You might also like
- Silicosis: Understanding the Deadly Lung DiseaseDocument72 pagesSilicosis: Understanding the Deadly Lung DiseaseAauLiiaa Lia LiiaNo ratings yet
- SilicosisDocument11 pagesSilicosisDurge Raj GhalanNo ratings yet
- B.SC Degree Course in Nursing (Basic) Medical - Surgical Nursing - II Unit - X Occupational Lung DiseasesDocument101 pagesB.SC Degree Course in Nursing (Basic) Medical - Surgical Nursing - II Unit - X Occupational Lung DiseasesvigneshNo ratings yet
- 5 6226231896498503742Document62 pages5 6226231896498503742dessypoerwantoNo ratings yet
- J NDF CGDocument6 pagesJ NDF CGDotia Modibo JamiuNo ratings yet
- Silica: The Deadly DustDocument45 pagesSilica: The Deadly DustpuskesmaskaliwunguNo ratings yet
- Restrictive Lung Diseases.Document59 pagesRestrictive Lung Diseases.Salman KhanNo ratings yet
- Occupational Lung Diseases: Pneumoconioses and Dust ExposureDocument11 pagesOccupational Lung Diseases: Pneumoconioses and Dust ExposureEMMANUEL BOTSHELONo ratings yet
- PNEUMOCONIOSISDocument53 pagesPNEUMOCONIOSISmaeliszxc kim100% (1)
- Silicosis Case Report from Faridpur Medical CollegeDocument3 pagesSilicosis Case Report from Faridpur Medical CollegeBunga RamadhaniNo ratings yet
- Silicosis and SilicotuberculosisDocument46 pagesSilicosis and SilicotuberculosisHaris Risdiana50% (2)
- PneumoconiosisDocument20 pagesPneumoconiosisankitkumaramit99No ratings yet
- Various Types of PneumoconiosisDocument20 pagesVarious Types of PneumoconiosisSharin K VargheseNo ratings yet
- DR / Ayman S. El-Khateeb Minia UniversityDocument20 pagesDR / Ayman S. El-Khateeb Minia UniversityKuruNo ratings yet
- Silicosis - UpToDateDocument44 pagesSilicosis - UpToDateyuliaNo ratings yet
- SilicosisDocument21 pagesSilicosisGadzikaNo ratings yet
- Mine DustDocument14 pagesMine DustdileepNo ratings yet
- Silica Silicosis TuberculosisDocument11 pagesSilica Silicosis TuberculosisAndrewNo ratings yet
- Part A-12-Wood Dust Allergies - Q&ADocument8 pagesPart A-12-Wood Dust Allergies - Q&Afernanda1rondelliNo ratings yet
- Presentation FinalDocument24 pagesPresentation FinalRahulNo ratings yet
- Respiratory Pathology IWS SilicosisDocument11 pagesRespiratory Pathology IWS SilicosisRameez MalekNo ratings yet
- PneumoconiosisDocument13 pagesPneumoconiosisSai charithaNo ratings yet
- Silica Dust Exposure TBT FINAL Oct 2017Document2 pagesSilica Dust Exposure TBT FINAL Oct 2017Herminio Román MoralesNo ratings yet
- Occupational Health - SilicosisDocument32 pagesOccupational Health - SilicosisEunice Co100% (1)
- Occupational Lung DiseaseDocument24 pagesOccupational Lung DiseaseprachitiNo ratings yet
- Ebook - The Effects of Mining On Human HealthDocument12 pagesEbook - The Effects of Mining On Human HealthLekha ANo ratings yet
- The Inorganic Dust Pneumoconioses: Richard P. Stankus and John E. SalvaggioDocument13 pagesThe Inorganic Dust Pneumoconioses: Richard P. Stankus and John E. SalvaggioAD DNo ratings yet
- Respiratory Disease GuideDocument59 pagesRespiratory Disease GuideGEORGENo ratings yet
- Environmental & Occupational Lung DiseasesDocument12 pagesEnvironmental & Occupational Lung Diseasesamm1101No ratings yet
- PneumoconiosisDocument7 pagesPneumoconiosisFriends ZoneNo ratings yet
- Construction Medical SurveyDocument4 pagesConstruction Medical SurveyVishnu AravindNo ratings yet
- 1.industrial DiseasesDocument4 pages1.industrial DiseasesShintonial OzileNo ratings yet
- Pneumokoniosis ReferatDocument7 pagesPneumokoniosis Referatbella yolandaNo ratings yet
- PneumoconiosisDocument19 pagesPneumoconiosisgabriela.was.gabbbieNo ratings yet
- All 14202Document13 pagesAll 14202sukiyantoNo ratings yet
- Dust Lung DiseasesDocument38 pagesDust Lung Diseasesankitkumaramit99No ratings yet
- Occupational Lung Disease Causes and EffectsDocument14 pagesOccupational Lung Disease Causes and EffectsEgy BagusNo ratings yet
- SilicosisDocument24 pagesSilicosisspecchioterraNo ratings yet
- Mechanisms of Silica-Induced Lung DiseaseDocument10 pagesMechanisms of Silica-Induced Lung DiseaseDang QuanNo ratings yet
- Jurnal Silikosis Dengan Pneumothorax PDFDocument6 pagesJurnal Silikosis Dengan Pneumothorax PDFfalisNo ratings yet
- Coal Workers' Lung Diseases: Attfield, Michael D. Petsonk, Edward L. Wagner, Gregory RDocument5 pagesCoal Workers' Lung Diseases: Attfield, Michael D. Petsonk, Edward L. Wagner, Gregory Rdwi rahwatiNo ratings yet
- Pneumoconiosis: Name and SynonymsDocument17 pagesPneumoconiosis: Name and Synonymsgasai gasaiNo ratings yet
- Coal worker's pneumoconiosis causes and symptomsDocument4 pagesCoal worker's pneumoconiosis causes and symptomsviren thakkarNo ratings yet
- Miner'S Diseases & Dust Hazards: NystagmusDocument7 pagesMiner'S Diseases & Dust Hazards: NystagmusPrabir GhoshNo ratings yet
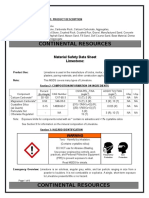
- Limestone MSDSDocument6 pagesLimestone MSDSSamuel GaétanNo ratings yet
- Pneumoconiosis Coal Worker'S Lungs: Mohana PreeshaDocument52 pagesPneumoconiosis Coal Worker'S Lungs: Mohana PreeshaChuks LeviNo ratings yet
- ByssinosisAsbestosis SilicosisDocument44 pagesByssinosisAsbestosis SilicosisMARK ARQUE LACANARIANo ratings yet
- Silicosis: Understanding the Dangers of Silica Dust ExposureDocument2 pagesSilicosis: Understanding the Dangers of Silica Dust ExposureFritz FontanillaNo ratings yet
- Occupational Lung DiseasesDocument75 pagesOccupational Lung DiseasesAnonymous h1XAlApsU100% (1)
- chp:10.1007/3 540 30903 9 - 11Document17 pageschp:10.1007/3 540 30903 9 - 11Alex MarinNo ratings yet
- Cystic Fibrosis PathophysiologyDocument5 pagesCystic Fibrosis PathophysiologyKim Enrico JumarangNo ratings yet
- Classification of DefectDocument5 pagesClassification of DefectbarbiemeNo ratings yet
- Hypersensitivity Pneumonitis Is Subdivided Into Two Forms: Acute and Chronic. Symptoms Differ For Each FormDocument4 pagesHypersensitivity Pneumonitis Is Subdivided Into Two Forms: Acute and Chronic. Symptoms Differ For Each FormSheree SorianoNo ratings yet
- Silicosis - Google SearchDocument1 pageSilicosis - Google Searchragesh r nairNo ratings yet
- Silicosis: An Update and Guide for CliniciansDocument14 pagesSilicosis: An Update and Guide for CliniciansLaras KinasihNo ratings yet
- Ward Class On Cystic FibrosisDocument58 pagesWard Class On Cystic FibrosisJannen CasasNo ratings yet
- Fujimura2000 (00001) PDFDocument5 pagesFujimura2000 (00001) PDFnantousNo ratings yet
- 10 Must Knows Words Related To Silica DustDocument3 pages10 Must Knows Words Related To Silica DustGRTNo ratings yet
- Silicosis in Artificial Stone Workers: Spectrum of Radiological High-Resolution CT Chest FindingsDocument9 pagesSilicosis in Artificial Stone Workers: Spectrum of Radiological High-Resolution CT Chest FindingsFabio GigliottiNo ratings yet
- Pulmonary FibrosisDocument4 pagesPulmonary FibrosisStefaniaM100% (1)
- Acute Respiratory Distress Syndrome: Jurnal RespirasiDocument11 pagesAcute Respiratory Distress Syndrome: Jurnal RespirasiArmia UsnihidayatiNo ratings yet
- Hatha YogaDocument188 pagesHatha YogaKumar Date80% (5)
- Case Study - Chest Tube MangementDocument4 pagesCase Study - Chest Tube MangementLee CelNo ratings yet
- 9th Grade Science Lesson on the Cardiovascular SystemDocument5 pages9th Grade Science Lesson on the Cardiovascular SystemOliver VillanuevaNo ratings yet
- EmphysemaDocument2 pagesEmphysemaapi-322389115No ratings yet
- Overview Ventilation ModesDocument18 pagesOverview Ventilation ModesDo NodsNo ratings yet
- 2020 Final Announcement PIPKRADocument31 pages2020 Final Announcement PIPKRAMario Okta Fiendi GintingNo ratings yet
- The Effects of Smoking On RespirationDocument1 pageThe Effects of Smoking On RespirationKumar JeevanNo ratings yet
- Nueva Ecija University of Science and Technology: Case 7Document7 pagesNueva Ecija University of Science and Technology: Case 7jomariNo ratings yet
- Pneumonia: (Related To Copious Tracheobronchial Secretions.)Document1 pagePneumonia: (Related To Copious Tracheobronchial Secretions.)Alyssa Mae DumularNo ratings yet
- Assessment of Respiratory System for AnesthesiaDocument49 pagesAssessment of Respiratory System for AnesthesiaMilanisti22No ratings yet
- Respirology Case Reports: Paradoxical Bronchospasm: A Rare Adverse Effect of Fenoterol UseDocument4 pagesRespirology Case Reports: Paradoxical Bronchospasm: A Rare Adverse Effect of Fenoterol UseDELLA LESTARINo ratings yet
- Burns ToxicologyDocument17 pagesBurns ToxicologyteuuuuNo ratings yet
- MSA Mainline Catalogue 2010Document252 pagesMSA Mainline Catalogue 2010Osama_Othman01100% (1)
- Acute Respiratory Distress Syndrome 2022Document182 pagesAcute Respiratory Distress Syndrome 2022Dalí Fuentes GonzalezNo ratings yet
- Acute Respiratory Distress Syndrome (Ards) : Muamar Aldalaeen, RN, Mba, HCRM, Cic, Ipm, MSN, Phd. Haneen Alnuaimi, MSNDocument59 pagesAcute Respiratory Distress Syndrome (Ards) : Muamar Aldalaeen, RN, Mba, HCRM, Cic, Ipm, MSN, Phd. Haneen Alnuaimi, MSNAboodsha ShNo ratings yet
- Diagnostic and Management of Hyaline Membrane Disease: August 2018Document11 pagesDiagnostic and Management of Hyaline Membrane Disease: August 2018Bella MonichaNo ratings yet
- Acute Respiratory Distress Syndrome (ARDS) : MR Sanjay. M. Peerapur, Principal, KLES Institute of Nursing Sciences, HubliDocument22 pagesAcute Respiratory Distress Syndrome (ARDS) : MR Sanjay. M. Peerapur, Principal, KLES Institute of Nursing Sciences, Hublimanish dafdaNo ratings yet
- COPD PathoDocument1 pageCOPD PathoGlenn_Ancheta_2074100% (1)
- Unit 7-Common Diseases and Conditions of Body SystemsDocument227 pagesUnit 7-Common Diseases and Conditions of Body Systemstau88100% (1)
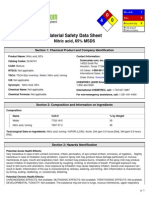
- Nitric acid, 65% MSDSDocument6 pagesNitric acid, 65% MSDSBharat J ShettyNo ratings yet
- 97893990619016Document14 pages97893990619016Khawla BahryNo ratings yet
- Lung Ultrasound in The Critically IllDocument50 pagesLung Ultrasound in The Critically IllJillNo ratings yet
- Asthma Lesson PlanDocument29 pagesAsthma Lesson PlanRabiu Hassan Musa86% (7)
- Final Concept MapDocument7 pagesFinal Concept Mapapi-405374041No ratings yet
- Mechanical Ventilator Management ProtocolDocument3 pagesMechanical Ventilator Management ProtocolRick Frea100% (2)
- Ncma219 Lec MidtermDocument51 pagesNcma219 Lec MidtermMacababbad Joshua MiguelNo ratings yet
- Thoracic Injuries Chapter QuestionsDocument12 pagesThoracic Injuries Chapter QuestionsRifka Anisa0% (1)
- Nursing Memory JoggersDocument2 pagesNursing Memory JoggersMel Tabanao100% (1)