You might also like
- Liver Disease in 30-Year-Old FarmerDocument5 pagesLiver Disease in 30-Year-Old FarmerKanwaljeet SinghNo ratings yet
- Right Iliac Fossa Mass in 56-Year-Old MaleDocument32 pagesRight Iliac Fossa Mass in 56-Year-Old Malemerin martinNo ratings yet
- Alcoholic Liver DiseaseDocument21 pagesAlcoholic Liver DiseaseInsta GrammerNo ratings yet
- Case CA StomachDocument23 pagesCase CA StomachBrutus AntonyNo ratings yet
- RIF MASSDocument25 pagesRIF MASSJeff LuwangNo ratings yet
- Obstructive JaundiceDocument21 pagesObstructive JaundicesnehaNo ratings yet
- Case Presentation Hernia 1 PDFDocument21 pagesCase Presentation Hernia 1 PDFMvs ramuNo ratings yet
- Epigastric Lump: by Dr. S Tejaswi, Second Year PG Dept of General SurgeryDocument30 pagesEpigastric Lump: by Dr. S Tejaswi, Second Year PG Dept of General SurgerymahalakshmiNo ratings yet
- Respiratory System CaseDocument7 pagesRespiratory System CaseKanwaljeet SinghNo ratings yet
- CA Stomach 1Document23 pagesCA Stomach 1Ticky TomNo ratings yet
- Clinical Case PresentationDocument13 pagesClinical Case PresentationSomanath KembhaviNo ratings yet
- Breast CA 094222Document26 pagesBreast CA 09422214-BALACHANDAR. R.PNo ratings yet
- CP 9Document47 pagesCP 9Mituran IshwarNo ratings yet
- Hernia CaseDocument16 pagesHernia Casebenak shivalingappaNo ratings yet
- Abdominal Swelling Case ReportDocument14 pagesAbdominal Swelling Case ReportLana LocoNo ratings yet
- Case PresentationDocument34 pagesCase PresentationAmninder KaurNo ratings yet
- Obstructive Jaundice: DR Anupam Lahiri Central Hospital, South Eastern Railway, Garden ReachDocument19 pagesObstructive Jaundice: DR Anupam Lahiri Central Hospital, South Eastern Railway, Garden Reachahmed arafaNo ratings yet
- Clinical Case PresentationDocument20 pagesClinical Case PresentationParvathi V KNo ratings yet
- Goo Case PresentationDocument23 pagesGoo Case PresentationsnehaNo ratings yet
- Case Report: Congestive Heart Failure FC III + Nonvalvular Atrial Fibrillation-Normo Ventricular ResponDocument21 pagesCase Report: Congestive Heart Failure FC III + Nonvalvular Atrial Fibrillation-Normo Ventricular ResponKarolus KetarenNo ratings yet
- Medicine Case Discussion: Roll Nos. - 106-P. Kavitha 107 - Padma Angmo 109 - Pinki Dubey 117 - Prannya AroraDocument25 pagesMedicine Case Discussion: Roll Nos. - 106-P. Kavitha 107 - Padma Angmo 109 - Pinki Dubey 117 - Prannya AroraAnagha M NairNo ratings yet
- Short Case-StnDocument26 pagesShort Case-StnSagarRathodNo ratings yet
- Case Presentation: Presented byDocument34 pagesCase Presentation: Presented byZahid AnwarNo ratings yet
- CASE PRESENTATION ON MULTINODULAR GOITREDocument23 pagesCASE PRESENTATION ON MULTINODULAR GOITREVishnuPriyaDikkalaNo ratings yet
- Diploma in Medical and Health Science Case ClerkingDocument11 pagesDiploma in Medical and Health Science Case ClerkingWan AmeeramirulzamanNo ratings yet
- Medicine Case Discussion: - Roll No - 202 - 205 - 208Document30 pagesMedicine Case Discussion: - Roll No - 202 - 205 - 208Anagha M NairNo ratings yet
- Wa0000Document25 pagesWa0000Nadia IndriNo ratings yet
- CP 2 VickyDocument45 pagesCP 2 Vickyanis amiraNo ratings yet
- Grand RoundDocument81 pagesGrand RoundMustofa HusainNo ratings yet
- CKD ExaminationDocument8 pagesCKD Examinationvenkatesh chowdaryNo ratings yet
- Subitcha T S - Case of Thyroid SwellingDocument26 pagesSubitcha T S - Case of Thyroid SwellingsnehaNo ratings yet
- Case Presentation: Lump Right HypochondriumDocument22 pagesCase Presentation: Lump Right HypochondriumNANDAN RAINo ratings yet
- Case Presentation: Paediatrics: by Tapan Jyoti Saikia 8 Sem Gauhati Medical CollegeDocument22 pagesCase Presentation: Paediatrics: by Tapan Jyoti Saikia 8 Sem Gauhati Medical CollegeArpit Mehta100% (1)
- AmoebaDocument24 pagesAmoebaJameh RomancapNo ratings yet
- Hernia Surgery Presentation1Document32 pagesHernia Surgery Presentation1Siddiqur Rahman AkashNo ratings yet
- Case of KMDocument28 pagesCase of KMPatty ReyesNo ratings yet
- Upper GI BleedingDocument70 pagesUpper GI BleedingMia MusNo ratings yet
- CASE PRESENTATION On Respiratory MedicineDocument34 pagesCASE PRESENTATION On Respiratory MedicineTanoy BoseNo ratings yet
- Case Presentation UrologyDocument30 pagesCase Presentation UrologypreciousNo ratings yet
- CVS Ie and MRDocument28 pagesCVS Ie and MRShilpi SarkarNo ratings yet
- Case PresentationDocument22 pagesCase PresentationBharathbushan V MandiriNo ratings yet
- Case Presentation BronchiectasisDocument61 pagesCase Presentation BronchiectasisUzair Muhd100% (6)
- MCC - CLDDocument27 pagesMCC - CLDAnagha M NairNo ratings yet
- Anaesthetic Management of Lumber PivdDocument21 pagesAnaesthetic Management of Lumber PivdSadasiv PandaNo ratings yet
- CopdDocument20 pagesCopdDhanesh B MNo ratings yet
- Case Report of Thyroid Toxic NoduleDocument17 pagesCase Report of Thyroid Toxic NoduleMatthias WollfNo ratings yet
- Clinical Case Discussion on Acute Cerebrovascular DiseaseDocument40 pagesClinical Case Discussion on Acute Cerebrovascular DiseaseRaghunandan RamanathanNo ratings yet
- University of Medicine (1) Yangon Community Medicine ProgramDocument31 pagesUniversity of Medicine (1) Yangon Community Medicine ProgramThuta128No ratings yet
- Case Report, General SurgeryDocument36 pagesCase Report, General Surgeryalnoooor38No ratings yet
- Examination of Parotid SwelllingDocument4 pagesExamination of Parotid SwelllingManas RanjanNo ratings yet
- AnemiaDocument62 pagesAnemiaKay Ramos JimenoNo ratings yet
- Case:chronic Constrictive Pericarditis - NicvdDocument44 pagesCase:chronic Constrictive Pericarditis - NicvdNavojit ChowdhuryNo ratings yet
- Acute PancreatitisDocument39 pagesAcute PancreatitisGENERAL sharpNo ratings yet
- Inguinal HerniaDocument57 pagesInguinal HerniaIsfahan ⎝⏠⏝⏠⎠No ratings yet
- Presentation Vericose .PPTX f.pptx2-1Document21 pagesPresentation Vericose .PPTX f.pptx2-1ArtiNo ratings yet
- Progressive Muscle Wasting in a 22-Year Old FemaleDocument25 pagesProgressive Muscle Wasting in a 22-Year Old FemaleTamzid Rabby TanmoyNo ratings yet
- Wa0003.Document21 pagesWa0003.merin martinNo ratings yet
- Case 8-1Document20 pagesCase 8-1NarendraNo ratings yet
- Case Summary For EmfDocument19 pagesCase Summary For EmfStella CooKeyNo ratings yet
- Lap Chole and HTN Long CaseDocument18 pagesLap Chole and HTN Long CaseDr.Biswajit jenaNo ratings yet
- Hernia and HydrocoeleDocument3 pagesHernia and HydrocoeleDr.Biswajit jenaNo ratings yet
- Review of Literature on Vasopressors for Cesarean SectionDocument10 pagesReview of Literature on Vasopressors for Cesarean SectionDr.Biswajit jenaNo ratings yet
- Spine Anatomy ExplainedDocument3 pagesSpine Anatomy ExplainedDr.Biswajit jenaNo ratings yet
- 6 Aim and ObjectivesDocument1 page6 Aim and ObjectivesDr.Biswajit jenaNo ratings yet
- Continous Non-Invasive Blood Pressure Monitoring (Clearsight System) - AADocument7 pagesContinous Non-Invasive Blood Pressure Monitoring (Clearsight System) - AADr.Biswajit jenaNo ratings yet
- Ea (Dyn)Document9 pagesEa (Dyn)Dr.Biswajit jenaNo ratings yet
- Echocardiography in Hemodynamic MonitoringDocument5 pagesEchocardiography in Hemodynamic MonitoringDr.Biswajit jenaNo ratings yet
- Advanced Hemodynamic Monitoring With Swan GanzDocument1 pageAdvanced Hemodynamic Monitoring With Swan GanzDr.Biswajit jenaNo ratings yet
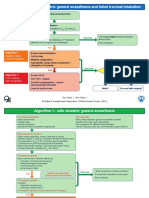
- 01 15 DAS Algorithms Web PRINT20092015Document6 pages01 15 DAS Algorithms Web PRINT20092015Sanj.etcNo ratings yet
- Minmally Invasive Cardiac Output MonitoringDocument6 pagesMinmally Invasive Cardiac Output MonitoringDr.Biswajit jenaNo ratings yet
- HDM 151022Document2 pagesHDM 151022Dr.Biswajit jenaNo ratings yet
- Properties and Uses of Common Inhalational AnaestheticsDocument56 pagesProperties and Uses of Common Inhalational AnaestheticsDr.Biswajit jenaNo ratings yet
- Anticholinergic Drugs: Mechanisms and Clinical UsesDocument39 pagesAnticholinergic Drugs: Mechanisms and Clinical UsesDr.Biswajit jenaNo ratings yet
- 00 Anticipation of Hypotension PAPERDocument18 pages00 Anticipation of Hypotension PAPERDr.Biswajit jenaNo ratings yet
- Anesthetic Management For Laparoscopic Cholecystectomy: Somchai AmornyotinDocument10 pagesAnesthetic Management For Laparoscopic Cholecystectomy: Somchai AmornyotinAidaDesNo ratings yet
- 2016 The Measurement of Adult Blood Pressure and Management of Hypertension Before Elective SurgeryDocument15 pages2016 The Measurement of Adult Blood Pressure and Management of Hypertension Before Elective SurgeryDr.Biswajit jenaNo ratings yet
- 2016 Current Recommendations On Adult Resuscitation BJADocument6 pages2016 Current Recommendations On Adult Resuscitation BJADr.Biswajit jenaNo ratings yet
- N 509 MaterialsDocument128 pagesN 509 MaterialsgdomagasNo ratings yet
- Discharge PlanDocument2 pagesDischarge PlanHannah ChiuNo ratings yet
- Arthritis OsteoarthritisDocument43 pagesArthritis OsteoarthritisMYMANo ratings yet
- Nuclear Medicine Therapy: Side Effects and Complications Luca GiovanellaDocument124 pagesNuclear Medicine Therapy: Side Effects and Complications Luca GiovanellaWhite HeartNo ratings yet
- Week1 - NAILCARE (Sek)Document2 pagesWeek1 - NAILCARE (Sek)rhyzeneNo ratings yet
- Physical Fitness Physical FitnessDocument18 pagesPhysical Fitness Physical FitnessCharmaine JanorasNo ratings yet
- Experimental and Correlational Studies of The Fear of Death: Direct Inethdds. The Earliest TechniqueDocument10 pagesExperimental and Correlational Studies of The Fear of Death: Direct Inethdds. The Earliest TechniqueDana PascuNo ratings yet
- Current Prospects of Social Work in India ArticleDocument9 pagesCurrent Prospects of Social Work in India Articlepuneeth87No ratings yet
- Audit of Delivery of Treatment Services For Children With AutismDocument72 pagesAudit of Delivery of Treatment Services For Children With AutismMichelle RindelsNo ratings yet
- Heavenly Spa MenuDocument2 pagesHeavenly Spa MenuDeTaaliNo ratings yet
- Guidelines For Case Classification For The National Birth Defects Prevention StudyDocument9 pagesGuidelines For Case Classification For The National Birth Defects Prevention Studyjorge davidNo ratings yet
- Vaccination Form (Sample)Document1 pageVaccination Form (Sample)Godfrey Loth Sales Alcansare Jr.No ratings yet
- The Psychology of Ageing - An Introduction, 3rd EdDocument320 pagesThe Psychology of Ageing - An Introduction, 3rd Edfauziahfasya123No ratings yet
- Modified Micro Marsupialization in Pediatric Patients: A Minimally Invasive TechniqueDocument4 pagesModified Micro Marsupialization in Pediatric Patients: A Minimally Invasive TechniquerinahpsNo ratings yet
- Case Presentation: Presenter: DR Amanda Lundah Date: 15/4/20Document25 pagesCase Presentation: Presenter: DR Amanda Lundah Date: 15/4/20King MazingaNo ratings yet
- Estate of Gerardo Gutierrez vs. PublixDocument12 pagesEstate of Gerardo Gutierrez vs. PublixPeterBurkeNo ratings yet
- Drug Metabolism-LectDocument35 pagesDrug Metabolism-LectFiona OyatsiNo ratings yet
- Emergency First Initial Assesment: Monday, October 05, 2020Document50 pagesEmergency First Initial Assesment: Monday, October 05, 2020Agoes TreeyantNo ratings yet
- Cardiac Marker Sem 5Document42 pagesCardiac Marker Sem 5novi pujiNo ratings yet
- Microbiologist: 3.1.5 Isolation & Gram StainingDocument5 pagesMicrobiologist: 3.1.5 Isolation & Gram Stainingapi-534896073No ratings yet
- MSDS Pro-Kleen 302Document8 pagesMSDS Pro-Kleen 302Wirdaniati EmiliaNo ratings yet
- DT Asa Bella-1Document12 pagesDT Asa Bella-1Bella Faradiska YuandaNo ratings yet
- Eat Yourself Smart: Britain Faces Airlift DeadlineDocument64 pagesEat Yourself Smart: Britain Faces Airlift DeadlineNidhi BhartiNo ratings yet
- Running Head: QSEN 1Document11 pagesRunning Head: QSEN 1Mariam AbedNo ratings yet
- Info - PathophysiologyDocument6 pagesInfo - PathophysiologyRupert BassigNo ratings yet
- CariesCare-International Consensus-Manuscript BDJ-corrected 12062019Document13 pagesCariesCare-International Consensus-Manuscript BDJ-corrected 12062019pocket4love4yeahNo ratings yet
- Jurnal Skripsi Anestesi 4Document8 pagesJurnal Skripsi Anestesi 4Tiara Anggun NurartoNo ratings yet
- OVPR FY20Q1 Proposal List PDFDocument45 pagesOVPR FY20Q1 Proposal List PDFtsuregiNo ratings yet
- Phlebotomy Essentials 7th EditionDocument61 pagesPhlebotomy Essentials 7th Editioneric.rodriguez669100% (44)
- Risk factors of diabetic retinopathy and vision threatening diabetic retinopathy and vision threatening diabetic retinopaty based on diabetic retinopathy screening program in greater bandung, west java.astriDocument14 pagesRisk factors of diabetic retinopathy and vision threatening diabetic retinopathy and vision threatening diabetic retinopaty based on diabetic retinopathy screening program in greater bandung, west java.astriSi PuputNo ratings yet