- Peterborough Public Health COVID-19 Weekly Situational ReportDocument3 pagesPeterborough Public Health COVID-19 Weekly Situational ReportPeterborough ExaminerNo ratings yet
- Pencarrow Lighthouse Conservation PlanDocument98 pagesPencarrow Lighthouse Conservation PlanClarice Futuro MuhlbauerNo ratings yet
- Current State of Alzheimer'S Disease Research and TherapeuticsDocument382 pagesCurrent State of Alzheimer'S Disease Research and TherapeuticsyusufNo ratings yet
- Non-Hodgkin Lymphoma (NHL)Document11 pagesNon-Hodgkin Lymphoma (NHL)archanaNo ratings yet
- Somatics Article, by Thomas HannaDocument16 pagesSomatics Article, by Thomas HannaEugenia Clandestina Ferrario100% (4)
- Revised ThesisDocument51 pagesRevised ThesisOfficial Lara Delos SantosNo ratings yet
- PRIME Appetite and Weight Reduction Daily Food Plan For The HCG Diet: Monday - ThursdayDocument1 pagePRIME Appetite and Weight Reduction Daily Food Plan For The HCG Diet: Monday - ThursdayskydivercoNo ratings yet
- Gender ReassignmentDocument4 pagesGender ReassignmentDaphne Susana PaulinNo ratings yet
- General Objecti-Wps OfficeDocument3 pagesGeneral Objecti-Wps OfficeSumit YadavNo ratings yet
- Unit4 Planning For A Health CareerDocument76 pagesUnit4 Planning For A Health CareerkitcathNo ratings yet
- Urinary Tract Infections in ChildrenDocument16 pagesUrinary Tract Infections in ChildrenPraluki HerliawanNo ratings yet
- Dyspepsia On CommonDocument21 pagesDyspepsia On CommonChatrina TandiloloNo ratings yet
- Polysomnograph EnglishDocument5 pagesPolysomnograph EnglishRam BehinNo ratings yet
- Local Food Trade Shows ProgramDocument39 pagesLocal Food Trade Shows ProgramAmy KleinNo ratings yet
- Analysis State of The Nation Address (SONA)Document2 pagesAnalysis State of The Nation Address (SONA)K CateNo ratings yet
- Practice Station History Breathless 1Document8 pagesPractice Station History Breathless 1Wenbin GuoNo ratings yet
- DapusDocument7 pagesDapusPutriPasaribuNo ratings yet
- Swine Flu - Read About Symptoms, Treatment and H1N1 VaccineDocument10 pagesSwine Flu - Read About Symptoms, Treatment and H1N1 VaccineRoyal ENo ratings yet
- Diode Laser Therapy Systems: E-Beauty MachineDocument40 pagesDiode Laser Therapy Systems: E-Beauty Machinekhaled khalasNo ratings yet
- Aaha Dental Guidelines PDFDocument21 pagesAaha Dental Guidelines PDFGianfranco DanziNo ratings yet
- Curie Breakthrough by SlidesgoDocument47 pagesCurie Breakthrough by SlidesgoRai YugiNo ratings yet
- SbarDocument3 pagesSbarCharlie65129No ratings yet
- Anxiety Disorders and Their Treatment Antony-Swinson-1996Document123 pagesAnxiety Disorders and Their Treatment Antony-Swinson-1996Ruxandra CraciunNo ratings yet
- Guadalquiver v. Sea Power Shipping Enterprise, Inc. GR No. 226200Document2 pagesGuadalquiver v. Sea Power Shipping Enterprise, Inc. GR No. 226200Maynard Gabayno100% (1)
- Guide To Application For Registration of Medicinal Products - 4th EditiDocument142 pagesGuide To Application For Registration of Medicinal Products - 4th EditiKdp03No ratings yet
- Diagnostic Centers MOU FormDocument5 pagesDiagnostic Centers MOU FormMuhammad Usman Ghani100% (1)