You might also like
- EmocDocument39 pagesEmocSarahNo ratings yet
- Cardiovascular Disorders and PregnancyDocument30 pagesCardiovascular Disorders and PregnancyAngelie RojasNo ratings yet
- Cardiovascular Disorders in PregnancyDocument55 pagesCardiovascular Disorders in PregnancyRyrey Abraham PacamanaNo ratings yet
- CARDIAC DISEASE IN PREGNANCY-2Document24 pagesCARDIAC DISEASE IN PREGNANCY-2Gladys OdibuNo ratings yet
- Heart and Thyroid Disease Seminar YesDocument32 pagesHeart and Thyroid Disease Seminar YesGoh Saw HuanNo ratings yet
- Unit 4, Chapter 20 UnfinishedDocument16 pagesUnit 4, Chapter 20 Unfinishedcutiepie creampieNo ratings yet
- NURS325 05 Antepartum ComplicationDocument81 pagesNURS325 05 Antepartum ComplicationaliNo ratings yet
- 1 Nursing Care of The Pregnant Client Pre Gestational ConditionDocument134 pages1 Nursing Care of The Pregnant Client Pre Gestational ConditionVince MatthewNo ratings yet
- Hypertension in PregnancyDocument8 pagesHypertension in PregnancyHannrhey VelascoNo ratings yet
- Minor Body Changes of PregnancyDocument41 pagesMinor Body Changes of Pregnancyraquel maniegoNo ratings yet
- Hyperemesis Gravidarum AnemiaDocument10 pagesHyperemesis Gravidarum AnemiaKate SantosNo ratings yet
- Case Presentation: Congenital Heart DiseaseDocument37 pagesCase Presentation: Congenital Heart DiseaseKarin Nadia UtamiNo ratings yet
- NRG 204 - Pre-Gestational ConditionsDocument66 pagesNRG 204 - Pre-Gestational ConditionsPRINCE PHILIP SAGUIGUITNo ratings yet
- MCN2 Lesson 1.2 - High Risk Pregnancy Pre-Ecisting and Acquired ConditionsDocument146 pagesMCN2 Lesson 1.2 - High Risk Pregnancy Pre-Ecisting and Acquired ConditionsErica Veluz LuyunNo ratings yet
- Simulation PaperworkDocument5 pagesSimulation Paperworkjustgraduate1408100% (1)
- Emergency Care of Pregnant PatientDocument16 pagesEmergency Care of Pregnant PatientAshraf QotmoshNo ratings yet
- Management of Pregnant PatientDocument113 pagesManagement of Pregnant PatientWilliam BharathNo ratings yet
- Complications of 2nd TrimesterDocument34 pagesComplications of 2nd TrimesterMA. JYRELL BONITONo ratings yet
- Abnormal Pregnancy: Prepared by Yeshi Assefa (MSC, BSC, R/N) March/2021Document34 pagesAbnormal Pregnancy: Prepared by Yeshi Assefa (MSC, BSC, R/N) March/2021Cheru DugaseNo ratings yet
- Other Intrapartum Complications 2022Document40 pagesOther Intrapartum Complications 2022Nikky SilvestreNo ratings yet
- What is PIH? Understanding Pregnancy Induced HypertensionDocument28 pagesWhat is PIH? Understanding Pregnancy Induced HypertensionMicah MagallanoNo ratings yet
- Managing Cardiac Disease in Labor, Delivery and the Postpartum PeriodDocument6 pagesManaging Cardiac Disease in Labor, Delivery and the Postpartum PeriodHassan osmanNo ratings yet
- Managing Obstetric Emergencies: Hemorrhage, Fetal Distress and Non-Reassuring TracingsDocument26 pagesManaging Obstetric Emergencies: Hemorrhage, Fetal Distress and Non-Reassuring TracingsrahulthedrNo ratings yet
- Dic PihDocument82 pagesDic PihMatth N. ErejerNo ratings yet
- Obstructed LabourDocument24 pagesObstructed LabourNatukunda Dianah50% (4)
- What The Bleep?: Common Calls For Junior Doctors in O&G DR Alice KnowlesDocument43 pagesWhat The Bleep?: Common Calls For Junior Doctors in O&G DR Alice KnowlesAlice KnowlesNo ratings yet
- Abnormal Progress in Labor (Precipitous Labor and Birth & Retraction Rings)Document34 pagesAbnormal Progress in Labor (Precipitous Labor and Birth & Retraction Rings)Ana100% (3)
- Hyperemesis Gravidarum AnemiaDocument7 pagesHyperemesis Gravidarum AnemiaAntonette CedroNo ratings yet
- NCM 109 - Week 1Document6 pagesNCM 109 - Week 1Aly HannahNo ratings yet
- Critical Care in Pregnancy - Dr. Suparto 2020Document21 pagesCritical Care in Pregnancy - Dr. Suparto 2020xiao chiengNo ratings yet
- Antepartum HemorrhageDocument30 pagesAntepartum HemorrhageNatukunda DianahNo ratings yet
- Hypertensive Disorders of PregnancyDocument46 pagesHypertensive Disorders of PregnancyJagadeeswari JayaseelanNo ratings yet
- Labor and Delivery NoteDocument26 pagesLabor and Delivery NoteyagyaNo ratings yet
- Nursing Care OF A Family Experiencing A Pregnancy From A Preexisting OR Newly Acquired IllnessDocument55 pagesNursing Care OF A Family Experiencing A Pregnancy From A Preexisting OR Newly Acquired IllnessJohn Van Dave TaturoNo ratings yet
- COMPLICATIONS OF PREGNANCY - pptx1Document23 pagesCOMPLICATIONS OF PREGNANCY - pptx1Zaroon Abdullah KhanNo ratings yet
- Uterine RuptureDocument19 pagesUterine RuptureAna Denise Quinajon0% (1)
- Nursing Care of High-Risk Pregnant ClientsDocument6 pagesNursing Care of High-Risk Pregnant ClientsFaith Calimlim100% (1)
- Nursing Care of High-Risk Prenatal Clients with Cardiac DiseasesDocument22 pagesNursing Care of High-Risk Prenatal Clients with Cardiac DiseasesMaria Pina Barbado PonceNo ratings yet
- AFE, RUPTURE OF UTERUS, (Autosaved)Document31 pagesAFE, RUPTURE OF UTERUS, (Autosaved)maezu100% (1)
- Obstetrical HemorrhageDocument76 pagesObstetrical HemorrhagejarssooNo ratings yet
- Complication of PregnancyDocument44 pagesComplication of PregnancyJharaNo ratings yet
- Cardio Vascular Disease in PregnancyDocument57 pagesCardio Vascular Disease in PregnancySanthosh.S.U0% (1)
- MaeDocument9 pagesMaeCharmaigne Mae Padilla Sotelo100% (1)
- Hypertension During PregnancyDocument33 pagesHypertension During PregnancyHanna DadacayNo ratings yet
- Heart Disease To STDDocument7 pagesHeart Disease To STDCURT JAZTYN PASCUALNo ratings yet
- Labor&DeliveryDocument8 pagesLabor&Deliverytomrey1533No ratings yet
- Ectopic Pregnancy Risks and SymptomsDocument17 pagesEctopic Pregnancy Risks and Symptomsdanica grace gubaNo ratings yet
- Antenatal Obstetric ComplicationsDocument43 pagesAntenatal Obstetric Complicationsmalaika khanNo ratings yet
- Rare Childbirth Emergency: Amniotic Fluid EmbolismDocument5 pagesRare Childbirth Emergency: Amniotic Fluid EmbolismPatel AmeeNo ratings yet
- hypertensive disorders of pregnancyDocument32 pageshypertensive disorders of pregnancySingitan SiyoumNo ratings yet
- MCHN PDFDocument11 pagesMCHN PDFJAHNYNE FAITH MA�ALACNo ratings yet
- System Wise Physiological ChangesDocument24 pagesSystem Wise Physiological ChangesKinjal VasavaNo ratings yet
- By: Darryl Jamison Macon County EMS Training CoordinatorDocument27 pagesBy: Darryl Jamison Macon County EMS Training Coordinatorputri azzahraNo ratings yet
- Heart Disease and PrenancyDocument24 pagesHeart Disease and PrenancyzizsatriaNo ratings yet
- Chronic Hypertension During Pregnancy.: Dr. Eman S. Radwan. 2 Year Resident in Obstetrics and GynecologyDocument25 pagesChronic Hypertension During Pregnancy.: Dr. Eman S. Radwan. 2 Year Resident in Obstetrics and GynecologyMaisara Al HadidiNo ratings yet
- Beginning of Chapter 2Document4 pagesBeginning of Chapter 2eirelav0902No ratings yet
- Discomforts of Middle To Late PregnancyDocument18 pagesDiscomforts of Middle To Late PregnancyMonique ReyesNo ratings yet
- Pre-eclampsia, (Pregnancy with Hypertension And Proteinuria) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandPre-eclampsia, (Pregnancy with Hypertension And Proteinuria) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Mitral Valve Regurgitation, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandMitral Valve Regurgitation, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- FormsDocument5 pagesFormsMatth N. ErejerNo ratings yet
- Biological MoleculesDocument5 pagesBiological MoleculesMatth N. ErejerNo ratings yet
- Daliton-Uts4 AnswersDocument3 pagesDaliton-Uts4 AnswersMatth N. ErejerNo ratings yet
- Changing and Discontinuing of IVFDocument1 pageChanging and Discontinuing of IVFMatth N. ErejerNo ratings yet
- Application of TravelbeeDocument1 pageApplication of TravelbeeMatth N. ErejerNo ratings yet
- Cell TheoryDocument3 pagesCell TheoryMatth N. ErejerNo ratings yet
- Cellular RespirationDocument6 pagesCellular RespirationMatth N. ErejerNo ratings yet
- Metronidazole DrugDocument1 pageMetronidazole DrugMatth N. ErejerNo ratings yet
- Slide 5 Cystic Fibrosis Mental IllnessDocument40 pagesSlide 5 Cystic Fibrosis Mental IllnessMatth N. ErejerNo ratings yet
- Clarithromycin DrugDocument1 pageClarithromycin DrugMatth N. ErejerNo ratings yet
- Dic PihDocument82 pagesDic PihMatth N. ErejerNo ratings yet
- Bacteria1 LecDocument7 pagesBacteria1 LecYezza Mae D. LucbanNo ratings yet
- Facilitating of Learning JunDocument12 pagesFacilitating of Learning JunMatth N. ErejerNo ratings yet
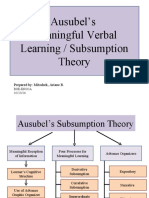
- Ausubel TheoryDocument13 pagesAusubel TheoryChristopher Arellano33% (3)
- Caber Human Environmental Factors Affecting MotivationDocument6 pagesCaber Human Environmental Factors Affecting MotivationMatth N. ErejerNo ratings yet
- Essential Intrapartum and Newborn CareDocument37 pagesEssential Intrapartum and Newborn CareVenice s SantosNo ratings yet
- Assessment of Pregnant WomanDocument6 pagesAssessment of Pregnant WomanKYLE SABAY100% (1)
- 757Document46 pages757David DavidNo ratings yet
- OBG-GYN Practice QuestionsDocument222 pagesOBG-GYN Practice QuestionsRizwanNo ratings yet
- Danger Signs in Pregnancy Teaching PlanDocument6 pagesDanger Signs in Pregnancy Teaching PlanEn George88% (8)
- 36 - Acute Inversion of The UterusDocument10 pages36 - Acute Inversion of The Uterusdr_asaleh100% (1)
- Community Resource ListDocument6 pagesCommunity Resource Listapi-240620529No ratings yet
- Retained Placenta and Postpartum Hemorrhage: Time Is Not EverythingDocument9 pagesRetained Placenta and Postpartum Hemorrhage: Time Is Not EverythingWalid AsyhariNo ratings yet
- Stages of LaborDocument15 pagesStages of LaborlumpiaNo ratings yet
- Cervical Pessary in Prevention of Preterm BirthDocument6 pagesCervical Pessary in Prevention of Preterm BirthAlessandra CruzNo ratings yet
- Vbac Royal CollegDocument31 pagesVbac Royal CollegBangun Said Santoso100% (1)
- Your Travel Insurance Policy: Reference Number: Insurefor/EA/2009 09IST, 09ISA & 09ISEDocument12 pagesYour Travel Insurance Policy: Reference Number: Insurefor/EA/2009 09IST, 09ISA & 09ISEOmar DahouNo ratings yet
- Antenatal CareDocument13 pagesAntenatal CareOjambo Flavia50% (2)
- To determine the gestational age based on herlast menstrual period. By knowing the date of her lastmenstrual period, we can estimate how far along in herpregnancy she might beDocument47 pagesTo determine the gestational age based on herlast menstrual period. By knowing the date of her lastmenstrual period, we can estimate how far along in herpregnancy she might bediza hanniNo ratings yet
- Practical BookDocument129 pagesPractical BookAndrew AhimbisibweNo ratings yet
- Ob Post TestDocument12 pagesOb Post TestMho Pimentel VanguardiaNo ratings yet
- PHENYLKETONURIADocument3 pagesPHENYLKETONURIAMiwa IshiiNo ratings yet
- Leopold's ManeuverDocument3 pagesLeopold's ManeuverPekabuNo ratings yet
- Ruptured Uterus 5.0finalDocument12 pagesRuptured Uterus 5.0finalkalpana gondipalliNo ratings yet
- Mother's Class ExerciseDocument40 pagesMother's Class ExerciseRA TranceNo ratings yet
- Pediatric Soap NotesDocument8 pagesPediatric Soap Noteskenata100% (1)
- Who Emt Mds CriteriaDocument2 pagesWho Emt Mds CriteriaClarissaNo ratings yet
- Obs Moses KazevuDocument285 pagesObs Moses KazevuChilufya KalasaNo ratings yet
- Postpartum Depression (PPD) : Sara Thurgood, BS Daniel M. Avery, MD Lloyda Williamson, MDDocument9 pagesPostpartum Depression (PPD) : Sara Thurgood, BS Daniel M. Avery, MD Lloyda Williamson, MDTimmy LarasatiNo ratings yet
- Ncma219 Course Task 3Document18 pagesNcma219 Course Task 3NikoruNo ratings yet
- Example 1: Application LetterDocument2 pagesExample 1: Application LetterYulinar MashuriNo ratings yet
- RD ManualDocument6 pagesRD Manualapple m.No ratings yet
- Family Nursing Care Plan ModuleDocument16 pagesFamily Nursing Care Plan ModuleHarlene Joyce ReyNo ratings yet
- PNC CareDocument2 pagesPNC CareAparna ChoudhuryNo ratings yet
- Asthma in Pregnancy: Dr. Agus Rusdhy Hariawan Hamid, Spog SMF Obgin Rsup NTBDocument10 pagesAsthma in Pregnancy: Dr. Agus Rusdhy Hariawan Hamid, Spog SMF Obgin Rsup NTBMartina RizkiNo ratings yet