You might also like
- My Mifespristone and Misoprostol Story: How I used mifepristone and misoprostol for a successful medical abortion and all you must know about these abortion pillsFrom EverandMy Mifespristone and Misoprostol Story: How I used mifepristone and misoprostol for a successful medical abortion and all you must know about these abortion pillsNo ratings yet
- Clinical Obstetrics/Gynecology Review 2023: For USMLE Step 2 CK and COMLEX-USA Level 2From EverandClinical Obstetrics/Gynecology Review 2023: For USMLE Step 2 CK and COMLEX-USA Level 2Rating: 4 out of 5 stars4/5 (1)
- Drugs in ObstDocument32 pagesDrugs in ObstĶHwola ƏľsHokryNo ratings yet
- Drug Data for Oxytocin, Methergine, Hyoscine, Vitamin K and Eye Care ProphylaxisDocument4 pagesDrug Data for Oxytocin, Methergine, Hyoscine, Vitamin K and Eye Care ProphylaxisJune Dumdumaya67% (3)
- Drugs Used in ObstetricsDocument6 pagesDrugs Used in ObstetricsJubin RajuNo ratings yet
- Drugs Used in ObstetricsDocument21 pagesDrugs Used in Obstetricssuchismita panda100% (2)
- Drugs - OBGDocument85 pagesDrugs - OBGKENEDYNo ratings yet
- 4th Year - Unit 5 - Pharmacotherapeutics in Obstetrics 1Document13 pages4th Year - Unit 5 - Pharmacotherapeutics in Obstetrics 1Rupa Ghosh100% (1)
- Drugs in PregnancyDocument52 pagesDrugs in Pregnancydarboeb265100% (2)
- 04 Oxytocics Group ADocument53 pages04 Oxytocics Group AKamal GhimireNo ratings yet
- Oxytocin and Methylergonovine Nursing StudyDocument16 pagesOxytocin and Methylergonovine Nursing StudyDinarkram Rabreca EculNo ratings yet
- Drugs Used in ObstetricsDocument37 pagesDrugs Used in ObstetricsWhirmey ChinyamaNo ratings yet
- Oxytocin and Drugs Acting on the Uterus (1)Document56 pagesOxytocin and Drugs Acting on the Uterus (1)KasturiRangan SrivatsaNo ratings yet
- DrugsDocument81 pagesDrugsrevathidadam55555100% (1)
- Drugs Used in Obstetric Emergencies: Vasanthakumari, MSC (N)Document56 pagesDrugs Used in Obstetric Emergencies: Vasanthakumari, MSC (N)revathidadam55555100% (1)
- Methylergonovine maleate postpartum careDocument2 pagesMethylergonovine maleate postpartum careRitamariaNo ratings yet
- UntitledDocument7 pagesUntitledShalabh JoharyNo ratings yet
- On Nursing Responsibilities of Drugs in ObstetricsDocument117 pagesOn Nursing Responsibilities of Drugs in ObstetricsSanjita Kumari PanditNo ratings yet
- OBSTETRICS drugsDocument6 pagesOBSTETRICS drugsDan Agyemang NketiahNo ratings yet
- Uterine StimulantsDocument24 pagesUterine StimulantsKilp MosesNo ratings yet
- Drugs I (Obgy)Document85 pagesDrugs I (Obgy)Aman Shaikh100% (2)
- Drug Study: ENRIQUEZ, Angelique Jade C. BSN 2 C4Document4 pagesDrug Study: ENRIQUEZ, Angelique Jade C. BSN 2 C4Angelique Jade EnriquezNo ratings yet
- MethergineDocument2 pagesMethergineRoseben SomidoNo ratings yet
- Drugs - OBDocument7 pagesDrugs - OBglennarthurNo ratings yet
- Drugs in ObgDocument41 pagesDrugs in ObgkishorNo ratings yet
- Pharmacotherapeutics in ObstetricsDocument14 pagesPharmacotherapeutics in ObstetricsmercyNo ratings yet
- Drugs Affecting The Myometrium (Stimulants and Relaxants of The Uterus)Document25 pagesDrugs Affecting The Myometrium (Stimulants and Relaxants of The Uterus)soumyajitchakraborty0238No ratings yet
- HORMONAL CONTRACEPTION PresentationDocument25 pagesHORMONAL CONTRACEPTION Presentationjaish8904No ratings yet
- DrugDocument11 pagesDrugrihamNo ratings yet
- Emergency Contraception: "The Morning-After Pill"Document24 pagesEmergency Contraception: "The Morning-After Pill"Dr. Sujnanendra MishraNo ratings yet
- Oxytocin and Other Drugs Acting On UterusDocument37 pagesOxytocin and Other Drugs Acting On UterusRamadi PrameelaNo ratings yet
- Drug StudyDocument14 pagesDrug StudyAthena Irish LastimosaNo ratings yet
- Maternity and Newborn MedicationsDocument38 pagesMaternity and Newborn MedicationsJaypee Fabros EdraNo ratings yet
- 1.7.1 Summary of Product Characteristics (SMPC)Document12 pages1.7.1 Summary of Product Characteristics (SMPC)ArebuNo ratings yet
- Contraception Part1Document38 pagesContraception Part1zianab aliNo ratings yet
- MCHN Popphi Amtsl Ref Man 2of3Document24 pagesMCHN Popphi Amtsl Ref Man 2of3Andhika Madang WijayaNo ratings yet
- Oral Hormonal Contraceptive: BY Magdyabdelrahmanmohamed 2 0 1 5Document36 pagesOral Hormonal Contraceptive: BY Magdyabdelrahmanmohamed 2 0 1 5UdtjeVanDerJeykNo ratings yet
- OB Drug ChartsDocument2 pagesOB Drug ChartsNursingSchoolNotesNo ratings yet
- ContraceptionDocument33 pagesContraceptionShams AtrashNo ratings yet
- OVARIAN STIMULANTS AND OXYTOCICS - PPTX - 22.04.2021 - Dr. SSDocument43 pagesOVARIAN STIMULANTS AND OXYTOCICS - PPTX - 22.04.2021 - Dr. SSRashitha NalarangaNo ratings yet
- Common Drugs During PregnancyDocument16 pagesCommon Drugs During Pregnancymdsoukar2000No ratings yet
- Drugs For GUTDocument11 pagesDrugs For GUTAyesha LiaqatNo ratings yet
- OB Drug StudyDocument19 pagesOB Drug StudyKismet Summons100% (8)
- Material ON Drugs Used IN ObstetricsDocument5 pagesMaterial ON Drugs Used IN ObstetricsMallika JoonNo ratings yet
- Drug StudyDocument34 pagesDrug StudyMarco MoralesNo ratings yet
- Drugs Producing Uterine CONTRACTIONS (Oxytocic Drugs) : Oxytocin Ergot Alkaloids ProstaglandinsDocument9 pagesDrugs Producing Uterine CONTRACTIONS (Oxytocic Drugs) : Oxytocin Ergot Alkaloids ProstaglandinsFaris Jamal Abu Za'nounehNo ratings yet
- Utrogestan Insert BelarusDocument4 pagesUtrogestan Insert BelarusLuni HaniaNo ratings yet
- Ceftriaxone, Misoprostol, OxytocinDocument4 pagesCeftriaxone, Misoprostol, OxytocinKrizia Bonilla100% (1)
- Active Management of 3RD Stage of LaborDocument7 pagesActive Management of 3RD Stage of LaborFarheen khanNo ratings yet
- Induction and AugmentationDocument23 pagesInduction and AugmentationMerry ZewduNo ratings yet
- Drugs Working On The UterusDocument28 pagesDrugs Working On The Uteruslinembambu1992No ratings yet
- Contraception and AbortionDocument20 pagesContraception and Abortiondaniel mitikuNo ratings yet
- Contraception: Heidery - Class DR. Hanaa Al 5 GynaecologyDocument11 pagesContraception: Heidery - Class DR. Hanaa Al 5 Gynaecologyzianab aliNo ratings yet
- 1-Drugs Affecting Uterine Muscle ContractilityDocument40 pages1-Drugs Affecting Uterine Muscle ContractilityjojolilimomoNo ratings yet
- Preterm Labor ManagementDocument50 pagesPreterm Labor ManagementDr-Firas Nayf Al-ThawabiaNo ratings yet
- Induction of LabourDocument20 pagesInduction of LabourNur Hanani Khan100% (1)
- Department of Pharmacy Practice Vels UniversityDocument29 pagesDepartment of Pharmacy Practice Vels UniversityUdtjeVanDerJeykNo ratings yet
- Inj. Ergometrine MaleatDocument17 pagesInj. Ergometrine MaleatAarti RajputNo ratings yet
- Summary of Product CharacteristicsDocument8 pagesSummary of Product CharacteristicsMirahAvishaNo ratings yet
- High Risk BabiesDocument44 pagesHigh Risk BabieskenmanikeseNo ratings yet
- God Is With UsDocument5 pagesGod Is With UskenmanikeseNo ratings yet
- Anatomy and Physiology IIDocument129 pagesAnatomy and Physiology IIkenmanikeseNo ratings yet
- AsthmaDocument31 pagesAsthmakenmanikeseNo ratings yet
- The Power of RepentanceDocument11 pagesThe Power of RepentancekenmanikeseNo ratings yet
- Nonadherence To Medications Among Persons With Bipolar Affective Disorder - A ReviewDocument9 pagesNonadherence To Medications Among Persons With Bipolar Affective Disorder - A ReviewIra DomunNo ratings yet
- CARDIAC EMERGENCIES IN DAILY PRACTICEDocument45 pagesCARDIAC EMERGENCIES IN DAILY PRACTICEnikenNo ratings yet
- Post-Cesarean Recovery Progress NotesDocument2 pagesPost-Cesarean Recovery Progress NotesJam JamaNo ratings yet
- Flower EsscencesDocument2 pagesFlower EsscencesDivyajyoti DevaNo ratings yet
- What Effects Do Smoking and DrinkingDocument8 pagesWhat Effects Do Smoking and DrinkingDulce M. LupaseNo ratings yet
- Ipcr Accomplishment June To Dec 2020Document3 pagesIpcr Accomplishment June To Dec 2020edwardraymond holl0% (1)
- Health - Lesson 1Document14 pagesHealth - Lesson 1annabel100% (1)
- Inhalation InjuriesDocument4 pagesInhalation InjuriesMohammadAwitNo ratings yet
- Hiv and Aids in Children3Document25 pagesHiv and Aids in Children3Kazau FwalangaNo ratings yet
- Assess Abdomen Percussion and PalpationDocument5 pagesAssess Abdomen Percussion and PalpationRatusweethella Intan Yudagrahania PuspitaNo ratings yet
- Infertility Questionnaire A. General InformationDocument4 pagesInfertility Questionnaire A. General InformationYogita DansenaNo ratings yet
- Veterinary Drug Formulary2014 English PDFDocument19 pagesVeterinary Drug Formulary2014 English PDFSamuel LamNo ratings yet
- ARTERISCLEROSISDocument46 pagesARTERISCLEROSISAdilla Edi AriefNo ratings yet
- H. PyloriDocument5 pagesH. PyloriWaleed El SaidNo ratings yet
- The Voice of PLC 1101Document6 pagesThe Voice of PLC 1101The Plymouth Laryngectomy ClubNo ratings yet
- Cardiac Sequential AnalysisDocument34 pagesCardiac Sequential AnalysisMochamad Rizky HendiperdanaNo ratings yet
- p214 PDFDocument3 pagesp214 PDFNinaNo ratings yet
- Pediatrics Lecture on Malnutrition Criteria and InterventionsDocument8 pagesPediatrics Lecture on Malnutrition Criteria and InterventionskrishNo ratings yet
- Lourdes College Nursing Program Drug StudyDocument2 pagesLourdes College Nursing Program Drug Studypinksapphire929100% (2)
- Budi Altgpt - Doc NewDocument3 pagesBudi Altgpt - Doc NewIrvanda ENVIOUSNo ratings yet
- Nursing Procedure Manual Nobel Medical College Teaching Hospital Biratnager, NepalDocument334 pagesNursing Procedure Manual Nobel Medical College Teaching Hospital Biratnager, NepalSweta ManandharNo ratings yet
- HLT32715 - Daily Lab Record - For Student & USBDocument4 pagesHLT32715 - Daily Lab Record - For Student & USBWafaa AdamNo ratings yet
- Comparison of ICD-10 and DSM-IV Criteria For Postconcussion SyndromedisorderDocument19 pagesComparison of ICD-10 and DSM-IV Criteria For Postconcussion Syndromedisorderneoraymix blackNo ratings yet
- GL On Pertussis Case ManagementDocument32 pagesGL On Pertussis Case Managementnazurah HamidNo ratings yet
- Preguntas de Investigación Priorizadas en Salud Mental PDFDocument10 pagesPreguntas de Investigación Priorizadas en Salud Mental PDFMatiasZambranoCNo ratings yet
- What Are The Challenges of Working With Mentally Ill Mothers Jerina SpicerDocument19 pagesWhat Are The Challenges of Working With Mentally Ill Mothers Jerina Spicerjerina spicerNo ratings yet
- Exam 3 lv4Document4 pagesExam 3 lv4Omph IcuNo ratings yet
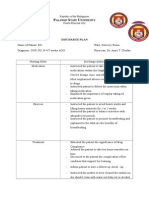
- Discharge Plan: Alawan Tate NiversityDocument2 pagesDischarge Plan: Alawan Tate NiversityLenieGracePascoNo ratings yet
- CosmetovigilentaDocument29 pagesCosmetovigilentaChiorean Ioana100% (1)
- NeuropsychiatricDocument18 pagesNeuropsychiatricSamuel JohnsonNo ratings yet