You might also like
- Care Bundle For Insertion and Maintenance of Central Venous Catheters Within The Renal and Transplant UnitDocument14 pagesCare Bundle For Insertion and Maintenance of Central Venous Catheters Within The Renal and Transplant Unitnavjav100% (1)
- ENHANZE® Drug Delivery Technology: Advancing Subcutaneous Drug Delivery using Recombinant Human Hyaluronidase PH20From EverandENHANZE® Drug Delivery Technology: Advancing Subcutaneous Drug Delivery using Recombinant Human Hyaluronidase PH20No ratings yet
- Case Scenario Evidence Based PracticeDocument3 pagesCase Scenario Evidence Based PracticeAdrienne Nicole PaneloNo ratings yet
- IV Catheter Insertion PDFDocument17 pagesIV Catheter Insertion PDFHannaNo ratings yet
- Case Scenario Evidence Base PracticeDocument4 pagesCase Scenario Evidence Base Practicemaria khalifaNo ratings yet
- Evidence Based PracticeDocument4 pagesEvidence Based PracticeMark EniegoNo ratings yet
- Jurnal Pengambilan Darah Vena PDFDocument10 pagesJurnal Pengambilan Darah Vena PDFfebriyankusumoningrum100% (1)
- Vap Care Bundle FinalDocument4 pagesVap Care Bundle FinalMother of Mercy Hospital -Tacloban Inc.No ratings yet
- Nonoperating Room Anesthesia Anesthesia in The Gastrointestinal SuiteDocument16 pagesNonoperating Room Anesthesia Anesthesia in The Gastrointestinal SuiteGustavo ParedesNo ratings yet
- Clinical Procedures For Safer Patient Care: Chapter 8. Intravenous TherapyDocument54 pagesClinical Procedures For Safer Patient Care: Chapter 8. Intravenous TherapyGladys YaresNo ratings yet
- Nursing Skill Iv InsertionDocument8 pagesNursing Skill Iv InsertionSabrina TolentinoNo ratings yet
- Procedure-Central Venous Access Catheter InsertionDocument18 pagesProcedure-Central Venous Access Catheter Insertionmohamad dildarNo ratings yet
- Quality Control in Endoscopy Unit: Safety Considerations For The PatientDocument13 pagesQuality Control in Endoscopy Unit: Safety Considerations For The PatientPamela PampamNo ratings yet
- Guidelines On The Insertion and Management of CentralDocument18 pagesGuidelines On The Insertion and Management of CentralAgustina ItinNo ratings yet
- IV Therapy Report Outlines Steps and BenefitsDocument65 pagesIV Therapy Report Outlines Steps and BenefitsCamille Honeyleith Lanuza Fernando100% (2)
- A Clinical Pathway For The Management ofDocument7 pagesA Clinical Pathway For The Management ofBheru LalNo ratings yet
- 2015 Article 159Document8 pages2015 Article 159andri anaNo ratings yet
- COVID 19. 4 - 13 KashmerDocument42 pagesCOVID 19. 4 - 13 KashmerIshfaq GanaiNo ratings yet
- Eras Bps Sept16Document28 pagesEras Bps Sept16Muhaimin EfendiNo ratings yet
- Dialysis-Protocol For HD Catheter InsertionDocument18 pagesDialysis-Protocol For HD Catheter InsertionDewi Ratna SariNo ratings yet
- Guia IDSA Prevencion ICVCDocument32 pagesGuia IDSA Prevencion ICVCmaturana61No ratings yet
- Bmjopen 2014 007257Document7 pagesBmjopen 2014 007257rezzkNo ratings yet
- Paediatric Intrathecal Antibiotic ProcedureDocument9 pagesPaediatric Intrathecal Antibiotic ProcedureAbu Azzam Al-HadiNo ratings yet
- Worldviews Ev Based Nurs - 2015 - Morrison - The Effectiveness of Clinically Indicated Replacement of PeripheralDocument12 pagesWorldviews Ev Based Nurs - 2015 - Morrison - The Effectiveness of Clinically Indicated Replacement of PeripheralDARWIN JAY SANG-ANNo ratings yet
- 1-s2.0-S0749070424000071Document18 pages1-s2.0-S0749070424000071أركان هيلث Arkan healthNo ratings yet
- SOP Patient Haemodialysis Care - CopyDocument50 pagesSOP Patient Haemodialysis Care - Copypj rakNo ratings yet
- Article ContentDocument10 pagesArticle ContentRicardo Muñoz PérezNo ratings yet
- Picc Infection PDFDocument16 pagesPicc Infection PDFMahesh ChandraNo ratings yet
- AKI COVID-19 Recommendations Document 03.21.2020Document5 pagesAKI COVID-19 Recommendations Document 03.21.2020Melissa Tunarosa MurciaNo ratings yet
- Intravenous Parenteral TherapyDocument110 pagesIntravenous Parenteral TherapyDarran Earl Gowing100% (1)
- Cathet Cardio Intervent - 2005 - Chambers - Infection Control Guidelines For The Cardiac Catheterization LaboratoryDocument9 pagesCathet Cardio Intervent - 2005 - Chambers - Infection Control Guidelines For The Cardiac Catheterization Laboratorygadhang dewanggaNo ratings yet
- Positive Effect of Care Bundles On Patients With Central Venous Catheter Insertions at A Tertiary Hospital in Beijing, ChinaDocument10 pagesPositive Effect of Care Bundles On Patients With Central Venous Catheter Insertions at A Tertiary Hospital in Beijing, ChinaElfina NataliaNo ratings yet
- Catheter Related Bloodstream Infection (CRBSI)Document36 pagesCatheter Related Bloodstream Infection (CRBSI)aringkinkingNo ratings yet
- Pencegahan Infeksi Aliran Darah Akibat Bakteri Resisten Antibiotik Pada Pasien Di Rumah Sakit Jayarasti KusumanegaraDocument25 pagesPencegahan Infeksi Aliran Darah Akibat Bakteri Resisten Antibiotik Pada Pasien Di Rumah Sakit Jayarasti KusumanegaraJayarasti KusumanegaraNo ratings yet
- Use of Short Peripheral Intravenous Catheters: Characteristics, Management, and Outcomes WorldwideDocument7 pagesUse of Short Peripheral Intravenous Catheters: Characteristics, Management, and Outcomes WorldwidemochkurniawanNo ratings yet
- 15Document21 pages15Tyson Easo JonesNo ratings yet
- HCA Venesection SOPDocument20 pagesHCA Venesection SOPDebby Adhila ShanahanNo ratings yet
- Motorcycle DiariesDocument5 pagesMotorcycle DiariesTharun kumarNo ratings yet
- PD QUALITY STANDARDS - 07082019 Edit - Ong SBDocument24 pagesPD QUALITY STANDARDS - 07082019 Edit - Ong SBNor Afzan Mohd TahirNo ratings yet
- 05 N293 33108Document23 pages05 N293 33108Arjay G ParaniNo ratings yet
- Urinary Catheterisation and Catheter Care in Adults GuidelinesDocument37 pagesUrinary Catheterisation and Catheter Care in Adults GuidelinesAllend Reidene Viyar100% (1)
- Guidelines For The Clinical Application of Laparoscopic Biliary Tract SurgeryDocument37 pagesGuidelines For The Clinical Application of Laparoscopic Biliary Tract SurgeryTerence SalazarNo ratings yet
- Percutaneous NephrosDocument17 pagesPercutaneous NephrosIan HuangNo ratings yet
- Insertion and Management of Peripheral Intravenous Cannulae in Western Australian Healthcare Facilities PolicyDocument22 pagesInsertion and Management of Peripheral Intravenous Cannulae in Western Australian Healthcare Facilities PolicyChristian RSNo ratings yet
- Bedside Sheets Safety FullDocument6 pagesBedside Sheets Safety FullHue LeNo ratings yet
- IV Therapy Level III NCM LectureDocument8 pagesIV Therapy Level III NCM LectureEva A BaldozaNo ratings yet
- Periprocedural Management With Antithrombotic Therapy Adult Inpatient Ambulatory Guideline 20201029Document14 pagesPeriprocedural Management With Antithrombotic Therapy Adult Inpatient Ambulatory Guideline 20201029Joanne HoNo ratings yet
- IV Theraphy and Blood TransfusionDocument128 pagesIV Theraphy and Blood TransfusionJoycee BoNo ratings yet
- 2014 - Guidelines For Safety in The Gastrointestinal Endoscopy Unit PDFDocument10 pages2014 - Guidelines For Safety in The Gastrointestinal Endoscopy Unit PDFBaim FarmaNo ratings yet
- Noninvasive Monitoring 2016Document6 pagesNoninvasive Monitoring 2016Maria LaiaNo ratings yet
- Lean Six Sigma For Intravenous TherapyDocument9 pagesLean Six Sigma For Intravenous TherapyJenifer Lopez SuarezNo ratings yet
- Joacp 35 29Document6 pagesJoacp 35 29kenjiNo ratings yet
- HAI bUNDLESDocument54 pagesHAI bUNDLESNurhayati100% (1)
- DialysisDocument20 pagesDialysisSiwani rai100% (1)
- Плаквенил - терапия - UCSF Adult COVID draft management guidelinesDocument21 pagesПлаквенил - терапия - UCSF Adult COVID draft management guidelinesGuy MskNo ratings yet
- Insertion Mangement Peripheral IVCannulaDocument20 pagesInsertion Mangement Peripheral IVCannulaAadil AadilNo ratings yet
- Ofac 525Document10 pagesOfac 525mochkurniawanNo ratings yet
- Fluid Management in ARDS: An Evaluation of Current Practice and The Association Between Early Diuretic Use and Hospital MortalityDocument11 pagesFluid Management in ARDS: An Evaluation of Current Practice and The Association Between Early Diuretic Use and Hospital MortalitywasiNo ratings yet
- My Mind and MeDocument1 pageMy Mind and MeJoy Ce VeralloNo ratings yet
- Disaster Report FinalllllDocument46 pagesDisaster Report FinalllllJoy Ce VeralloNo ratings yet
- Phil. Lit ModuleDocument10 pagesPhil. Lit ModuleJoy Ce VeralloNo ratings yet
- NCM 118: Nursing Care of Clients with Life Threatening SIRSDocument35 pagesNCM 118: Nursing Care of Clients with Life Threatening SIRSJoy Ce VeralloNo ratings yet
- Little ThingsDocument3 pagesLittle ThingszwartwerkerijNo ratings yet
- Frequently Asked Questions About Ailunce HD1: Where Can Find HD1 Software & Firmware?Document5 pagesFrequently Asked Questions About Ailunce HD1: Where Can Find HD1 Software & Firmware?Eric Contra Color0% (1)
- Orion C.M. HVAC Case Study-07.25.23Document25 pagesOrion C.M. HVAC Case Study-07.25.23ledmabaya23No ratings yet
- FIL M 216 2nd Yer Panitikan NG PilipinasDocument10 pagesFIL M 216 2nd Yer Panitikan NG PilipinasJunas LopezNo ratings yet
- Summative Test For Quadratic Equations2Document2 pagesSummative Test For Quadratic Equations2AsmiraMangontra0% (1)
- GMS175CSDocument4 pagesGMS175CScorsini999No ratings yet
- Lecture Euler EquationDocument33 pagesLecture Euler EquationYash RajNo ratings yet
- Ip 19 3RD EditionDocument240 pagesIp 19 3RD EditionSumanta Bhaya100% (13)
- An Introduction To Log ShootingDocument10 pagesAn Introduction To Log ShootingSorin GociuNo ratings yet
- 01 The-Mckinsey-Edge-Hattori-En-26154Document5 pages01 The-Mckinsey-Edge-Hattori-En-26154Waqar AhmedNo ratings yet
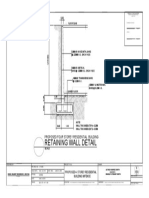
- Retaining Wall DetailsDocument1 pageRetaining Wall DetailsWilbert ReuyanNo ratings yet
- MINTZBERGDocument32 pagesMINTZBERGgeezee10004464100% (2)
- A Rail-To-Rail Constant Gain Buffered Op-Amp For Real Time Video ApplicationsDocument8 pagesA Rail-To-Rail Constant Gain Buffered Op-Amp For Real Time Video Applicationskvpk_vlsiNo ratings yet
- Red Lion Edict-97 - Manual PDFDocument282 pagesRed Lion Edict-97 - Manual PDFnaminalatrukNo ratings yet
- Senior High School Tracks: Free Powerpoint Templates Free Powerpoint TemplatesDocument11 pagesSenior High School Tracks: Free Powerpoint Templates Free Powerpoint TemplatesGeraldineNo ratings yet
- Comparative Media SystemsDocument10 pagesComparative Media SystemsJoram MutwiriNo ratings yet
- 2 Both Texts, and Then Answer Question 1 On The Question Paper. Text A: Esports in The Olympic Games?Document2 pages2 Both Texts, and Then Answer Question 1 On The Question Paper. Text A: Esports in The Olympic Games?...No ratings yet
- BSNL TrainingDocument25 pagesBSNL TrainingAditya Dandotia68% (19)
- 21st Century Literary GenresDocument2 pages21st Century Literary GenresGO2. Aldovino Princess G.No ratings yet
- Classification of AnimalsDocument6 pagesClassification of Animalsapi-282695651No ratings yet
- Temenos Brochure - FormpipeDocument5 pagesTemenos Brochure - FormpipeDanial OngNo ratings yet
- M.Com Second Semester – Advanced Cost Accounting MCQDocument11 pagesM.Com Second Semester – Advanced Cost Accounting MCQSagar BangreNo ratings yet
- READMEDocument3 pagesREADMERadu TimisNo ratings yet
- Basic Facts in EventDocument1 pageBasic Facts in EventAllan AgpaloNo ratings yet
- AlternatorDocument3 pagesAlternatorVatsal PatelNo ratings yet
- Twingo 3 & Clio 4Document10 pagesTwingo 3 & Clio 4Alexandre Le GrandNo ratings yet
- Board Question Paper: March 2018: Geography and EconomicsDocument2 pagesBoard Question Paper: March 2018: Geography and EconomicsVishvajit PatilNo ratings yet
- HonorDishonorProcess - Victoria Joy-1 PDFDocument126 pagesHonorDishonorProcess - Victoria Joy-1 PDFarjay1266100% (3)
- Joe Ann MarcellanaDocument17 pagesJoe Ann MarcellanarudyNo ratings yet
- Sunera Best Practices For Remediating SoDsDocument7 pagesSunera Best Practices For Remediating SoDssura anil reddyNo ratings yet