You might also like
- Surgical Site Infection DR WidDocument36 pagesSurgical Site Infection DR WidNia UswantiNo ratings yet
- Clinic-Pharmacologic Approaches To Antimicrobial Therapy in Surgical InfectionsDocument27 pagesClinic-Pharmacologic Approaches To Antimicrobial Therapy in Surgical InfectionsMuhammad NaveedNo ratings yet
- 5.surgical Infections LectureDocument56 pages5.surgical Infections LectureBiruk DesalegnNo ratings yet
- Antibiotic Selection GuideDocument37 pagesAntibiotic Selection GuideAbanoub Nabil100% (1)
- Bacterial PathogenesisDocument36 pagesBacterial Pathogenesisapi-19969058100% (3)
- Necrotizing Fasciitis..By DR Kassahun GirmaDocument49 pagesNecrotizing Fasciitis..By DR Kassahun GirmaKassahun Girma GelawNo ratings yet
- Antimicrobial Prophylaxis For Prevention of Surgical Site Infection in AdultsDocument59 pagesAntimicrobial Prophylaxis For Prevention of Surgical Site Infection in Adultsbolohan biatriceNo ratings yet
- 2016 Antifungal Agent Full PDFDocument16 pages2016 Antifungal Agent Full PDFyeni novi yantiNo ratings yet
- Bisotat For MlsDocument57 pagesBisotat For MlsABAYNo ratings yet
- Pathology Bleeding DisordersDocument67 pagesPathology Bleeding DisordersMarcelliaNo ratings yet
- Primary Immunodeficiency DiseasesDocument24 pagesPrimary Immunodeficiency DiseasesClaire Henderson100% (1)
- Vancomycin & Vancomycin Resistant Enterococci: Abdullah M. Kharbosh, B.SC., PharmDocument78 pagesVancomycin & Vancomycin Resistant Enterococci: Abdullah M. Kharbosh, B.SC., Pharmkharbosham100% (1)
- Genetic RecombinationDocument25 pagesGenetic RecombinationChandrashekhar UnakalNo ratings yet
- Evaluation of Coagulation Disorders - FINALDocument34 pagesEvaluation of Coagulation Disorders - FINALRatna Stephenson BasimallaNo ratings yet
- Arthroplasty JournalDocument3 pagesArthroplasty Journallina yohanes100% (1)
- Hemostasis and Thrombosis: Practical Guidelines in Clinical ManagementFrom EverandHemostasis and Thrombosis: Practical Guidelines in Clinical ManagementHussain I. SabaNo ratings yet
- Tissue and Organs of The Immune System: Learning GoalsDocument113 pagesTissue and Organs of The Immune System: Learning Goalsbright nvachirawit100% (1)
- Antimicrobial Therapy in Sepsis PDFDocument38 pagesAntimicrobial Therapy in Sepsis PDFTatik HandayaniNo ratings yet
- Chemical Mediators of InflammationDocument46 pagesChemical Mediators of Inflammationroohi khanNo ratings yet
- 2 Transplantation ImmunologyDocument33 pages2 Transplantation Immunologykirubel getyeNo ratings yet
- Cohort StudyDocument46 pagesCohort StudydrnareshchauhanNo ratings yet
- General Principles of Combination ChemotherapyDocument40 pagesGeneral Principles of Combination Chemotherapyoncology KMC-KnlNo ratings yet
- Study Designs in EpidemiologyDocument34 pagesStudy Designs in EpidemiologyPawan BaraiNo ratings yet
- Immunopharmacology: Dr. Hamad AlshabiDocument8 pagesImmunopharmacology: Dr. Hamad AlshabiHamad Alshabi100% (1)
- Rational Antibiotic Usage and Antibiotic Policy - Dr. FirmansyahDocument76 pagesRational Antibiotic Usage and Antibiotic Policy - Dr. Firmansyahjay neefNo ratings yet
- Pathology 5.05a CervixDocument6 pagesPathology 5.05a CervixDranreb Berylle MasangkayNo ratings yet
- 1.rationale of Use of Antibiotic in Surgical Patients CDocument22 pages1.rationale of Use of Antibiotic in Surgical Patients CPanna SahaNo ratings yet
- Procalcitonin Guided Antibiotic TherapyDocument20 pagesProcalcitonin Guided Antibiotic TherapyhziglamNo ratings yet
- Cohort Study.. Design, Steps, Analysis: Dr. Jatin ChhayaDocument33 pagesCohort Study.. Design, Steps, Analysis: Dr. Jatin ChhayaShivani ShahNo ratings yet
- Transplantation Immunology PDFDocument99 pagesTransplantation Immunology PDFVictoriaNo ratings yet
- Crispr TechniqueDocument16 pagesCrispr TechniqueAmmar Abbas100% (1)
- Tumors of The Small Tumors of The Small and and Large Intestines Large IntestinesDocument18 pagesTumors of The Small Tumors of The Small and and Large Intestines Large Intestinespal_pal_pal100% (1)
- Measures of Disease Frequency NOTESDocument22 pagesMeasures of Disease Frequency NOTESSJ Jung100% (1)
- 03 The Modern Age of MicrobiologyDocument5 pages03 The Modern Age of Microbiologysabrinalugo85No ratings yet
- Surgical InfectionsDocument54 pagesSurgical InfectionsManish Shrestha100% (1)
- Diagnosis and Management of Upper Gastrointestinal Bleeding PDFDocument10 pagesDiagnosis and Management of Upper Gastrointestinal Bleeding PDFKetut Suwadiaya P AdnyanaNo ratings yet
- Infectious Diseases - Infective EndocarditisDocument41 pagesInfectious Diseases - Infective Endocarditisfire_n_iceNo ratings yet
- Refkas CondylomaAccuminataDocument18 pagesRefkas CondylomaAccuminatamichelle1945No ratings yet
- New Basic Epi IntroDocument52 pagesNew Basic Epi Introaktaruzzaman bethuNo ratings yet
- Cohort StudyDocument37 pagesCohort Studygilbert2691No ratings yet
- Fungal Infections in The IcuDocument23 pagesFungal Infections in The IcuVemuri SrinivasNo ratings yet
- Opioids A ReviewDocument19 pagesOpioids A ReviewAlan padilla sesma100% (1)
- Hypersensitivity StatesDocument40 pagesHypersensitivity StatesMorrison NjageNo ratings yet
- Arthritis, Infectious, BacterialDocument6 pagesArthritis, Infectious, BacterialHarry IsraNo ratings yet
- Febrile Neutropenia: Nontapak ThiangpakDocument53 pagesFebrile Neutropenia: Nontapak ThiangpakRapid MedicineNo ratings yet
- Rational Use of AntibioticsDocument85 pagesRational Use of AntibioticsAHMAD MAHIR BIN CHE RAHMATNo ratings yet
- Antibiotic in OmfsDocument47 pagesAntibiotic in OmfsRajat GuptaNo ratings yet
- UTI Guidelines IDSA 2010Document18 pagesUTI Guidelines IDSA 2010Ati'ul Ma'rifah HambalyNo ratings yet
- Measuring Health and DiseaseDocument25 pagesMeasuring Health and DiseaseMNBNo ratings yet
- Incidence and Prevalence PDFDocument9 pagesIncidence and Prevalence PDFSreya SanilNo ratings yet
- Surgical InfectionsDocument310 pagesSurgical InfectionsOmar Ed ChavezNo ratings yet
- Vancomycin Auc With Answers 1Document64 pagesVancomycin Auc With Answers 1api-493355126No ratings yet
- BiostatisticsQUIZ AnswersDocument5 pagesBiostatisticsQUIZ AnswersDipankar RoyNo ratings yet
- Obese Patients - Medication Dosing RQHR - 3Document8 pagesObese Patients - Medication Dosing RQHR - 3Sarah Zielda NajibNo ratings yet
- Rational Use of AntibioticsDocument32 pagesRational Use of AntibioticsRendy SusantoNo ratings yet
- InflammationDocument41 pagesInflammationbharath goNo ratings yet
- Drug Therapy of TB, 2015Document44 pagesDrug Therapy of TB, 2015FongChanyipNo ratings yet
- Study DesignDocument34 pagesStudy DesignVikashgtmNo ratings yet
- Second Year: 2.1 Pathophysiolog Y (Theory)Document15 pagesSecond Year: 2.1 Pathophysiolog Y (Theory)Prashanth RajuNo ratings yet
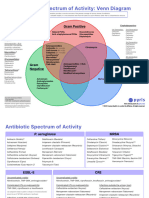
- Antibotics Venn DiagramDocument2 pagesAntibotics Venn DiagramTop VidsNo ratings yet
- Pharmacotherapy CasesDocument8 pagesPharmacotherapy CasesTop VidsNo ratings yet
- Chapter 146: Antimicrobial Prophylaxis in Surgery SELF-ASSESSMENT QUESTIONSDocument3 pagesChapter 146: Antimicrobial Prophylaxis in Surgery SELF-ASSESSMENT QUESTIONSTop VidsNo ratings yet
- Antiviral Agents - 2022Document113 pagesAntiviral Agents - 2022Top VidsNo ratings yet
- Reducing Med ErrorsDocument14 pagesReducing Med ErrorsTop VidsNo ratings yet
- Chapter 139: Urinary Tract Infections Self-Assessment QuestionsDocument4 pagesChapter 139: Urinary Tract Infections Self-Assessment QuestionsTop VidsNo ratings yet
- Chapter 48 - Antifungal Agents - Preclass MaterialsDocument14 pagesChapter 48 - Antifungal Agents - Preclass MaterialsTop VidsNo ratings yet
- CH 141: Bone and Joint Infections Self-Assessment Question-AnswersDocument3 pagesCH 141: Bone and Joint Infections Self-Assessment Question-AnswersTop VidsNo ratings yet
- CH 142: Sepsis and Septic Shock ANSWERSDocument2 pagesCH 142: Sepsis and Septic Shock ANSWERSTop VidsNo ratings yet
- CH 136: GI Infections and Enterotoxigenic Poisonings SELF-ASSESSMENT QUESTIONSDocument4 pagesCH 136: GI Infections and Enterotoxigenic Poisonings SELF-ASSESSMENT QUESTIONSTop VidsNo ratings yet
- Cipla Product ListDocument33 pagesCipla Product ListSumit Singhania100% (2)
- 2022 - PINELLA Workbook - v08Document84 pages2022 - PINELLA Workbook - v08Ann FarstaNo ratings yet
- Gram Positive Cocci - Sem 1Document45 pagesGram Positive Cocci - Sem 1Charmaine Corpuz GranilNo ratings yet
- Chapter 14Document8 pagesChapter 14SamanthaNo ratings yet
- Chapter 28Document14 pagesChapter 28ram sunderNo ratings yet
- General QuestionDocument70 pagesGeneral QuestionMONFOLA100% (2)
- (Libribook - Com) Introduction To Clinical Infectious Diseases A Problem-Based Approach 1st EditionDocument465 pages(Libribook - Com) Introduction To Clinical Infectious Diseases A Problem-Based Approach 1st EditionDaoud IssaNo ratings yet
- Campaign To Prevent Antimicrobial Resistance: Clinicians Hold The Solution!Document63 pagesCampaign To Prevent Antimicrobial Resistance: Clinicians Hold The Solution!kashifbutty2k100% (1)
- Mfhpb21-Eng - Enumeration of Staphylococcus Aureus in FoodsDocument14 pagesMfhpb21-Eng - Enumeration of Staphylococcus Aureus in FoodsPedro Carrillo PeredoNo ratings yet
- Acute Osteomyelitis in Children - JurdingDocument25 pagesAcute Osteomyelitis in Children - JurdingTimoty MarioNo ratings yet
- Staphylococcus Aureus Mastitis:: Cause, Detection, and ControlDocument7 pagesStaphylococcus Aureus Mastitis:: Cause, Detection, and ControlBrenda KristNo ratings yet
- Estafilococo Aureus Patogenicidad. Virulencia 2021Document23 pagesEstafilococo Aureus Patogenicidad. Virulencia 2021Gabriela ChaconNo ratings yet
- Coconut Oil Offers Hope For Antibiotic Resistant GermsDocument5 pagesCoconut Oil Offers Hope For Antibiotic Resistant GermsLiza Y. EspinosaNo ratings yet
- An Infectious Disease of Skin MCQsDocument111 pagesAn Infectious Disease of Skin MCQsDr.Tawheed67% (6)
- Bacteriology Reviewer: Bacteria Important Notes Tests Aerobic Gram-Positive (+) CocciDocument18 pagesBacteriology Reviewer: Bacteria Important Notes Tests Aerobic Gram-Positive (+) CocciAJNo ratings yet
- UC San Diego: Independent Study ProjectsDocument21 pagesUC San Diego: Independent Study ProjectsSoha ShahidNo ratings yet
- 1 Prevalence and Antibiotic Susceptibility Pattern of Staphylococcus Aureus in A TertiaryDocument4 pages1 Prevalence and Antibiotic Susceptibility Pattern of Staphylococcus Aureus in A Tertiaryzia ul RahmanNo ratings yet
- Pyogenic Staphylococcal & Streptococcal InfectionsDocument24 pagesPyogenic Staphylococcal & Streptococcal InfectionsFY MicroNo ratings yet
- Aureus: Prepared By: Miss Sidra-tul-MuntahaDocument16 pagesAureus: Prepared By: Miss Sidra-tul-MuntahamuqaddasNo ratings yet
- Microbio Lec 5 - StaphylococcusDocument6 pagesMicrobio Lec 5 - Staphylococcusapi-3743217100% (2)
- ChromagarDocument2 pagesChromagarapi-26429188No ratings yet
- MRSA What To KnowDocument3 pagesMRSA What To KnowFara LeeNo ratings yet
- Gram Positive Cocci Sem 1 1Document45 pagesGram Positive Cocci Sem 1 1Charmaine Corpuz Granil100% (1)
- General Information About MRSADocument4 pagesGeneral Information About MRSATati MaryatiNo ratings yet
- Prisma Health Adult Antimicrobial Guidebook 2021Document52 pagesPrisma Health Adult Antimicrobial Guidebook 2021JhNo ratings yet
- Staph Food PoisiningDocument14 pagesStaph Food PoisiningaishaNo ratings yet
- Clinical Presentation and Treatment of Orthopaedic Implant-Associated InfectionDocument9 pagesClinical Presentation and Treatment of Orthopaedic Implant-Associated InfectionSergio Martínez AlaínezNo ratings yet
- Darmstadt 1994Document15 pagesDarmstadt 1994rismahNo ratings yet
- Genul StaphylococcusDocument28 pagesGenul StaphylococcusAna Maria RusuNo ratings yet
- Antibiotic Resistance: Microbiology: A Clinical Approach © Garland ScienceDocument40 pagesAntibiotic Resistance: Microbiology: A Clinical Approach © Garland ScienceAnonymous Ra09vhgLNo ratings yet