You might also like
- NRPH BreastfeedingDocument8 pagesNRPH BreastfeedingDaphne PearlNo ratings yet
- Physiology of LactationDocument18 pagesPhysiology of LactationPreeti Sawant100% (2)
- Chap 4 Lactation and Human Milk Part 1Document12 pagesChap 4 Lactation and Human Milk Part 1Fetria MelaniNo ratings yet
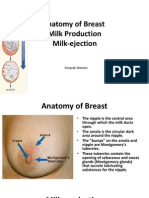
- Anatomy of Breast, Milk Production, and Milk-EjectionDocument23 pagesAnatomy of Breast, Milk Production, and Milk-EjectionDeepak Ghimire100% (2)
- Clinical Obstetrics/Gynecology Review 2023: For USMLE Step 2 CK and COMLEX-USA Level 2From EverandClinical Obstetrics/Gynecology Review 2023: For USMLE Step 2 CK and COMLEX-USA Level 2Rating: 4 out of 5 stars4/5 (1)
- HyperthyroidismDocument18 pagesHyperthyroidismWahyuni FatmonaNo ratings yet
- Polycystic Ovary Syndrome: Dr. Gurpreet KaurDocument57 pagesPolycystic Ovary Syndrome: Dr. Gurpreet KaurPiyush Agarwal100% (1)
- Physiology of LactationDocument3 pagesPhysiology of LactationAswathy Chandran100% (1)
- Physiology of Breast Milk ProductionDocument17 pagesPhysiology of Breast Milk ProductionOlivia TegliaNo ratings yet
- U9W6 - Physiology of LactationDocument2 pagesU9W6 - Physiology of LactationSuh KhaNo ratings yet
- Chapter 3 Lactation NewDocument15 pagesChapter 3 Lactation NewJassyNo ratings yet
- Breastfeeding: Grup 1 NameDocument13 pagesBreastfeeding: Grup 1 NameAnnisaDpsNo ratings yet
- Breast and LactationDocument27 pagesBreast and Lactationgugus aminaNo ratings yet
- 132 16SCCND4 2020051908100864Document81 pages132 16SCCND4 2020051908100864manjuskkNo ratings yet
- LactationDocument9 pagesLactationLithiya JoseNo ratings yet
- LactationDocument8 pagesLactationDevuchandana RNo ratings yet
- Basic Knowledge of LactationDocument27 pagesBasic Knowledge of Lactationedward_chiNo ratings yet
- Physiology of Lactation and PurpuriumDocument37 pagesPhysiology of Lactation and Purpuriumvarshasharma05No ratings yet
- Physiology of Lactation 2023Document34 pagesPhysiology of Lactation 2023liu goedy fernadezNo ratings yet
- Physiology of Breast MilkDocument6 pagesPhysiology of Breast Milkrix07No ratings yet
- Physiological Breast Development and Involution - CompressedDocument7 pagesPhysiological Breast Development and Involution - CompressedmohamedhazemelfollNo ratings yet
- Physiology of Lactation NewDocument28 pagesPhysiology of Lactation NewLala SumatraNo ratings yet
- Structure of The Lactating Breast: Lactation Is The Process by Which Milk Is Synthesized and Secreted From The MammaryDocument5 pagesStructure of The Lactating Breast: Lactation Is The Process by Which Milk Is Synthesized and Secreted From The Mammaryratna putriNo ratings yet
- Medical, Lactation, MastitisDocument46 pagesMedical, Lactation, Mastitishiteshwar9999No ratings yet
- Physiology of Milk ProductionDocument22 pagesPhysiology of Milk ProductionRajeev NepalNo ratings yet
- Mammae (Payudara) : LactationDocument13 pagesMammae (Payudara) : LactationAde ElvinaNo ratings yet
- Concepts of LactationDocument26 pagesConcepts of LactationKeerthi AnbazhaganNo ratings yet
- Human Reproduction-L12 - May 16.pdf 2.oDocument69 pagesHuman Reproduction-L12 - May 16.pdf 2.oUpal PramanickNo ratings yet
- Physiology of LactationDocument29 pagesPhysiology of Lactationcorzpun16867879% (14)
- Physiology of Lactation: Prepared By: Fy MSC NursingDocument32 pagesPhysiology of Lactation: Prepared By: Fy MSC NursingSùjâl PätídàrNo ratings yet
- Roles of HormonesDocument13 pagesRoles of Hormoneshafizah_90100% (6)
- The Anatomy, Physiology and Philosophy of Breastfeeding: Hiltrud Dawson, RN, BT, IBCLC 2008Document66 pagesThe Anatomy, Physiology and Philosophy of Breastfeeding: Hiltrud Dawson, RN, BT, IBCLC 2008ericNo ratings yet
- Basic Science NeonatalDocument114 pagesBasic Science NeonatalKAROMAHUL MALAYA JATINo ratings yet
- 02 Physiology of LactationDocument32 pages02 Physiology of Lactationabozizo063No ratings yet
- Anatomy and Physiology of The Breast: Mammary GlandsDocument10 pagesAnatomy and Physiology of The Breast: Mammary GlandsAlmira GamaoNo ratings yet
- Breast FeedingDocument5 pagesBreast FeedingClareen JuanicoNo ratings yet
- LactationDocument24 pagesLactationEric Mayo Dagradi KabatNo ratings yet
- Seminar Breast Feeding and BFH PDFDocument16 pagesSeminar Breast Feeding and BFH PDFDevuchandana R100% (3)
- Fertilization and Implantation Copy To StudentsDocument40 pagesFertilization and Implantation Copy To StudentsRiya SinghNo ratings yet
- Physiology of LactationDocument16 pagesPhysiology of LactationsabaNo ratings yet
- Breast FeedingDocument18 pagesBreast FeedingCabdullahi maxamed xussenNo ratings yet
- MCN Nursing 1Document107 pagesMCN Nursing 1Fau Fau DheoboNo ratings yet
- LACTATIONDocument4 pagesLACTATIONNlemorusa PaschalineNo ratings yet
- CHAPTER 3-LactationDocument12 pagesCHAPTER 3-LactationMaria Alexis Ahadain OlvidoNo ratings yet
- University of Agriculture, Abeokuta: Department of Animal Production & HealthDocument29 pagesUniversity of Agriculture, Abeokuta: Department of Animal Production & HealthransinghNo ratings yet
- The PuerperiumDocument42 pagesThe PuerperiumVenzNo ratings yet
- Clinical Teaching On Breast Feeding 3Document19 pagesClinical Teaching On Breast Feeding 3Devuchandana RNo ratings yet
- BreastfeedingDocument32 pagesBreastfeedingAhmed MadkourNo ratings yet
- Lactation by Syed MohsinDocument22 pagesLactation by Syed MohsinSyed Mohsin NisarNo ratings yet
- Anatomy and Physiology FinalDocument2 pagesAnatomy and Physiology FinalMary Anne Gagarin DomingoNo ratings yet
- Anatomy and Physiology of Female BreastDocument16 pagesAnatomy and Physiology of Female Breastsami loveNo ratings yet
- Breastfeeding and Nutritional Requirements in ChildrenDocument64 pagesBreastfeeding and Nutritional Requirements in Childrenapule geraldhumble100% (1)
- 4 Endocrine 6Document16 pages4 Endocrine 6ShenNo ratings yet
- Breastfeeding Lecture PowerpointDocument36 pagesBreastfeeding Lecture PowerpointMa. Isabel A. EnriquezNo ratings yet
- Anatomy and Physiology BreastDocument3 pagesAnatomy and Physiology BreastJames Daniel CodamonNo ratings yet
- Group 4 Parturation-And-LactationDocument35 pagesGroup 4 Parturation-And-LactationIgnacio FelicityNo ratings yet
- Breastfeeding 121023054344 Phpapp01Document36 pagesBreastfeeding 121023054344 Phpapp01Jose Miguel Granados GalvanNo ratings yet
- Breast Care and Breast Feeding For CI, by DR Abera Sept 2021Document57 pagesBreast Care and Breast Feeding For CI, by DR Abera Sept 2021Kerod AbebeNo ratings yet
- CamScanner 10-25-2023 10.15Document22 pagesCamScanner 10-25-2023 10.15Farhan JarifNo ratings yet
- Anatomia y Fisiologuia General Libro-1351-1400Document50 pagesAnatomia y Fisiologuia General Libro-1351-1400Felipe Aguirre CórdovaNo ratings yet
- Pregnancy, Parturition, Breastfeeding - Physiology For Medical StudentsDocument34 pagesPregnancy, Parturition, Breastfeeding - Physiology For Medical StudentsLamy SNo ratings yet
- "Nurturing Beginnings: A Comprehensive Guide to Breastfeeding Success"From Everand"Nurturing Beginnings: A Comprehensive Guide to Breastfeeding Success"No ratings yet
- WelcomeDocument106 pagesWelcomeDakshayini MbNo ratings yet
- Good Afternoon: Powerpoint TemplatesDocument58 pagesGood Afternoon: Powerpoint TemplatesDakshayini MbNo ratings yet
- UntitledDocument43 pagesUntitledDakshayini MbNo ratings yet
- Prelabour Rupture of The MembranesDocument22 pagesPrelabour Rupture of The MembranesDakshayini MbNo ratings yet
- Pre Eclampsia and EclampsiaDocument40 pagesPre Eclampsia and EclampsiaDakshayini MbNo ratings yet
- High Risk PregnancyDocument33 pagesHigh Risk PregnancyDakshayini MbNo ratings yet
- WelcomeDocument28 pagesWelcomeDakshayini MbNo ratings yet
- Patient Classification SystemDocument97 pagesPatient Classification SystemDakshayini MbNo ratings yet
- Induction AND Augmentation OF LabourDocument42 pagesInduction AND Augmentation OF LabourDakshayini MbNo ratings yet
- Ward ManagementDocument20 pagesWard ManagementDakshayini MbNo ratings yet
- Nursing Service AdministrationDocument25 pagesNursing Service AdministrationDakshayini MbNo ratings yet
- UntitledDocument19 pagesUntitledDakshayini MbNo ratings yet
- Performance AppraisalDocument22 pagesPerformance AppraisalDakshayini MbNo ratings yet
- Ramadan Guide For DiabetesDocument9 pagesRamadan Guide For DiabetesUjwal TickooNo ratings yet
- Endocrine Manifestations of Eating Disorders PDFDocument11 pagesEndocrine Manifestations of Eating Disorders PDFJaime GonzálezNo ratings yet
- Pcos QuizDocument12 pagesPcos QuizHimani VermaNo ratings yet
- Hirsutism: Diagnosis and TreatmentDocument6 pagesHirsutism: Diagnosis and TreatmentAnonymous ysrxggk21cNo ratings yet
- Male and Female HormonesDocument26 pagesMale and Female HormonesZuha HundalNo ratings yet
- Chap 5 Hormonal Response To ExerciseDocument53 pagesChap 5 Hormonal Response To ExerciseAnnie KhanNo ratings yet
- Thyroid Function TestDocument21 pagesThyroid Function TestPat JacintoNo ratings yet
- Overview of Biochemical EndocrinologyDocument20 pagesOverview of Biochemical EndocrinologyGauri KashyapNo ratings yet
- What Is Goitre?: Thyroid GlandDocument3 pagesWhat Is Goitre?: Thyroid Glandflex gyNo ratings yet
- Dapus FixDocument6 pagesDapus FixArdian Zaka RANo ratings yet
- Alsangedy Bullets For Paces Acromegaly 2nd EditionDocument2 pagesAlsangedy Bullets For Paces Acromegaly 2nd EditionGhulamMemonNo ratings yet
- Testing During Pregnancy: David G. Grenache, PHD University of Utah & Arup Laboratories Salt Lake City, UtDocument54 pagesTesting During Pregnancy: David G. Grenache, PHD University of Utah & Arup Laboratories Salt Lake City, Utمحمد عمران راناNo ratings yet
- An Essay On Congenital Adrenal Hyperplasia - MYP5Document3 pagesAn Essay On Congenital Adrenal Hyperplasia - MYP5Monica Paris SisourathNo ratings yet
- Menstrual DisordersDocument16 pagesMenstrual DisordersKamran khanNo ratings yet
- Dry Lab Exercise 4 EndocrineDocument4 pagesDry Lab Exercise 4 Endocrine06Fajrian RidhatunnisaNo ratings yet
- EBM - 5. Adrenal DisordersDocument101 pagesEBM - 5. Adrenal DisordersBRI KUNo ratings yet
- BSC 6 Sem General Mammalian Physiology 2 Zoology Summer 2018Document1 pageBSC 6 Sem General Mammalian Physiology 2 Zoology Summer 2018Ujjwala KumbhalkarNo ratings yet
- PhysioEx Exercise 4 Activity 2Document3 pagesPhysioEx Exercise 4 Activity 2Alesandra Campo SanmartínNo ratings yet
- Chapter 10 ANATOMY AND PHYSIOLOGYDocument5 pagesChapter 10 ANATOMY AND PHYSIOLOGYAngela Mae MeriñoNo ratings yet
- Endocrine System Prepared By: Prof. Mike Chavez RN, USRNDocument7 pagesEndocrine System Prepared By: Prof. Mike Chavez RN, USRNMeiJoyFlamianoIINo ratings yet
- Summary of Endocrine DisordersDocument2 pagesSummary of Endocrine DisordersKrysny MontebonNo ratings yet
- Introduction To Endocrinology For Clinical StudentsDocument28 pagesIntroduction To Endocrinology For Clinical StudentsOhwovoriole ToketemuNo ratings yet
- Tugas B.inggrisDocument5 pagesTugas B.inggrisFauziatul RiyadaNo ratings yet
- Anterior Pituitary HormonesDocument46 pagesAnterior Pituitary Hormonespramod bhaleraoNo ratings yet
- Panacea Biotec Launches - TENEPAN, A Cost Effective Product For The Treatment of Type 2 Diabetes Mellitus (T2DM) (Company Update)Document5 pagesPanacea Biotec Launches - TENEPAN, A Cost Effective Product For The Treatment of Type 2 Diabetes Mellitus (T2DM) (Company Update)Shyam SunderNo ratings yet
- Terona HarDocument3 pagesTerona HarIoana Maria DănilăNo ratings yet
- Ibn Sina Diagnostic & Imaging CenterDocument6 pagesIbn Sina Diagnostic & Imaging CenterSAHMIMNo ratings yet
- Endocrine EmergenciesDocument33 pagesEndocrine EmergenciesbetyahNo ratings yet