You might also like
- The Problem Oriented Medical RecordDocument32 pagesThe Problem Oriented Medical RecordPriscila TanuwidjajaNo ratings yet
- CQ3 - Royal Collegue PDFDocument529 pagesCQ3 - Royal Collegue PDFJohanna Rodriguez RobayoNo ratings yet
- Hypertension Disorder in PregnancyDocument42 pagesHypertension Disorder in Pregnancyholly girlchy JastinNo ratings yet
- Organization of The Human BodyDocument8 pagesOrganization of The Human BodyAly HannahNo ratings yet
- PIHDocument4 pagesPIHCatherine PradoNo ratings yet
- Emergency Obstetrics2Document105 pagesEmergency Obstetrics2Alphine DalgoNo ratings yet
- Eclampsia Pre EclampsiaDocument3 pagesEclampsia Pre EclampsiaOona Nicole Diorico100% (2)
- Lead and Lead Poisoning From Antiquity To Modern TimesDocument7 pagesLead and Lead Poisoning From Antiquity To Modern Timesgheijo100% (1)
- PihDocument35 pagesPihmark100% (6)
- Cardiovascular Disorders & PregnancyDocument6 pagesCardiovascular Disorders & PregnancyChelcee MagsinoNo ratings yet
- Hesi Exam Practice Pharmacology PDFDocument55 pagesHesi Exam Practice Pharmacology PDFAna Bienne100% (2)
- Dysphagia, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandDysphagia, A Simple Guide To The Condition, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (1)
- Drugs in SportsDocument32 pagesDrugs in SportsBerlin AlonzoNo ratings yet
- NCM 109 ReviewerDocument8 pagesNCM 109 ReviewerAlma Janella TOSINO100% (2)
- Advance Practice in Maternal and Child Nursing 1 High Risk Pregnancy: Nursing Care of A Family Experiencing A Pregnancy Complication From A Pre-Existing or Newly Acquired IllnessDocument31 pagesAdvance Practice in Maternal and Child Nursing 1 High Risk Pregnancy: Nursing Care of A Family Experiencing A Pregnancy Complication From A Pre-Existing or Newly Acquired Illnessallanrnmanaloto100% (2)
- Abruptio Placenta and AbortionDocument10 pagesAbruptio Placenta and Abortiondanica grace gubaNo ratings yet
- Pre-eclampsia, (Pregnancy with Hypertension And Proteinuria) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandPre-eclampsia, (Pregnancy with Hypertension And Proteinuria) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Pathological ObDocument43 pagesPathological ObMatth N. ErejerNo ratings yet
- Pregestational ConditionsDocument10 pagesPregestational Conditionsevangelistakatrina523No ratings yet
- Chronic Hypertension During Pregnancy.: Dr. Eman S. Radwan. 2 Year Resident in Obstetrics and GynecologyDocument25 pagesChronic Hypertension During Pregnancy.: Dr. Eman S. Radwan. 2 Year Resident in Obstetrics and GynecologyMaisara Al HadidiNo ratings yet
- Hypertension During PregnancyDocument33 pagesHypertension During PregnancyHanna DadacayNo ratings yet
- Dic PihDocument82 pagesDic PihMatth N. ErejerNo ratings yet
- COMPLICATIONS OF PREGNANCY - pptx1Document23 pagesCOMPLICATIONS OF PREGNANCY - pptx1Zaroon Abdullah KhanNo ratings yet
- 12 - Jhasnu 19 007Document3 pages12 - Jhasnu 19 007Dila AuNo ratings yet
- APH PresentationDocument42 pagesAPH Presentationestela aberaNo ratings yet
- Labor&DeliveryDocument8 pagesLabor&Deliverytomrey1533No ratings yet
- NCM 109 High Risk PregnancyDocument11 pagesNCM 109 High Risk PregnancyLea BorceNo ratings yet
- Module 3 - Maternal TransesDocument7 pagesModule 3 - Maternal TransesCarl UyNo ratings yet
- Gestational 1Document8 pagesGestational 1RoseAngelyne VicenteNo ratings yet
- High Risk PregnancyDocument4 pagesHigh Risk PregnancyCrisheila Sarah PiedadNo ratings yet
- Nursing Care of Pregnant Client - Doc Tinagan DiscussionDocument8 pagesNursing Care of Pregnant Client - Doc Tinagan DiscussionshainakyllebarbonNo ratings yet
- Hypertensive Disorders of PregnancyDocument32 pagesHypertensive Disorders of PregnancySingitan SiyoumNo ratings yet
- Heart and Thyroid Disease Seminar YesDocument32 pagesHeart and Thyroid Disease Seminar YesGoh Saw HuanNo ratings yet
- Simulation PaperworkDocument5 pagesSimulation Paperworkjustgraduate1408100% (1)
- Postnatal LeafletDocument2 pagesPostnatal LeafletAnonymous miY5zfHNo ratings yet
- MCN ReviewerDocument4 pagesMCN ReviewerMaria Arabella LanacaNo ratings yet
- S1 5 OB Lec Nursing Care of The Pregnant Client Pre Gestational ConditionDocument132 pagesS1 5 OB Lec Nursing Care of The Pregnant Client Pre Gestational ConditionJustine Ingrid O. FernandezNo ratings yet
- Task 1 PIH and Heart Disease During PregnancyDocument5 pagesTask 1 PIH and Heart Disease During Pregnancyrobertvaliente471No ratings yet
- Module 2 - MCN TransesDocument6 pagesModule 2 - MCN TransesCarl UyNo ratings yet
- APH&PPHDocument77 pagesAPH&PPHKåbåñå TürüñåNo ratings yet
- Management of Cardiac Disease in LaborDocument6 pagesManagement of Cardiac Disease in LaborHassan osmanNo ratings yet
- EmocDocument39 pagesEmocSarahNo ratings yet
- Hypertensive Disorders of PregnancyDocument8 pagesHypertensive Disorders of PregnancyHannrhey VelascoNo ratings yet
- Module 2 - Maternal TransesDocument6 pagesModule 2 - Maternal TransesCarl UyNo ratings yet
- Ward Class - PCI, HPN DX in PregnancyDocument26 pagesWard Class - PCI, HPN DX in Pregnancyhrry stylesNo ratings yet
- Hypertensive Disorder in PregnantDocument41 pagesHypertensive Disorder in PregnantMRT RadiologyNo ratings yet
- Guidelines For The Management of Hypertensive Disorders of Pregnancy 2008Document5 pagesGuidelines For The Management of Hypertensive Disorders of Pregnancy 2008Firah Triple'sNo ratings yet
- Pregnancy HypertensionDocument71 pagesPregnancy Hypertensionbazuu mbwegzeNo ratings yet
- Preeclampsia: Team Poli RSCMDocument35 pagesPreeclampsia: Team Poli RSCMbenediktus danangNo ratings yet
- Cardiac Disease in Pregnancy-2Document24 pagesCardiac Disease in Pregnancy-2Gladys OdibuNo ratings yet
- Pre EclampsiaDocument11 pagesPre EclampsiaAkinsoun MotunrayoNo ratings yet
- NMT 06101: Care of A Woman With Obstetric Emergency ConditionsDocument10 pagesNMT 06101: Care of A Woman With Obstetric Emergency ConditionsWILBARD JOACHIMNo ratings yet
- Maternal Reviewer FinalsDocument36 pagesMaternal Reviewer FinalsHannah QuindipanNo ratings yet
- 2F Compiled Oral Revalida 1Document75 pages2F Compiled Oral Revalida 1Mary Loise VillegasNo ratings yet
- CA MaternalDocument156 pagesCA MaternalLovely Hope LugatimanNo ratings yet
- Nursing Care of Mother With Complications During PregnancyDocument32 pagesNursing Care of Mother With Complications During Pregnancydad112389No ratings yet
- Perdarahan Antepartum - EmiliaDocument26 pagesPerdarahan Antepartum - EmiliaEmilia NazmaNo ratings yet
- Slide 5 Cystic Fibrosis Mental IllnessDocument40 pagesSlide 5 Cystic Fibrosis Mental IllnessMatth N. ErejerNo ratings yet
- Early Pregnancy ComplicationDocument31 pagesEarly Pregnancy ComplicationHizami NorddinNo ratings yet
- By: Darryl Jamison Macon County EMS Training CoordinatorDocument27 pagesBy: Darryl Jamison Macon County EMS Training Coordinatorputri azzahraNo ratings yet
- Summary Concepts: Complications of PregnancyDocument2 pagesSummary Concepts: Complications of Pregnancyvia macarioNo ratings yet
- Acute Renal Failure in Pregnancy: Additional Professor Obstetrics and Gynaecology Aiims BhubaneswarDocument25 pagesAcute Renal Failure in Pregnancy: Additional Professor Obstetrics and Gynaecology Aiims BhubaneswarSharoon KumarNo ratings yet
- Hypertensive Disease in Pregnancy: A. Kurdi SyamsuriDocument42 pagesHypertensive Disease in Pregnancy: A. Kurdi SyamsuriBilly DarismaNo ratings yet
- Pregnancy ComplicationsDocument14 pagesPregnancy ComplicationsespantojoannamerielNo ratings yet
- Preexisting or Newly Acquired IllnessDocument26 pagesPreexisting or Newly Acquired IllnessCreciabullecerNo ratings yet
- Complications of 2nd TrimesterDocument34 pagesComplications of 2nd TrimesterMA. JYRELL BONITONo ratings yet
- Urinary SystemDocument10 pagesUrinary SystemAly HannahNo ratings yet
- Quantum NumbersDocument4 pagesQuantum NumbersAly HannahNo ratings yet
- Organic Compounds S3Document34 pagesOrganic Compounds S3Aly HannahNo ratings yet
- CardioDocument9 pagesCardioAly HannahNo ratings yet
- Leopold ManeuverDocument10 pagesLeopold ManeuverAly HannahNo ratings yet
- Magnetic PropertiesDocument3 pagesMagnetic PropertiesAly HannahNo ratings yet
- Quantum Numbers S3Document16 pagesQuantum Numbers S3Aly HannahNo ratings yet
- Chemical BondingDocument17 pagesChemical BondingAly HannahNo ratings yet
- IsomersDocument15 pagesIsomersAly HannahNo ratings yet
- IMF Liquids and SolidsDocument29 pagesIMF Liquids and SolidsAly HannahNo ratings yet
- Dalton Graham Gas LawsDocument16 pagesDalton Graham Gas LawsAly HannahNo ratings yet
- Combined & Ideal Gas LawDocument12 pagesCombined & Ideal Gas LawAly HannahNo ratings yet
- Mole ConceptDocument5 pagesMole ConceptAly HannahNo ratings yet
- AtomsDocument8 pagesAtomsAly HannahNo ratings yet
- Electron Configuration & Orbital DiagramDocument3 pagesElectron Configuration & Orbital DiagramAly HannahNo ratings yet
- Respiratory SystemDocument13 pagesRespiratory SystemAly HannahNo ratings yet
- Lymphatic SystemDocument10 pagesLymphatic SystemAly HannahNo ratings yet
- Nervous SystemDocument3 pagesNervous SystemAly HannahNo ratings yet
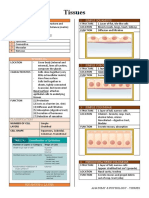
- TissuesDocument4 pagesTissuesAly HannahNo ratings yet
- Blood VesselsDocument5 pagesBlood VesselsAly HannahNo ratings yet
- 11.fatty Liver DiseaseDocument5 pages11.fatty Liver DiseaseSubhi MishraNo ratings yet
- Nutrition Care ProcessDocument44 pagesNutrition Care ProcessKATH GONo ratings yet
- Chordal Preservation During Mitral Valve Replacement: Basis, Techniques and ResultsDocument9 pagesChordal Preservation During Mitral Valve Replacement: Basis, Techniques and ResultsThanh BinhNo ratings yet
- Medication: Expected Pharmacological Action Therapeutic UseDocument1 pageMedication: Expected Pharmacological Action Therapeutic UseMike EveretteNo ratings yet
- Muntingia Calabura A Review On Its TradiDocument67 pagesMuntingia Calabura A Review On Its TradiAhmad Anas Nagoor GunnyNo ratings yet
- OsteoporoseDocument54 pagesOsteoporoseJandui DinizNo ratings yet
- Eugenio NCP 2Document2 pagesEugenio NCP 2Bethrice MelegritoNo ratings yet
- Occupational Health Lectures 2009.student - ModifiedDocument68 pagesOccupational Health Lectures 2009.student - ModifiedAdewumi Ebenezer Oluwapelumi0% (1)
- HMS - Women's Health (MCQ & Notes)Document44 pagesHMS - Women's Health (MCQ & Notes)marouf elgoulNo ratings yet
- Sural Nerve BiopsyDocument2 pagesSural Nerve BiopsyArindam MukherjeeNo ratings yet
- FINAL-EXAM-level-Vi DESARROLLADODocument5 pagesFINAL-EXAM-level-Vi DESARROLLADOEmerzon GuevaraNo ratings yet
- Residual Limb Complications and Management StrategiesDocument9 pagesResidual Limb Complications and Management StrategiesTarushi TanwarNo ratings yet
- Rajiv Gandhi University of Health Sciences, KarnatakaDocument16 pagesRajiv Gandhi University of Health Sciences, KarnatakaSanthana PriyaNo ratings yet
- Genetic Counselling AssignmentDocument3 pagesGenetic Counselling Assignmentjyoti singhNo ratings yet
- West Bengal COVID-19 RestrictionsDocument2 pagesWest Bengal COVID-19 RestrictionsNDTV80% (10)
- Results: Final QuizDocument4 pagesResults: Final QuizChö Häche SantanäNo ratings yet
- A Review On Influence of Ahara Diet On Mental HealDocument4 pagesA Review On Influence of Ahara Diet On Mental HealPablo M. MauroNo ratings yet
- CPH AssignmentDocument3 pagesCPH AssignmentChrystelle Mariano TibayNo ratings yet
- Analytical ExpositionDocument5 pagesAnalytical ExpositionMuhammad Rafi AldianzaNo ratings yet
- Keamanan Pangan Hasil PerikananDocument42 pagesKeamanan Pangan Hasil PerikananBhatara Ayi MeataNo ratings yet
- Genitourinary PharmacologyDocument11 pagesGenitourinary PharmacologySadia YousafNo ratings yet
- Case Study No.8Document7 pagesCase Study No.8Tahira Zehra0% (1)
- CHN Day 2Document12 pagesCHN Day 2Enrico LavariasNo ratings yet
- Trochlearnerve 180712145548Document39 pagesTrochlearnerve 180712145548Mv.suravijay Mv.suravijayNo ratings yet
- GlobalFund HealthFinancingPolicyBrief Ethiopia Palladium FinalMar2019 - 2Document36 pagesGlobalFund HealthFinancingPolicyBrief Ethiopia Palladium FinalMar2019 - 2Estalew YalewNo ratings yet