You might also like
- Unit 203 ConsultationssDocument19 pagesUnit 203 Consultationssapi-264759453No ratings yet
- 8 Hr. Hair Removal Waxing Concept: Segment OutlineDocument22 pages8 Hr. Hair Removal Waxing Concept: Segment OutlineFitzgerald Pacheco100% (2)
- New Hair Restoration Ebook PDFDocument135 pagesNew Hair Restoration Ebook PDFsankopubNo ratings yet
- Top Knife - Cutted - Top PDFDocument238 pagesTop Knife - Cutted - Top PDFIvanKazaiev100% (1)
- Soft Tissue Analysis (Autosaved)Document126 pagesSoft Tissue Analysis (Autosaved)Ayushi Toley100% (1)
- Hair TransplantDocument80 pagesHair TransplantMir Laieeq75% (4)
- AlopeciaDocument113 pagesAlopeciaRika RevinaNo ratings yet
- Hair Transplant: DR Imran Adeel Consultant Plastic Surgeon Quaid e Azam Medical College BahawalpurDocument48 pagesHair Transplant: DR Imran Adeel Consultant Plastic Surgeon Quaid e Azam Medical College BahawalpurFakhra TehseenNo ratings yet
- Hair Tranplants Melbourne FLDocument3 pagesHair Tranplants Melbourne FLgelmanhairNo ratings yet
- Hair Transplant Consent FormDocument7 pagesHair Transplant Consent FormHossam Abd algawadNo ratings yet
- Hair Restoration: Alfonso Barrera, MD, FACSDocument8 pagesHair Restoration: Alfonso Barrera, MD, FACSmarco gutierrezNo ratings yet
- Hair Transplant Consent Form 1Document7 pagesHair Transplant Consent Form 1dr. CalvLieNo ratings yet
- Affection of Horn: Diseases of Integumentary SystemDocument31 pagesAffection of Horn: Diseases of Integumentary SystemInam khanNo ratings yet
- Hair Transplantation Update-Dermatologic Clinics (2012)Document13 pagesHair Transplantation Update-Dermatologic Clinics (2012)masmoreraNo ratings yet
- Be Beautiful With Stem CellsDocument11 pagesBe Beautiful With Stem Cellsapi-253545554No ratings yet
- The Forensic Analysis of HairDocument21 pagesThe Forensic Analysis of HairTJPlayzNo ratings yet
- Hair Transplant Consent Form 1Document7 pagesHair Transplant Consent Form 1dr. CalvLieNo ratings yet
- HairDocument31 pagesHairShaurya100% (1)
- Hair4u MedDocument87 pagesHair4u MedkurutalaNo ratings yet
- Procedure: Pre-Operative Assessment and PlanningDocument2 pagesProcedure: Pre-Operative Assessment and PlanningRudyNo ratings yet
- Nishant Singh (The Forensic Analysis of Hair) FinalDocument23 pagesNishant Singh (The Forensic Analysis of Hair) FinalShikhar NigamNo ratings yet
- Mr. Zahid HTS SummaryDocument2 pagesMr. Zahid HTS SummaryothairclubNo ratings yet
- Hair RestorationDocument21 pagesHair RestorationNejat EsenerNo ratings yet
- LHR Full Details - 1.03.21Document38 pagesLHR Full Details - 1.03.21chauhanpriyanshu059No ratings yet
- Nipple Reconstruction FINALDocument39 pagesNipple Reconstruction FINALBarath Kumar SinghNo ratings yet
- Chapter 20Document84 pagesChapter 20Ana Brigigida NunezNo ratings yet
- Principles in Plastic SurgeryDocument49 pagesPrinciples in Plastic SurgerySurgery ResidentNo ratings yet
- 2.hair DisordersDocument50 pages2.hair DisordersAzeem Majid100% (3)
- Lecture 11 RegionalDocument34 pagesLecture 11 RegionalAbed AlawnehNo ratings yet
- Curly Hair TransplantDocument1 pageCurly Hair Transplantjean francois ngan tjenNo ratings yet
- Principles of Orofacial ReconstructionDocument29 pagesPrinciples of Orofacial ReconstructionMohd ZahiNo ratings yet
- Basic BraidingDocument17 pagesBasic BraidingMARIALUPE ESTOQUENo ratings yet
- Aa 1 1Document52 pagesAa 1 1Jaweed NaqshbandiNo ratings yet
- Hair4U 10% MedicalDocument50 pagesHair4U 10% MedicalkurutalaNo ratings yet
- Idenitification of HairDocument52 pagesIdenitification of HairelashmawyhagerNo ratings yet
- A Scan BiometryDocument37 pagesA Scan BiometryAnonymous Wb2LoZv9c100% (1)
- Reviewer in Hairdressing (From Pointers)Document4 pagesReviewer in Hairdressing (From Pointers)peanut nutterNo ratings yet
- Examination of Aspirates For Leishmania AmastigotesDocument35 pagesExamination of Aspirates For Leishmania AmastigotesMegbaruNo ratings yet
- Forensics of Hair AnalysisDocument28 pagesForensics of Hair AnalysisNyanmaruNo ratings yet
- Forensics of Hair AnalysisDocument29 pagesForensics of Hair AnalysisEub EuNo ratings yet
- 31594hair Transplant The ClinicDocument3 pages31594hair Transplant The ClinichairtransplantmailtronlineabcdefghijklmnopqrstuvwxNo ratings yet
- Hair & Fiber Analysis: ©anthony & Patricia BertinoDocument40 pagesHair & Fiber Analysis: ©anthony & Patricia BertinoNormalyn Andres MacaysaNo ratings yet
- Derma HairDocument11 pagesDerma HairBhavuk BansalNo ratings yet
- Cos - Chapter 11 Properties of The Hair and ScalpDocument9 pagesCos - Chapter 11 Properties of The Hair and ScalpRhoda Mica J. Limon100% (1)
- Anatomy and Physiology Day 2Document32 pagesAnatomy and Physiology Day 2Lake JazzNo ratings yet
- GH10 - Style and Finish HairDocument29 pagesGH10 - Style and Finish HairShipra SinghNo ratings yet
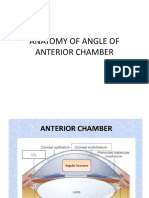
- Anatomy of Angle of Anterior ChamberDocument67 pagesAnatomy of Angle of Anterior ChamberRahnaNo ratings yet
- Hair DisordersDocument38 pagesHair DisordersMoayad NawaflehNo ratings yet
- OCT MaculaDocument71 pagesOCT MaculaNasrin sultana rmcNo ratings yet
- 206897hair Transplant in Turkey ClinicDocument3 pages206897hair Transplant in Turkey ClinichairtransplantmailtronlineabcdefghijklmnopqrstuvwxNo ratings yet
- Scalp PDFDocument7 pagesScalp PDFduranduran11No ratings yet
- Local Flaps in Head &neck ReconstructionDocument85 pagesLocal Flaps in Head &neck Reconstructiontegegnegenet2No ratings yet
- Hair and Fiber AnalysisDocument37 pagesHair and Fiber AnalysisKaleem KhanNo ratings yet
- Hair Transplantation: With Follicular Unit MicrograftsDocument2 pagesHair Transplantation: With Follicular Unit MicrograftsRavvaNo ratings yet
- MicrosurgeryDocument20 pagesMicrosurgeryNyein Chan AungNo ratings yet
- Physical Means of Treating Unwanted Hair: R W & T S. ADocument10 pagesPhysical Means of Treating Unwanted Hair: R W & T S. Adipika awindaNo ratings yet
- Reduce Hair Contamination To Zero - A Technical PerspectiveDocument22 pagesReduce Hair Contamination To Zero - A Technical PerspectiveRamasubramanian SankaranarayananNo ratings yet
- Anatomy of Cornea and ScleraDocument24 pagesAnatomy of Cornea and ScleraOphthalmology DiscussionNo ratings yet
- Hema I Chapter 3 - PhlebotomyDocument118 pagesHema I Chapter 3 - Phlebotomyderibew100% (1)
- PhacoemulsificationDocument54 pagesPhacoemulsificationIshita Kinra100% (1)
- CryotherapyDocument35 pagesCryotherapyRusty RyanNo ratings yet
- BotoxDocument44 pagesBotoxRusty RyanNo ratings yet
- Vasculitis 1Document47 pagesVasculitis 1Rusty RyanNo ratings yet
- Chemical Peels ArticleDocument29 pagesChemical Peels ArticleRusty RyanNo ratings yet
- SARP (Skin Anesthesia Radiology Psychiatry) Review 2010Document4 pagesSARP (Skin Anesthesia Radiology Psychiatry) Review 2010QworldNo ratings yet
- Meshoma A Rare Complication of Abdomen and HerniaDocument3 pagesMeshoma A Rare Complication of Abdomen and HernialeartaNo ratings yet
- Hand SurgeryDocument2 pagesHand SurgeryplastaukNo ratings yet
- DR Ranjith MP Senior Resident Department of Cardiology Government Medical College KozhikodeDocument78 pagesDR Ranjith MP Senior Resident Department of Cardiology Government Medical College KozhikodePutu Adi SusantaNo ratings yet
- Shock: Ron Michael N. Olaguera 2 Year Surgery ResidentDocument40 pagesShock: Ron Michael N. Olaguera 2 Year Surgery ResidentErick Anca100% (2)
- Seminar On Acute PancreatitisDocument20 pagesSeminar On Acute PancreatitisJoice DasNo ratings yet
- Periop WorkbookDocument2 pagesPeriop WorkbookZhy CaluzaNo ratings yet
- Adult Brachial Plexus InjuryDocument13 pagesAdult Brachial Plexus Injurysunshine bloomNo ratings yet
- 5 IV Therapy TransesDocument9 pages5 IV Therapy TransesKeana Dacayana100% (1)
- Abdominal Paracentesis - Procedures - 5MinuteConsultDocument6 pagesAbdominal Paracentesis - Procedures - 5MinuteConsultJose MtzNo ratings yet
- CBR0040 Lightwave Brochure PDFDocument2 pagesCBR0040 Lightwave Brochure PDFAmir H NBNo ratings yet
- Pneumothorax GuidelineDocument8 pagesPneumothorax GuidelineIonut - Eugen IonitaNo ratings yet
- Ro-Jharkhand: List of Empanelled Hospitals Under Esic RegionDocument5 pagesRo-Jharkhand: List of Empanelled Hospitals Under Esic RegionShaina Hayat KhanNo ratings yet
- EPIDURALDocument3 pagesEPIDURALMarcos Jose WurschmidtNo ratings yet
- Factors Affecting Time of USCODocument10 pagesFactors Affecting Time of USCOMUBENGANo ratings yet
- Modified Technique For Esthetic Crown Lengthening in The Natural Dentition - Case SeriesDocument15 pagesModified Technique For Esthetic Crown Lengthening in The Natural Dentition - Case SeriesCentro Dental IntegralNo ratings yet
- 06-Systematic Review of Perforated Appendicitis and PhlegmonDocument7 pages06-Systematic Review of Perforated Appendicitis and PhlegmonTo MarNo ratings yet
- Laparoscopic SurgeryDocument16 pagesLaparoscopic Surgeryprincess-mendoza-de-guzman-808No ratings yet
- 11.sudden Natural Death 3Document55 pages11.sudden Natural Death 3Hasabo AwadNo ratings yet
- Lung Cancer EgansDocument15 pagesLung Cancer Eganslady birdNo ratings yet
- DC-70 Specification Ver 1.0 20140808Document17 pagesDC-70 Specification Ver 1.0 20140808miljenkoNo ratings yet
- Suture Materials and Suture TechniquesDocument17 pagesSuture Materials and Suture TechniquesimranNo ratings yet
- Explore LapDocument5 pagesExplore LapAngie MandeoyaNo ratings yet
- Final Checklist Nursing Skills Checklist-1 2Document7 pagesFinal Checklist Nursing Skills Checklist-1 2api-380107556No ratings yet
- Group 5 A.1 Axial BonesDocument7 pagesGroup 5 A.1 Axial BonesIsabella CariagaNo ratings yet
- Diaphragmatic Paralysis Associated With Neonatal Brachial Plexus PalsyDocument3 pagesDiaphragmatic Paralysis Associated With Neonatal Brachial Plexus PalsyDennyNo ratings yet
- MediCAD Brochure 2D + 3D (Except Shoulder)Document16 pagesMediCAD Brochure 2D + 3D (Except Shoulder)kocis_pNo ratings yet
- MCQDocument24 pagesMCQiqra jabeenNo ratings yet