You might also like
- StrabismusDocument61 pagesStrabismusOmesh PrathirajaNo ratings yet
- Concomitant Squint: Noor Asmah MD Azmi Optometrist HsahDocument56 pagesConcomitant Squint: Noor Asmah MD Azmi Optometrist HsahAnonymous l2Fve4PpD33% (3)
- SquintDocument36 pagesSquintbismahNo ratings yet
- Strabismus & Amblyopia: Dr. Boyke Sisprihattono, SPMDocument24 pagesStrabismus & Amblyopia: Dr. Boyke Sisprihattono, SPMranz ibonkNo ratings yet
- Strabismus & Amblyopia: Dr. Boyke Sisprihattono, SPMDocument24 pagesStrabismus & Amblyopia: Dr. Boyke Sisprihattono, SPMPurnomo Ponco NugrohoNo ratings yet
- Non-Concomitant Strabismus 2Document60 pagesNon-Concomitant Strabismus 2Ijeoma Okpalla100% (2)
- 8-Strabismus & AmbliopiaDocument24 pages8-Strabismus & AmbliopiaMuhammad Faisal100% (1)
- HeterophoriaDocument25 pagesHeterophoriatehreem tanveerNo ratings yet
- StrabismusDocument21 pagesStrabismusWardahNo ratings yet
- Anomalies of Accommodation.Document31 pagesAnomalies of Accommodation.Taiba RafiqNo ratings yet
- Ocular Motility: Department of Ophthalmology Fatima College of MedicineDocument41 pagesOcular Motility: Department of Ophthalmology Fatima College of MedicineMohammedHuzairIbunuAbidNo ratings yet
- BV Exam2Document33 pagesBV Exam2Andrew CoatesNo ratings yet
- Strabismus: Dr. Digin Mariam OphthalmologyDocument94 pagesStrabismus: Dr. Digin Mariam OphthalmologyVishnu SaiNo ratings yet
- Klasifikasi StrabismusDocument72 pagesKlasifikasi Strabismusbonny_07_fk_unsri9248No ratings yet
- HYPERMETROPIA and Myopia PDFDocument55 pagesHYPERMETROPIA and Myopia PDFDrashti ChudasamaNo ratings yet
- Binocular Vision Disorder: - Non Strabismus Problems - Strabismus - Amblyopia - SteriopsisDocument74 pagesBinocular Vision Disorder: - Non Strabismus Problems - Strabismus - Amblyopia - SteriopsisHenok BirukNo ratings yet
- Accommodative Esotropia: Rishabh Gupta M.Optom 1 YearDocument10 pagesAccommodative Esotropia: Rishabh Gupta M.Optom 1 YearRishabh GuptaNo ratings yet
- 6 StrabismusDocument49 pages6 StrabismusMariam QaisNo ratings yet
- AMETROPIADocument48 pagesAMETROPIARahul KirkNo ratings yet
- Esodeviation الحول الإنسيDocument33 pagesEsodeviation الحول الإنسيYaman MuhaisenNo ratings yet
- Childhood StrabismusDocument25 pagesChildhood StrabismusRYrstmNo ratings yet
- 51childhood StrabismusDocument18 pages51childhood StrabismusEstuNo ratings yet
- Infantile Strabismus - 9Document35 pagesInfantile Strabismus - 9Lavanya MadabushiNo ratings yet
- DT StrabismusDocument42 pagesDT StrabismushamzahNo ratings yet
- Lecture 11 Special Senses Part 6-VisionDocument48 pagesLecture 11 Special Senses Part 6-VisionMoses Jr KazevuNo ratings yet
- Management of Nystagmus - The Ophthalmologist S PerspectiveDocument55 pagesManagement of Nystagmus - The Ophthalmologist S PerspectiveZaras Yudisthira SagaNo ratings yet
- Congenital Strabismus: S. Vanitha, B.optom, 3 YearDocument23 pagesCongenital Strabismus: S. Vanitha, B.optom, 3 YearDivya Priya Dharmalingam100% (1)
- 6-History and Examination Part 2Document27 pages6-History and Examination Part 2AmrNo ratings yet
- InggrisDocument32 pagesInggrisRani Dwi HapsariNo ratings yet
- Chapter 11 Eye & Vision DisordersDocument72 pagesChapter 11 Eye & Vision DisordersMYLENE GRACE ELARCOSANo ratings yet
- 2 - BPE - Eye ExaminationDocument50 pages2 - BPE - Eye ExaminationZauhar NurdildayevaNo ratings yet
- Opthalmic Emergencies PresentationDocument85 pagesOpthalmic Emergencies PresentationvictoreffiomNo ratings yet
- Strab: IsmusDocument93 pagesStrab: IsmusUlquiorra SchifferNo ratings yet
- Refractive ErrorsDocument33 pagesRefractive ErrorsMathew Sebastian100% (2)
- Tes HenserbergDocument16 pagesTes HenserberghamzahNo ratings yet
- Care of The Clients With Eye and Ear DisorderDocument35 pagesCare of The Clients With Eye and Ear DisorderKristine Joy RevañoNo ratings yet
- Objective - Subjective Eye Examination-Referral System and When To ReferDocument56 pagesObjective - Subjective Eye Examination-Referral System and When To ReferClara Sainuka100% (1)
- Strabismus & Ambliopia - LTDocument24 pagesStrabismus & Ambliopia - LTharshveerNo ratings yet
- Kudakwashe Magogo BV Assignment 2Document4 pagesKudakwashe Magogo BV Assignment 2Kudakwashe MagogoNo ratings yet
- Nungki-Esodeviations & ExodeviationsDocument36 pagesNungki-Esodeviations & ExodeviationsNia RoosdhantiaNo ratings yet
- Strabismus and Amblyopia: Allen Habajab Samantha ReyesDocument23 pagesStrabismus and Amblyopia: Allen Habajab Samantha Reyesallenh016No ratings yet
- Eye Movement Disorders: Professor Dr. Ayman Youssef Ezeddin EassaDocument25 pagesEye Movement Disorders: Professor Dr. Ayman Youssef Ezeddin EassaEhab Khiry100% (1)
- Refractive Disorders Blok VisualDocument27 pagesRefractive Disorders Blok Visualmuhammad ajiNo ratings yet
- Cataract SenilisDocument54 pagesCataract Senilismayo djitroNo ratings yet
- Strabismus: By: Audra Bishop Beth Moline Elisabeth CohenDocument60 pagesStrabismus: By: Audra Bishop Beth Moline Elisabeth CohenmalathiNo ratings yet
- Squint 20240210 204429Document22 pagesSquint 20240210 204429Madhura Pushpa kumaraNo ratings yet
- Squint Evaluation 1Document69 pagesSquint Evaluation 1rucha kacha100% (2)
- HEENT HX and P Examination (Repaired)Document77 pagesHEENT HX and P Examination (Repaired)ObsaNo ratings yet
- Strabismus For Med VDocument102 pagesStrabismus For Med Vhenok birukNo ratings yet
- Pemeriksaan Dasar MataDocument103 pagesPemeriksaan Dasar Mataandhie_soyNo ratings yet
- Strabismus: Satrio Wahyu Sadewo I11109039Document20 pagesStrabismus: Satrio Wahyu Sadewo I11109039Satrio Wahyu SadewoNo ratings yet
- Anomalies of Accommodation: Mr. Natnael L. (Lecturer) April/2017Document33 pagesAnomalies of Accommodation: Mr. Natnael L. (Lecturer) April/2017henok birukNo ratings yet
- Amblyopia: Glomarie Hope A. Paquera Danica Ilah M. SincoDocument39 pagesAmblyopia: Glomarie Hope A. Paquera Danica Ilah M. SincoJan IrishNo ratings yet
- AmblyopiaDocument28 pagesAmblyopiaAndhika YogiswaraNo ratings yet
- StrabismusDocument32 pagesStrabismusparugandooNo ratings yet
- 8 SquintDocument46 pages8 Squintwanderer_1010No ratings yet
- Eye Movement AbnormalitiesDocument34 pagesEye Movement AbnormalitiesSeshagiri DoniparthiNo ratings yet
- Ophthalmology: Sofia Sipin, MD Pediatric OphthalmologistDocument62 pagesOphthalmology: Sofia Sipin, MD Pediatric OphthalmologistPrincess Noreen SavellanoNo ratings yet
- Peripheral Vestibular DisordersDocument42 pagesPeripheral Vestibular Disorders李丞永No ratings yet
- Cranial Nerves TableDocument2 pagesCranial Nerves TableJhielo ArambulaNo ratings yet
- Human Nervous SystemDocument14 pagesHuman Nervous SystemAshah SeevarathenamNo ratings yet
- BS en 00172-1995 (2002)Document20 pagesBS en 00172-1995 (2002)myenas87No ratings yet
- EndophthalmitisDocument2 pagesEndophthalmitisakillerbeast632No ratings yet
- Pre-And Post-Operative Intraocular Pressure of Pediatric Cataract SurgeryDocument5 pagesPre-And Post-Operative Intraocular Pressure of Pediatric Cataract SurgeryKris AdinataNo ratings yet
- Daftar PustakaDocument8 pagesDaftar PustakaStefan SaerangNo ratings yet
- 10 Minute CGADocument15 pages10 Minute CGAIrene Veron Bernardo ChicoNo ratings yet
- Cornea 2 Volume Set 5Th Edition Mark J Mannis MD Facs Full ChapterDocument67 pagesCornea 2 Volume Set 5Th Edition Mark J Mannis MD Facs Full Chapterdonald.mccrea778100% (4)
- Retinopathy of Prematurity: Aao Reading Subdiv Vitreo-RetinaDocument35 pagesRetinopathy of Prematurity: Aao Reading Subdiv Vitreo-RetinaHerin NataliaNo ratings yet
- Collaboration With African Traditional Healers For The Prevention of BlindnessDocument58 pagesCollaboration With African Traditional Healers For The Prevention of BlindnessAliNo ratings yet
- Anatomy and Physiology With PhatophysiologyDocument8 pagesAnatomy and Physiology With PhatophysiologyJustine Mae OyongNo ratings yet
- Update On Refractive SurgeryDocument15 pagesUpdate On Refractive SurgeryStefanieNo ratings yet
- NDT - Tech 02 1Document8 pagesNDT - Tech 02 1mark_59No ratings yet
- OT Mom Learning Activities: Visual PerceptionDocument4 pagesOT Mom Learning Activities: Visual PerceptionDamayanti Thapa100% (1)
- Mine 1Document55 pagesMine 1emeNo ratings yet
- Visual AcuityDocument9 pagesVisual AcuityauliaNo ratings yet
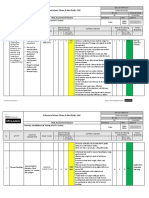
- Risk Assessment For Installation and Testing of CCTVDocument11 pagesRisk Assessment For Installation and Testing of CCTVAnandu Ashokan100% (4)
- ODC Form 1ADocument11 pagesODC Form 1ADaphne MagsiNo ratings yet
- MDWF 2070 Drug Protocol ErthyromycinDocument1 pageMDWF 2070 Drug Protocol Erthyromycinapi-442131145No ratings yet
- Prevalence and Associated Factor of Glaucoma in Aligarh, India A Population Based StudyDocument6 pagesPrevalence and Associated Factor of Glaucoma in Aligarh, India A Population Based StudyBeci TomNo ratings yet
- Case Study Analysis - Aravind HospitalDocument6 pagesCase Study Analysis - Aravind Hospitalsubhadip100% (1)
- Fellowship Medical RetinaDocument5 pagesFellowship Medical RetinaThe Doctor's InterestsNo ratings yet
- Ocular ProstheticsDocument2 pagesOcular ProstheticsEshiramhe AugustineNo ratings yet
- Role of Ophthalmic Nurses With Visually Impaired PatientsDocument6 pagesRole of Ophthalmic Nurses With Visually Impaired PatientsIsaac Aleman0% (1)
- Module 8: The Scholar'S Journey: Learning Activity 1Document4 pagesModule 8: The Scholar'S Journey: Learning Activity 1Danizelle Kaye Cadocoy Bernardo100% (1)
- BLINDNESSDocument24 pagesBLINDNESSpriyagerardNo ratings yet
- Prevalence and Risk Factors For Myopia Among School Children in Aba (Pdfdrive)Document109 pagesPrevalence and Risk Factors For Myopia Among School Children in Aba (Pdfdrive)Esther AkwuruohaNo ratings yet
- Hill IQ PreferenceDocument4 pagesHill IQ PreferencefdoaguayoNo ratings yet
- M-7 Dr. Vimala Menon: P-10 Dr. Phiroze PatelDocument58 pagesM-7 Dr. Vimala Menon: P-10 Dr. Phiroze PatelShiwali SinghNo ratings yet
- Do's and Don'ts For Wearing Contact LensDocument1 pageDo's and Don'ts For Wearing Contact LensMrkikuNo ratings yet