You might also like
- Reverse and Prevent Heart Disease: Natural Ways to Stop and Prevent Heart Disease, Using Plant-Based Oil-Free Diets (Cure Congestive Heart Failure)From EverandReverse and Prevent Heart Disease: Natural Ways to Stop and Prevent Heart Disease, Using Plant-Based Oil-Free Diets (Cure Congestive Heart Failure)No ratings yet
- Cardio-Vascular Disease: Ischemic Heart Disease: Atheroscelorsis, Angina, Myocardial InfarctionDocument64 pagesCardio-Vascular Disease: Ischemic Heart Disease: Atheroscelorsis, Angina, Myocardial InfarctionFarheen KhanNo ratings yet
- Ischemic Heart DiseaseDocument56 pagesIschemic Heart DiseaseSMART PHARMACY By BRIJESHNo ratings yet
- Medicine in Brief: Name the Disease in Haiku, Tanka and ArtFrom EverandMedicine in Brief: Name the Disease in Haiku, Tanka and ArtRating: 5 out of 5 stars5/5 (1)
- Ischemic Heart Disease (IHD)Document70 pagesIschemic Heart Disease (IHD)Deborah AnnNo ratings yet
- Acute Myocardial InfarctionDocument35 pagesAcute Myocardial Infarctionvirnzrobz80% (10)
- Myocardial Infarction. BPTDocument62 pagesMyocardial Infarction. BPTAanchal GuptaNo ratings yet
- Cardiovasculer Disorders 1Document77 pagesCardiovasculer Disorders 1SaraNo ratings yet
- ATHEROSCLEROSISDocument41 pagesATHEROSCLEROSISDoc On CallNo ratings yet
- Curs 9 Myocarditis CardiomyopathyDocument41 pagesCurs 9 Myocarditis CardiomyopathyIliescu DenisaNo ratings yet
- Peny. KardiovaskulerDocument99 pagesPeny. Kardiovaskulerpraptiningsih.90No ratings yet
- CHD, RHD, HypertensionDocument32 pagesCHD, RHD, Hypertensionkacytyne tablazonNo ratings yet
- Cagayan State University College of Medicine and Surgery SY: 2009-2010Document41 pagesCagayan State University College of Medicine and Surgery SY: 2009-2010ahmad usmanNo ratings yet
- HTN and CHFDocument29 pagesHTN and CHFkiflomNo ratings yet
- AtherosclerosisDocument41 pagesAtherosclerosisSachin KumarNo ratings yet
- Cardiovascular System Pathology, MBCHBDocument18 pagesCardiovascular System Pathology, MBCHBSecret AgentNo ratings yet
- CARDIOMYOPATHYDocument64 pagesCARDIOMYOPATHYgalemayehu471No ratings yet
- Acute Myocardial Infarction: Sarah Priore RN BSNDocument53 pagesAcute Myocardial Infarction: Sarah Priore RN BSNAngnaKalsiNo ratings yet
- Group 5 Report in Health: CardiovascularDocument22 pagesGroup 5 Report in Health: CardiovascularWinona Jasmin TamaresNo ratings yet
- Topic 1. Cardiovascular Emergencies: What Causes ItDocument6 pagesTopic 1. Cardiovascular Emergencies: What Causes ItJojo JustoNo ratings yet
- Learning Objectives in Cardiovascular DiseaseDocument13 pagesLearning Objectives in Cardiovascular DiseaseZul Azim AnuarNo ratings yet
- Myocardial InfarctionDocument16 pagesMyocardial Infarction211941103014No ratings yet
- Dilated Cardiomyopathy: DR Adekunle Victor O. Cardiology Unit Medicine Department Abuth Shika ZariaDocument26 pagesDilated Cardiomyopathy: DR Adekunle Victor O. Cardiology Unit Medicine Department Abuth Shika ZariaVictor AdekunleNo ratings yet
- CardiologyDocument613 pagesCardiologyyangi dokaNo ratings yet
- Congestive Heart FailureDocument47 pagesCongestive Heart FailureRajesh Sharma100% (1)
- Ischemic Heart DiseaseDocument47 pagesIschemic Heart DiseaseAbood SamoudiNo ratings yet
- Ischemic Heart DiseaseDocument116 pagesIschemic Heart DiseaseAndrew OrlovNo ratings yet
- Curs Bolile PericarduluiDocument85 pagesCurs Bolile PericarduluiAndreea ElenaNo ratings yet
- Cardio MyopathiesDocument39 pagesCardio Myopathiesinyanji.barasaNo ratings yet
- Group 3Document8 pagesGroup 3obrieNo ratings yet
- Project Based Learning 2 Year 2021 Title: Heart DiseasesDocument19 pagesProject Based Learning 2 Year 2021 Title: Heart DiseasesADAM BIN MUHIDIN MoeNo ratings yet
- CARDIOMYOPATHIESDocument46 pagesCARDIOMYOPATHIESStella CooKeyNo ratings yet
- Cardivascular Deseases and Diabetes MellitusDocument38 pagesCardivascular Deseases and Diabetes MellitusYu QingNo ratings yet
- Heart Failure and Pulmonary EdemaDocument60 pagesHeart Failure and Pulmonary EdemaYosra —No ratings yet
- Case Analysis:: Myocardial InfarctionDocument76 pagesCase Analysis:: Myocardial InfarctionIpeNo ratings yet
- Introduction To Vascular SurgeryDocument13 pagesIntroduction To Vascular Surgeryapi-3858544100% (1)
- Atherosclerosis 2 2017 (Modified)Document64 pagesAtherosclerosis 2 2017 (Modified)Remo B AbyNo ratings yet
- Pharmacotherapeutics AssignmentDocument14 pagesPharmacotherapeutics AssignmentKaneez ZehraNo ratings yet
- 03-Ischemic Heart Disease - 2020 OngoingDocument151 pages03-Ischemic Heart Disease - 2020 OngoingDana MohammadNo ratings yet
- AtherosclerosisDocument62 pagesAtherosclerosisMoush AbdiNo ratings yet
- Hypertension LectureDocument36 pagesHypertension Lectureaurora_dorisNo ratings yet
- CARDIOMYOPATHIESDocument80 pagesCARDIOMYOPATHIESNadun MethwadaneNo ratings yet
- HNI 310 - Cardiovascular System BB 2015Document59 pagesHNI 310 - Cardiovascular System BB 2015Mohammad Usman QureshiNo ratings yet
- 4 CardiomyopathyDocument54 pages4 CardiomyopathyDanny DesuNo ratings yet
- GeriatriDocument39 pagesGeriatriLisa ElfiraNo ratings yet
- Dilated CardiomyopathyDocument12 pagesDilated Cardiomyopathyelene nikoleishviliNo ratings yet
- Ischemic Heart Disease (IHD)Document55 pagesIschemic Heart Disease (IHD)rameshbmc100% (5)
- Sudden Unexpected Death FMT 400Document11 pagesSudden Unexpected Death FMT 400khadzxNo ratings yet
- Coronary Heart DiseaseDocument42 pagesCoronary Heart DiseaseMuhammad ShahzadNo ratings yet
- Coronary Artery Disease: By. Saiha AlinaDocument19 pagesCoronary Artery Disease: By. Saiha AlinasaihaNo ratings yet
- Acute Coronary SyndromeDocument30 pagesAcute Coronary SyndromeEndar EszterNo ratings yet
- Cardiovascular PathologyDocument182 pagesCardiovascular PathologyPavan chowdaryNo ratings yet
- SEMINARDocument31 pagesSEMINARDeveshNo ratings yet
- NSG 210 Study GuideDocument25 pagesNSG 210 Study GuideyasserNo ratings yet
- Inflammatory and Valvular DisordersDocument43 pagesInflammatory and Valvular DisordersRifqi Hary ZulfikarNo ratings yet
- Atherosclerosis and Myocardial InfractionDocument26 pagesAtherosclerosis and Myocardial InfractionElina GNo ratings yet
- Management of Patients With Coronary Vascular Disease Jeff SydioncoDocument25 pagesManagement of Patients With Coronary Vascular Disease Jeff SydioncoRoyce Vincent TizonNo ratings yet
- Cardiovascular Diseases: Presented By: Maliha Zulqarnain (31), Pernia Zuha (15), Maryam Rao (23), Minahil ZaheerDocument34 pagesCardiovascular Diseases: Presented By: Maliha Zulqarnain (31), Pernia Zuha (15), Maryam Rao (23), Minahil ZaheerTabeer fatimaNo ratings yet
- Ischaemic Heart Disease Mku 2020Document38 pagesIschaemic Heart Disease Mku 2020ElvisNo ratings yet
- Ecg Essentials 2 PDFDocument45 pagesEcg Essentials 2 PDFjaikishan marathe 69No ratings yet
- Tan. Injuries PDFDocument1 pageTan. Injuries PDFtanishk malviyaNo ratings yet
- ANS Skeletal Muscle AssignmentDocument4 pagesANS Skeletal Muscle AssignmentAkinsanya Oyinkansola ChristineNo ratings yet
- B22 Neural Mechanisms of Learning & MemoryDocument21 pagesB22 Neural Mechanisms of Learning & MemoryNilanjana Chatterjee ChakrabortyNo ratings yet
- Erste Hilfe Kurs AnglaisDocument7 pagesErste Hilfe Kurs AnglaisMed SîmöNo ratings yet
- 101 Modul Hebat Bio 2021 - PDF - Eng-65-70Document6 pages101 Modul Hebat Bio 2021 - PDF - Eng-65-70BF CLNo ratings yet
- The Circulatory System: (Parts and Functions) Prepared By: Wilfred D. ManingasDocument30 pagesThe Circulatory System: (Parts and Functions) Prepared By: Wilfred D. ManingasAngelica OlivarNo ratings yet
- Seminar On Bronchial Asthma NewDocument42 pagesSeminar On Bronchial Asthma NewShabna SameerNo ratings yet
- Cholinesterase Inhibitors - AlzheimersDocument1 pageCholinesterase Inhibitors - AlzheimerscpboilergirlNo ratings yet
- Detailed Lesson Plan in Science 5 1st QuarterDocument8 pagesDetailed Lesson Plan in Science 5 1st QuarterAndrewNo ratings yet
- StomaDocument10 pagesStomanozel77No ratings yet
- Blood Circulation and TransportDocument15 pagesBlood Circulation and Transportqas1727No ratings yet
- By Duy Thai, 1997: Pharmacology Semester 1 Page 1 of 4Document4 pagesBy Duy Thai, 1997: Pharmacology Semester 1 Page 1 of 4ravi2likeNo ratings yet
- The ESC Textbook of Sports CardiologyDocument478 pagesThe ESC Textbook of Sports CardiologyIBFiS100% (1)
- Brain Wash: David Perlmutter, MD, and Austin Perlmutter, MDDocument7 pagesBrain Wash: David Perlmutter, MD, and Austin Perlmutter, MDhanhdoc0% (1)
- Reverse Medical Terminology #2Document6 pagesReverse Medical Terminology #2Jessica CarterNo ratings yet
- ECG LectureDocument37 pagesECG LectureAmit Pannu100% (1)
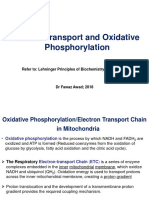
- Electron Transport and Oxidative Phosphorylation: Refer To: Lehninger Principles of Biochemistry (Chapter 19)Document43 pagesElectron Transport and Oxidative Phosphorylation: Refer To: Lehninger Principles of Biochemistry (Chapter 19)Yousef KhallafNo ratings yet
- Immune System by Asif PresentationDocument35 pagesImmune System by Asif PresentationHassan AsifNo ratings yet
- Health Benefits of Drinking WaterDocument1 pageHealth Benefits of Drinking WaterailynaNo ratings yet
- GENERAL BIOLOGY 2 Baby LabDocument10 pagesGENERAL BIOLOGY 2 Baby LabRK MendozaNo ratings yet
- Gas ExchangeDocument3 pagesGas ExchangeDemi Ruth ElenNo ratings yet
- 2020 - A Physiologic Approach To Hemodynamic Monitoring and Optimizing Oxygen Delivery in Shock ResuscitationDocument18 pages2020 - A Physiologic Approach To Hemodynamic Monitoring and Optimizing Oxygen Delivery in Shock ResuscitationAndre OliveiraNo ratings yet
- General AnesthesiaDocument7 pagesGeneral AnesthesiaPADAYON MEDISINANo ratings yet
- Shock NotesDocument4 pagesShock NotesKenneth UbaldeNo ratings yet
- Cardiogenic ShockDocument3 pagesCardiogenic ShockDiaz AlmayangNo ratings yet
- CJM SepsisDocument1 pageCJM Sepsisapi-688564858No ratings yet
- Biochemical Analysis of BloodDocument2 pagesBiochemical Analysis of Bloodbucsit100% (1)
- Spirometry Acceptability PosterDocument1 pageSpirometry Acceptability PosterMauricioDinizNo ratings yet
- Immediate Effect of Nadi Shodhana Pranayama On Blood Glucose, Heart Rate and Blood PressureDocument6 pagesImmediate Effect of Nadi Shodhana Pranayama On Blood Glucose, Heart Rate and Blood PressureDr. Manoranjan TripathyNo ratings yet