You might also like
- NP Performance Appraisal Sample PDFDocument2 pagesNP Performance Appraisal Sample PDFHamss Ahmed80% (5)
- Revisiting The Fascist Subtext of Attack On Titan - Some Notes On A Modern Reactionary AnimeDocument10 pagesRevisiting The Fascist Subtext of Attack On Titan - Some Notes On A Modern Reactionary AnimeSouthern FuturistNo ratings yet
- Axe - Positioning - v0.2Document6 pagesAxe - Positioning - v0.2Karthik Kota100% (1)
- Ong v. BognalbalDocument2 pagesOng v. BognalbalStefanRodriguez100% (3)
- Fractures and Low Back Pain: Dr. Lubna DwerijDocument49 pagesFractures and Low Back Pain: Dr. Lubna DwerijNoor MajaliNo ratings yet
- Nur 149 - p3w3 - Fri - Session 23 - FracturesDocument52 pagesNur 149 - p3w3 - Fri - Session 23 - FracturesAlliah Marie CababarosNo ratings yet
- Fracture 190706114534Document61 pagesFracture 190706114534Precious BlessingNo ratings yet
- Fraktur Terbuka Dan TertutupDocument19 pagesFraktur Terbuka Dan TertutupVilza maharaniNo ratings yet
- Types of Fractures and Healing StagesDocument45 pagesTypes of Fractures and Healing Stagesanupama varghese100% (1)
- Orthopaedic Surgery Fractures and Dislocations: Tomas Kurakovas MF LL Group 29Document13 pagesOrthopaedic Surgery Fractures and Dislocations: Tomas Kurakovas MF LL Group 29Tomas Kurakovas100% (1)
- Fracture PP Ahmad Aqel 2013Document32 pagesFracture PP Ahmad Aqel 2013ahmadNo ratings yet
- MusculoskelealDocument32 pagesMusculoskelealEbuka AniNo ratings yet
- Bone FractureDocument10 pagesBone FractureDat boi100% (1)
- FractureDocument27 pagesFractureAkio OzaragaNo ratings yet
- Fracture: Presented By: Ms. Durga Joshi M. SC NursingDocument63 pagesFracture: Presented By: Ms. Durga Joshi M. SC NursingSanjaya PutraNo ratings yet
- Fracture Nursing Care Management: Study GuideDocument5 pagesFracture Nursing Care Management: Study Guidezahwa ayundaNo ratings yet
- Fracture 140717081851 Phpapp02Document63 pagesFracture 140717081851 Phpapp02Jaylord VerazonNo ratings yet
- Understanding Intertrochanteric Fractures of the FemurDocument12 pagesUnderstanding Intertrochanteric Fractures of the FemurEinz Nur Amalyah IdrusNo ratings yet
- Frakktur Kelompok 15 (English) PDFDocument45 pagesFrakktur Kelompok 15 (English) PDFTri WulandariSemester 1BNo ratings yet
- Fracture: Group 1Document29 pagesFracture: Group 1Louisse Angeli AbucejoNo ratings yet
- Bone FractureDocument10 pagesBone Fractureraphael chidiebereNo ratings yet
- Lo MSK 2-3Document6 pagesLo MSK 2-3FirmanHidayatNo ratings yet
- Fracture: Suchithra.P.V 1 Year Msc. Nursing College of Nursing AlappuzhaDocument96 pagesFracture: Suchithra.P.V 1 Year Msc. Nursing College of Nursing AlappuzhaAakash A. AgrawalNo ratings yet
- Management of Musculoskeletal InjuriesDocument102 pagesManagement of Musculoskeletal InjuriesMaria Lynne Parambita100% (1)
- Fracture FinalDocument56 pagesFracture FinalnobelaugustineNo ratings yet
- A Closed Fracture Does Not Penetrate The SkinDocument5 pagesA Closed Fracture Does Not Penetrate The SkinIvan Liquiran Avenado100% (1)
- Open FractureDocument9 pagesOpen FractureAnnyl LaurelNo ratings yet
- Fractures: Mary Grace B. Gutierrez Resti Mariano Ma. Cindy O. BautistaDocument50 pagesFractures: Mary Grace B. Gutierrez Resti Mariano Ma. Cindy O. BautistaJustin Ahorro-DionisioNo ratings yet
- Fracture: Prepared By: Jamito, Anisa A. & Mauna, AlaysaDocument37 pagesFracture: Prepared By: Jamito, Anisa A. & Mauna, AlaysaBella DonnaNo ratings yet
- Types and Treatment of FracturesDocument68 pagesTypes and Treatment of FracturesokaciaNo ratings yet
- Introduction of FractureDocument80 pagesIntroduction of Fracturealsead798No ratings yet
- FRACTUREDocument16 pagesFRACTUREPriyaNo ratings yet
- Fracture Nursing CareDocument6 pagesFracture Nursing CareRizqi LutfiNo ratings yet
- Traumatic InjuryDocument64 pagesTraumatic InjuryDYRAH GRACE COPAUSNo ratings yet
- Orthopedic EmergenciesDocument75 pagesOrthopedic EmergenciesAlex beharuNo ratings yet
- NCP: Nursing Care Plan For Bone FracturesDocument8 pagesNCP: Nursing Care Plan For Bone FracturesElham TabaoNo ratings yet
- Fracture PP Ahmad Aqel 2013Document32 pagesFracture PP Ahmad Aqel 2013aqel605859No ratings yet
- NUR 202 Musculoskeletal Surgery 9.5.22Document64 pagesNUR 202 Musculoskeletal Surgery 9.5.22Merve kdkkNo ratings yet
- Orthopedic NursingDocument19 pagesOrthopedic NursingDa BondadNo ratings yet
- Management of Open FracturesDocument8 pagesManagement of Open FracturesAndreas KristianNo ratings yet
- Orthopedic SurgeryDocument14 pagesOrthopedic SurgerySajjad LaghariNo ratings yet
- My Lesson Plan: Closed Fracture Distal 3rd Right Radius Ulna, Secondary To FallDocument6 pagesMy Lesson Plan: Closed Fracture Distal 3rd Right Radius Ulna, Secondary To Fallshenecajean carajayNo ratings yet
- FractureDocument34 pagesFractureDwi Kurnia SariNo ratings yet
- Care StudyDocument27 pagesCare StudyFavourNo ratings yet
- 3-Fracture 1Document36 pages3-Fracture 1Radwa TalaatNo ratings yet
- Fracture Case AbstractDocument27 pagesFracture Case AbstractMaribel Briones JuanNo ratings yet
- Maja Musculo Sceletal-NovaDocument18 pagesMaja Musculo Sceletal-NovaLuka KoloskiNo ratings yet
- Bone FracturesDocument26 pagesBone FracturesgwynNo ratings yet
- Nursing Management of A Patient With Close FractureDocument15 pagesNursing Management of A Patient With Close FractureJoshuaYapNo ratings yet
- Physiology & Injries in SportsDocument17 pagesPhysiology & Injries in Sportsashvirchatha3No ratings yet
- FracturesDocument44 pagesFracturesCaptain AmericaNo ratings yet
- Untitled Presentation 4Document13 pagesUntitled Presentation 4api-619359087No ratings yet
- Conservative Treatment of Diaphyseal Fractures of Tibia andDocument40 pagesConservative Treatment of Diaphyseal Fractures of Tibia andsaihaNo ratings yet
- La Consolacion College Manila: Femoral Neck FractureDocument3 pagesLa Consolacion College Manila: Femoral Neck FractureIvan Liquiran AvenadoNo ratings yet
- Musculoskeletal TraumaDocument103 pagesMusculoskeletal TraumaJona Kristin EnclunaNo ratings yet
- Classification of FracturesDocument26 pagesClassification of FracturesHoney May Rollan VicenteNo ratings yet
- Principles of Bone Fracture HealingDocument62 pagesPrinciples of Bone Fracture HealingFuad AbdullahNo ratings yet
- Nursing Management: Musculoskeletal Trauma and Orthopedic SurgeryDocument25 pagesNursing Management: Musculoskeletal Trauma and Orthopedic SurgeryDeannahTampusNo ratings yet
- Bahaa Motawea. #. & DislocationsDocument51 pagesBahaa Motawea. #. & DislocationsFathy AlhallagNo ratings yet
- 10 - Musculoskeletal InjuriesDocument8 pages10 - Musculoskeletal InjuriesEastern SamarNo ratings yet
- Types of FracturesDocument10 pagesTypes of Fracturesazeencancer2003No ratings yet
- Types of Bone Fractures and Common Traction MethodsDocument3 pagesTypes of Bone Fractures and Common Traction MethodsMarc AnchetaNo ratings yet
- Fractures: Pathophysiology and EtiologyDocument5 pagesFractures: Pathophysiology and EtiologyHafid JuniorNo ratings yet
- Elbow Injury Guidelines for Grappling AthletesFrom EverandElbow Injury Guidelines for Grappling AthletesNo ratings yet
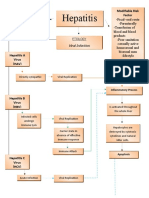
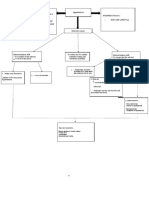
- Hepatitis TracingDocument2 pagesHepatitis TracingCatherine M. EbajanNo ratings yet
- Hypokalemia PathoDocument9 pagesHypokalemia PathoCatherine M. EbajanNo ratings yet
- Tracing HyperkalemiaDocument3 pagesTracing HyperkalemiaCatherine M. EbajanNo ratings yet
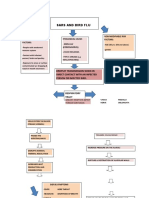
- SARS and Bird Flu Risk Factors and TransmissionDocument2 pagesSARS and Bird Flu Risk Factors and TransmissionCatherine M. EbajanNo ratings yet
- 10th MICROCURRICULAR - PLANNING PROJECT 1Document7 pages10th MICROCURRICULAR - PLANNING PROJECT 1Vinicio Marcelo ChicaizaNo ratings yet
- Recommended Curriculum: Seven (7) Types of CurriculumDocument1 pageRecommended Curriculum: Seven (7) Types of CurriculummoyesaNo ratings yet
- Empirical and Molecular Formulas WK SHTDocument8 pagesEmpirical and Molecular Formulas WK SHTAnnaReyesNo ratings yet
- Instructions For Filling-Up The Application Form (Online)Document9 pagesInstructions For Filling-Up The Application Form (Online)Himaghna DasguptaNo ratings yet
- Lal Bahadur ShastriDocument17 pagesLal Bahadur Shastribhaskar124970No ratings yet
- Hughie's Financial StatusDocument3 pagesHughie's Financial StatusGuna SeelanNo ratings yet
- Long Call Vs Short Put: Presented byDocument9 pagesLong Call Vs Short Put: Presented bygovardhanNo ratings yet
- An Introduction To Identification & Intervention For Children With Sensory Processing DifficultiesDocument92 pagesAn Introduction To Identification & Intervention For Children With Sensory Processing DifficultiesFrancisca CondutoNo ratings yet
- CARAVAL - Opening ExtractDocument29 pagesCARAVAL - Opening ExtractHodder Stoughton100% (1)
- Medium Term Plan On Teaching Scratch in Year 4Document5 pagesMedium Term Plan On Teaching Scratch in Year 4api-272550320No ratings yet
- Life, Works and Writings of RizalDocument6 pagesLife, Works and Writings of RizalPatrickMendozaNo ratings yet
- MUET Reading Task - Print OutDocument5 pagesMUET Reading Task - Print Out萱儿林No ratings yet
- Ferriols, Roque J. - A Memoir of Six YearsDocument4 pagesFerriols, Roque J. - A Memoir of Six YearsCharlene TanNo ratings yet
- Criminal LiabilityDocument3 pagesCriminal LiabilityAqZarNo ratings yet
- England's Warrior Queen BoudicaDocument1 pageEngland's Warrior Queen Boudicachrisgreen4905No ratings yet
- Hospital Sector Data Analysis: Price, Market Cap, Sales & Valuation RatiosDocument3 pagesHospital Sector Data Analysis: Price, Market Cap, Sales & Valuation RatiosYash SinghalNo ratings yet
- Sandeep Kumar KommareddyDocument1 pageSandeep Kumar KommareddysandeepNo ratings yet
- Thiruppugal Pathigam - Song 923 ("Madhi-Yālvi - Thagan-Āgi")Document7 pagesThiruppugal Pathigam - Song 923 ("Madhi-Yālvi - Thagan-Āgi")apjbalamuruganNo ratings yet
- Population and Responsible Parenthood ReportDocument15 pagesPopulation and Responsible Parenthood ReportJo Anne May BalnajaNo ratings yet
- Gupea 2077 37037 1Document46 pagesGupea 2077 37037 1Guilherme PeresNo ratings yet
- Manifestation With Urgent Motion To Cancel ArraignmentDocument4 pagesManifestation With Urgent Motion To Cancel ArraignmentAlkaios RonquilloNo ratings yet
- Andrew Balkin - CapstoneDocument147 pagesAndrew Balkin - CapstoneTrần Tâm PhươngNo ratings yet
- Friedan Explores "Problem With No NameDocument13 pagesFriedan Explores "Problem With No NameRoxana Daniela AjderNo ratings yet
- Food Chain Gizmo WorksheetDocument5 pagesFood Chain Gizmo Worksheetvictoria gagroNo ratings yet
- Easychair Preprint: Mansi Panjwani, Rahul Ramrakhiani, Hitesh Jumnani, Krishna Zanwar and Rupali HandeDocument9 pagesEasychair Preprint: Mansi Panjwani, Rahul Ramrakhiani, Hitesh Jumnani, Krishna Zanwar and Rupali Handeimrul emonNo ratings yet
- Kidnapping: Nurul Asyikeen HJ Abdul Jabar DBML MSUDocument9 pagesKidnapping: Nurul Asyikeen HJ Abdul Jabar DBML MSUPrushotaman NadarajahNo ratings yet