You might also like
- Financial Planning GodrejDocument199 pagesFinancial Planning GodrejriteshnaikNo ratings yet
- Basic Statistical Tools in Research and Data AnalysisDocument5 pagesBasic Statistical Tools in Research and Data AnalysisAira VillarinNo ratings yet
- Type 1 DiabetesDocument21 pagesType 1 Diabetesplogiojayr8340No ratings yet
- Kurdonia Structural Design ReportDocument341 pagesKurdonia Structural Design ReportAnonymous nQ9RqmNo ratings yet
- Diabetes Mellitus: Types, Causes, Symptoms, Complications, Diagnosis, Risk Factors and ManagementDocument39 pagesDiabetes Mellitus: Types, Causes, Symptoms, Complications, Diagnosis, Risk Factors and Managementimee cNo ratings yet
- The Pursuit of Happyness (Reaction Paper)Document2 pagesThe Pursuit of Happyness (Reaction Paper)ChavelleNo ratings yet
- Credit Management Overview and Principles of LendingDocument44 pagesCredit Management Overview and Principles of LendingTavneet Singh100% (2)
- 1888 For Almost DUMMIES - Robert J WielandDocument126 pages1888 For Almost DUMMIES - Robert J Wielandpropovednik100% (1)
- Case Study Presentation On Diabetic Foot UlcerDocument61 pagesCase Study Presentation On Diabetic Foot UlcerBindu GC100% (1)
- Managing Diabetes Through Proper Treatment and MonitoringDocument10 pagesManaging Diabetes Through Proper Treatment and Monitoringjoeln_9No ratings yet
- DIABETES MELLITUS Presentation (1) .PPTMDocument124 pagesDIABETES MELLITUS Presentation (1) .PPTMfrankNo ratings yet
- World History & Civilizations IIDocument8 pagesWorld History & Civilizations IIKosta GiakoumisNo ratings yet
- Error of DispensationalismDocument3 pagesError of DispensationalismJesus Lives100% (1)
- Diabetes and It's Oral ManifestationsDocument28 pagesDiabetes and It's Oral ManifestationsYashpreetsingh BhatiaNo ratings yet
- The Handbook of English For Specific Purposes: Edited by Brian Paltridge and Sue StarfieldDocument50 pagesThe Handbook of English For Specific Purposes: Edited by Brian Paltridge and Sue StarfieldEmiliano AcevedoNo ratings yet
- Assessment of Ear, Eye, Nose and ThroatDocument101 pagesAssessment of Ear, Eye, Nose and ThroatMuhammad100% (1)
- Health Assessment For Nusrses 1Document56 pagesHealth Assessment For Nusrses 1MuhammadNo ratings yet
- Diabetes MellitusDocument30 pagesDiabetes Mellitusurusha vaidyaNo ratings yet
- Baby Agnes Samuel NBU Care PlanDocument4 pagesBaby Agnes Samuel NBU Care PlanMuhammadNo ratings yet
- Baby Agnes Samuel NBU Care PlanDocument4 pagesBaby Agnes Samuel NBU Care PlanMuhammadNo ratings yet
- Paeda DMDocument38 pagesPaeda DMAmanuel LemiNo ratings yet
- Diabetes Mellitus: Prepared by Divya Bhusal B.SC - Nursing 3 YearDocument43 pagesDiabetes Mellitus: Prepared by Divya Bhusal B.SC - Nursing 3 YearSristi LamsalNo ratings yet
- Endocrine & Metabolic DisordersDocument38 pagesEndocrine & Metabolic DisordersBala UrmarNo ratings yet
- 12 Nursing Managment of Childern With Endocarine Disorders 2nd SemesterDocument27 pages12 Nursing Managment of Childern With Endocarine Disorders 2nd SemesterFaisal M.AlruwailiNo ratings yet
- Dental Management of Patients With Diabetes MellitusDocument8 pagesDental Management of Patients With Diabetes Mellitusاحمد سلامNo ratings yet
- Disorders of Carbohydrate and Lipid Metabolism-Converted - WatermarkDocument82 pagesDisorders of Carbohydrate and Lipid Metabolism-Converted - WatermarkAbhi VarnaNo ratings yet
- Hockenberry: Wong's Nursing Care of Infants and Children, 10th EditionDocument3 pagesHockenberry: Wong's Nursing Care of Infants and Children, 10th Editionshay gaindNo ratings yet
- Diabetes Mellitus Bahasa InggrisDocument16 pagesDiabetes Mellitus Bahasa InggrisyustikapupenNo ratings yet
- Diabetes Foot CheckDocument62 pagesDiabetes Foot CheckIosefina DudeanuNo ratings yet
- Common endocrinopathies: Diabetes, thyroid disorders, and congenital hypothyroidismDocument50 pagesCommon endocrinopathies: Diabetes, thyroid disorders, and congenital hypothyroidismHamza AliNo ratings yet
- Quiz Blessings #6Document7 pagesQuiz Blessings #6Rachel LiuNo ratings yet
- Diabetes Mellitus.U.iiDocument38 pagesDiabetes Mellitus.U.iitamtamtamtama0No ratings yet
- Diabetes MellitusDocument52 pagesDiabetes MellitusMervis masatunyaNo ratings yet
- Type 1 DM, 485Document20 pagesType 1 DM, 485Ananth Sai BadetiNo ratings yet
- DM Reporting ZDocument52 pagesDM Reporting ZZsazsaNo ratings yet
- Bio Project On DiabetesDocument17 pagesBio Project On DiabetesNishant KumarNo ratings yet
- Diabetes Students Fall21Document59 pagesDiabetes Students Fall21Ismael SerunjogiNo ratings yet
- Diabetes-Cho 2023 3rd Yr.Document37 pagesDiabetes-Cho 2023 3rd Yr.abdulrahmanbelewa96No ratings yet
- Diabete Mellitus HandoutsDocument7 pagesDiabete Mellitus HandoutsSittie Nashieva A. UsmanNo ratings yet
- Hypoglycemia in NewbornDocument10 pagesHypoglycemia in Newbornmaxim tomuNo ratings yet
- Diabetes Mellitus: Appled MedicineDocument8 pagesDiabetes Mellitus: Appled MedicinesabaamjadNo ratings yet
- Diabetes Mellitus: A Chronic Disease of Glucose MetabolismDocument69 pagesDiabetes Mellitus: A Chronic Disease of Glucose MetabolismKirstin del CarmenNo ratings yet
- Case Study: Diabetes Mellitus Type 2Document48 pagesCase Study: Diabetes Mellitus Type 2John Carlo GarciaNo ratings yet
- CARBOHYDRATE METABOLISM AND DISORDERS (Herbal Med)Document44 pagesCARBOHYDRATE METABOLISM AND DISORDERS (Herbal Med)AhjNo ratings yet
- DiabetesDocument35 pagesDiabetesyutisharma17No ratings yet
- Diabetes Lecture Spring 2018-2Document101 pagesDiabetes Lecture Spring 2018-2Cruz YrNo ratings yet
- Diabetes IDocument7 pagesDiabetes IRanier Sebastian CaparidaNo ratings yet
- The Endocrine System & Its DisturbancesDocument94 pagesThe Endocrine System & Its DisturbancesKarlou BorjaNo ratings yet
- Diabetes NotesDocument10 pagesDiabetes Notestripj33No ratings yet
- DM FinalDocument58 pagesDM FinalMalueth AnguiNo ratings yet
- Neonatal HypoglyDocument31 pagesNeonatal HypoglyAli FalihNo ratings yet
- DM Type 1 PDFDocument19 pagesDM Type 1 PDFesmana joelNo ratings yet
- Diabetes Mellitus - slidesDocument28 pagesDiabetes Mellitus - slidesReem ShamasNo ratings yet
- Nephrotic Syndrome: Prepared By: Manisha Praharaj Msc. Nursing 2Nd YearDocument28 pagesNephrotic Syndrome: Prepared By: Manisha Praharaj Msc. Nursing 2Nd YearMaria YaseenNo ratings yet
- Diabetes MellitusDocument17 pagesDiabetes MellitusRuqayya KobatteNo ratings yet
- 1.CHAPTER 1 What Is DiabetesDocument7 pages1.CHAPTER 1 What Is DiabetesGautam ManoharNo ratings yet
- DIABETES MELITUS GROUP PROJECTDocument10 pagesDIABETES MELITUS GROUP PROJECTahmad rizalNo ratings yet
- National University-Sudan Faculty of Pharmacy Diabetes Mellitus LectureDocument52 pagesNational University-Sudan Faculty of Pharmacy Diabetes Mellitus LectureMohammed KamalNo ratings yet
- 1 5 4 Diabetes Mellitus - PDF 2Document6 pages1 5 4 Diabetes Mellitus - PDF 2Maica LectanaNo ratings yet
- DiabetesDocument32 pagesDiabetesaneeshajaiswalNo ratings yet
- Endo - DMDocument24 pagesEndo - DMdoctorrfarrukhNo ratings yet
- Type 1 Diabetes Mellitus Nael HernandezDocument15 pagesType 1 Diabetes Mellitus Nael HernandezShermayne Mallapre HernandezNo ratings yet
- DMDocument76 pagesDMrose ann ayala100% (1)
- Diabetes Mellitus NewDocument97 pagesDiabetes Mellitus NewTMC PGI GENER MICKONo ratings yet
- Common Endocrine Disorders: Iril I. Panes, RN, MANDocument63 pagesCommon Endocrine Disorders: Iril I. Panes, RN, MANJona Phie Domingo MonteroNo ratings yet
- Complications (Acute)Document32 pagesComplications (Acute)Shwetal ShindeNo ratings yet
- Abnormal Blood Glucose LevelDocument23 pagesAbnormal Blood Glucose LevelAyush BhattNo ratings yet
- Metabolic DiseasesDocument35 pagesMetabolic DiseasesSOFIA YVONNE ZANONo ratings yet
- 222 Diabetes 2Document61 pages222 Diabetes 2Rahman Md.MoshiurNo ratings yet
- DM Presentation NewDocument44 pagesDM Presentation NewKipz JonsNo ratings yet
- Breaking the Chains of Diabetes. A Comprehensive Guide to Understanding and Managing Diabetes NaturallyFrom EverandBreaking the Chains of Diabetes. A Comprehensive Guide to Understanding and Managing Diabetes NaturallyNo ratings yet
- Ultimate Diet Plan for Diabetic Patients: Revolutionizing Diabetic NutritionFrom EverandUltimate Diet Plan for Diabetic Patients: Revolutionizing Diabetic NutritionNo ratings yet
- Introduction To DemographyDocument41 pagesIntroduction To DemographyMuhammadNo ratings yet
- Community Health-1Document52 pagesCommunity Health-1MuhammadNo ratings yet
- Assessing The Community's HealthDocument13 pagesAssessing The Community's HealthMuhammadNo ratings yet
- Gynaecology Assignment: Group 7Document32 pagesGynaecology Assignment: Group 7MuhammadNo ratings yet
- Bradhill Criteria of CausationDocument25 pagesBradhill Criteria of CausationMuhammadNo ratings yet
- Faraj Medical Case Study Mksl5 1Document30 pagesFaraj Medical Case Study Mksl5 1MuhammadNo ratings yet
- Indicators of HealthDocument62 pagesIndicators of HealthMuhammadNo ratings yet
- Epidemiology OverviewDocument4 pagesEpidemiology OverviewMuhammadNo ratings yet
- Types of Epidemiological StudiesDocument15 pagesTypes of Epidemiological StudiesMuhammadNo ratings yet
- CUSHING'S SYNDR-WPS OfficeDocument8 pagesCUSHING'S SYNDR-WPS OfficeMuhammadNo ratings yet
- Growth Hormone DeficiencyDocument1 pageGrowth Hormone DeficiencyMuhammadNo ratings yet
- Chest Examination: TechniqueDocument7 pagesChest Examination: TechniqueMuhammadNo ratings yet
- Conducting System of The HeartDocument27 pagesConducting System of The HeartMuhammadNo ratings yet
- Lect. 3 Adaptive ImmunityDocument8 pagesLect. 3 Adaptive ImmunityMuhammadNo ratings yet
- Understanding Hypersensitivity ReactionsDocument42 pagesUnderstanding Hypersensitivity ReactionsMuhammadNo ratings yet
- Lect. 10 ImmunodeficiencyDocument16 pagesLect. 10 ImmunodeficiencyMuhammadNo ratings yet
- Immunology Lecture6Antigen-Antibody ReactionsDocument15 pagesImmunology Lecture6Antigen-Antibody ReactionsVenkata Ramana Murthy VasupilliNo ratings yet
- Lect. 9 AutoimmunityDocument42 pagesLect. 9 AutoimmunityMuhammadNo ratings yet
- Lect. 6 ImmunoglobulinsDocument9 pagesLect. 6 ImmunoglobulinsMuhammadNo ratings yet
- The Complement Proteins and Their ReceptorsDocument15 pagesThe Complement Proteins and Their ReceptorsMuhammadNo ratings yet
- Discuss Nucleic AcidsDocument4 pagesDiscuss Nucleic AcidsMuhammadNo ratings yet
- Lect. 2 Innate Immunity FinalDocument47 pagesLect. 2 Innate Immunity FinalMuhammadNo ratings yet
- Nuru 115Document42 pagesNuru 115MuhammadNo ratings yet
- Nuru 115Document42 pagesNuru 115MuhammadNo ratings yet
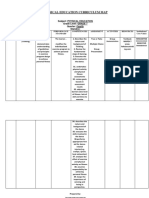
- Physical Education Curriculum MapDocument20 pagesPhysical Education Curriculum MapdyonaraNo ratings yet
- Quotation # SO2021/1274870: Quotation Date: Expiration: SalespersonDocument1 pageQuotation # SO2021/1274870: Quotation Date: Expiration: SalespersonAbdul WadoodNo ratings yet
- Bloock Diagram Reduction SummaryDocument10 pagesBloock Diagram Reduction SummaryLakshay KhichiNo ratings yet
- Communicating in Teams and OrganizationsDocument6 pagesCommunicating in Teams and Organizationserielle mejicoNo ratings yet
- Employee Satisfaction Analysis and InterpretationDocument29 pagesEmployee Satisfaction Analysis and InterpretationkhayyumNo ratings yet
- Adverb Exercise AnswerDocument3 pagesAdverb Exercise AnswerNatalia ErvinaNo ratings yet
- Brain-Ring "What? Where? When?"Document4 pagesBrain-Ring "What? Where? When?"Оксана ГорькаяNo ratings yet
- Travelling Sexualities: Wong Kar-Wai's Happy TogetherDocument27 pagesTravelling Sexualities: Wong Kar-Wai's Happy TogetherXi LINo ratings yet
- A Enm 201401692Document6 pagesA Enm 201401692Bhabani Sankar SwainNo ratings yet
- Principles and Stategies in Teaching MathDocument35 pagesPrinciples and Stategies in Teaching MathGeraldine RamosNo ratings yet
- Unit 8A and 8B Revision QuestionsDocument16 pagesUnit 8A and 8B Revision QuestionsAmgad AllamNo ratings yet
- Nmat Test Result-1017051213Document1 pageNmat Test Result-1017051213Dushyant SarvaiyaNo ratings yet
- Two Contributions To The Foundations of Set TheoryDocument9 pagesTwo Contributions To The Foundations of Set TheoryDietethiqueNo ratings yet
- Moyen Et Al., 2003, JSGDocument21 pagesMoyen Et Al., 2003, JSGambika senNo ratings yet
- Case Nizar SummaryDocument3 pagesCase Nizar SummaryShahera Zainudin100% (1)
- History of Anglo Saxon Literature English Assignment NUML National University of Modern LanguagesDocument15 pagesHistory of Anglo Saxon Literature English Assignment NUML National University of Modern LanguagesMaanNo ratings yet
- Use of Imagery in Look Back in AngerDocument3 pagesUse of Imagery in Look Back in AngerArindam SenNo ratings yet
- PBA4806 Exam Answer SheetDocument11 pagesPBA4806 Exam Answer SheetPhindile HNo ratings yet
- The Effect of 5S On Employee Performance: An Empirical Study Among Lebanese HospitalsDocument7 pagesThe Effect of 5S On Employee Performance: An Empirical Study Among Lebanese HospitalsMuthu BaskaranNo ratings yet
- Labor 2 CasesDocument77 pagesLabor 2 CasesMercado MarloNo ratings yet
- Sorting Lesson PlanDocument4 pagesSorting Lesson PlanStasha DuttNo ratings yet