You might also like
- Care of The Mother and The Fetus During The Perinatal PeriodDocument22 pagesCare of The Mother and The Fetus During The Perinatal PeriodRoshin Tejero100% (1)
- Lec 7 Prenatal CareDocument58 pagesLec 7 Prenatal CareCarmel CochingNo ratings yet
- Pre Natal Care 2Document19 pagesPre Natal Care 2Isha Catimbang GenerilloNo ratings yet
- Care of The Woman During PregnancyDocument99 pagesCare of The Woman During PregnancyFrancr ToledanoNo ratings yet
- NCM 107 NotesDocument29 pagesNCM 107 NotesKryza CastilloNo ratings yet
- Prenatal CareDocument57 pagesPrenatal CareJunry PilapilNo ratings yet
- MCN Skills Lab 2021Document25 pagesMCN Skills Lab 2021irene mancaoNo ratings yet
- MCHN Prenatal CareDocument69 pagesMCHN Prenatal CareLEBADISOS KATE PRINCESSNo ratings yet
- PregnancyDocument32 pagesPregnancyAllyah Anthonette FerweloNo ratings yet
- MCN Rle Lesson 1Document3 pagesMCN Rle Lesson 1Joeyca Shien PiolNo ratings yet
- Obstetrics History TakingDocument3 pagesObstetrics History TakingYavani KulasinghamNo ratings yet
- Combined Ob I and IIDocument2,079 pagesCombined Ob I and IIAmanuelNo ratings yet
- CH 14 Antepartum Nursing Assessment NotesDocument8 pagesCH 14 Antepartum Nursing Assessment NotesMary LowryNo ratings yet
- Ritah's Very Reproductive Health PortifolioDocument18 pagesRitah's Very Reproductive Health PortifolioDerick AaronNo ratings yet
- Prenatal CareDocument5 pagesPrenatal CareJoshua AysonNo ratings yet
- Care of Mother (Lab) TransDocument89 pagesCare of Mother (Lab) TransHANNA FRANCESCA CORPUZNo ratings yet
- Establishing Pregnancy PDFDocument6 pagesEstablishing Pregnancy PDFShemess ButgorgNo ratings yet
- UZ MaternalFetalAssessment FaidangDocument65 pagesUZ MaternalFetalAssessment FaidangMamor MutalibNo ratings yet
- NCM 107a Care of The Pregnant WomanDocument43 pagesNCM 107a Care of The Pregnant WomanMelchizedek Tagarino Torio100% (1)
- Assessment of The Childbearing Woman ReviewerDocument10 pagesAssessment of The Childbearing Woman ReviewerLaurisse April NecesitoNo ratings yet
- OBST 7010 Quiz 2 Review (Swan) : Week 2 - Antepartum CareDocument6 pagesOBST 7010 Quiz 2 Review (Swan) : Week 2 - Antepartum CareBridget MasonNo ratings yet
- Ateneo de Zamboanga University: College of Nursing Level 2Document7 pagesAteneo de Zamboanga University: College of Nursing Level 2Sheryhan Tahir BayleNo ratings yet
- Safe Motherhood ANCDocument51 pagesSafe Motherhood ANCAsad ullah100% (1)
- The Prenatal CareDocument10 pagesThe Prenatal CareDONITA DALUMPINESNo ratings yet
- Care of Mother, Child or Family (RLE) - REVIEWER #1Document4 pagesCare of Mother, Child or Family (RLE) - REVIEWER #1rocket12shipsNo ratings yet
- Prenatalf EFewfw EFWDocument52 pagesPrenatalf EFewfw EFWJoshua Isiah S. LumapasNo ratings yet
- Makalah PBL Blok 13 Skenario 1Document17 pagesMakalah PBL Blok 13 Skenario 1BIntangsinagaNo ratings yet
- Pedia AssessmentDocument15 pagesPedia AssessmentCezanne HutallaNo ratings yet
- Antenatal Power PointDocument135 pagesAntenatal Power PointBULARON, Gerry Mar ANo ratings yet
- Ob Evaluation 2 Final - Sec ADocument35 pagesOb Evaluation 2 Final - Sec AKarla Mae Israel CamarintaNo ratings yet
- 2M Di Ayos Table of ContentsDocument114 pages2M Di Ayos Table of ContentsRolland Ray MendozaNo ratings yet
- History Clerking, Physical Examination of Obstetrics PatientsDocument9 pagesHistory Clerking, Physical Examination of Obstetrics PatientsCk Kma0% (1)
- Case Study 114: ScenarioDocument4 pagesCase Study 114: ScenarioPrincess Levie CenizaNo ratings yet
- Multifetal Gestation Case StudyDocument67 pagesMultifetal Gestation Case StudyNikki Joy NavarroNo ratings yet
- Maternal NSG ProceduresDocument18 pagesMaternal NSG ProceduresGARCIA, KYLA MAE A.No ratings yet
- Assessment of Fetal Growth and DevelopmentDocument10 pagesAssessment of Fetal Growth and DevelopmentAira Jane BasuelNo ratings yet
- Fundic HeightDocument37 pagesFundic HeightJanel PinuelaNo ratings yet
- Case ScenarioDocument3 pagesCase ScenarioCathy Marie Constante100% (1)
- Tumbuh Kembang - Steven L SantosoDocument28 pagesTumbuh Kembang - Steven L SantosoAndri OnnadioNo ratings yet
- ANC OB and GYN HISTORY Taking SampleDocument43 pagesANC OB and GYN HISTORY Taking SampleGebremichael Reta100% (3)
- Chapter 007Document29 pagesChapter 007Charm TanyaNo ratings yet
- 1 Obstetrical HistoryDocument5 pages1 Obstetrical HistoryNilofar SadiqNo ratings yet
- Antepartal CareDocument9 pagesAntepartal CareChristopher R. Bañez-Full Account100% (1)
- Ob-Gy HX & P-EDocument83 pagesOb-Gy HX & P-Emaezu100% (2)
- ASUHAN KEBIDANAN KEHAMILAN PKKBDocument12 pagesASUHAN KEBIDANAN KEHAMILAN PKKBInggrit Novisari RatuNo ratings yet
- Prenatal MGTDocument16 pagesPrenatal MGTClairie Jhane ClaorNo ratings yet
- MCN Case Study-2pDocument76 pagesMCN Case Study-2pAngeline ShackletonNo ratings yet
- AntepartalDocument27 pagesAntepartalaliehso100% (1)
- Anc 1 2 1Document22 pagesAnc 1 2 1Lemma AbishaNo ratings yet
- ANTENATAL CARE Translate GooglingDocument26 pagesANTENATAL CARE Translate GooglingLutfi ari206100% (2)
- BastaaDocument9 pagesBastaajohncarlo ramosNo ratings yet
- Maternal Assessment: History TakingDocument18 pagesMaternal Assessment: History TakingSirisha ChelvaNo ratings yet
- Gynacology and Obstetrics Format For History & Physical ExaminaitonDocument13 pagesGynacology and Obstetrics Format For History & Physical ExaminaitonBayisa GirmaNo ratings yet
- IntroductionDocument7 pagesIntroductionJana MasharqahNo ratings yet
- Maternal and Child Summary NotesDocument25 pagesMaternal and Child Summary Notesrossinniblue.protacioNo ratings yet
- Final-Antenatal Care (Latest) 4Document20 pagesFinal-Antenatal Care (Latest) 4Khibul Lim100% (1)
- Final-Antenatal Care (Latest) 3Document21 pagesFinal-Antenatal Care (Latest) 3Khibul LimNo ratings yet
- NCM 107 Skills Module MCN PDFDocument18 pagesNCM 107 Skills Module MCN PDFmysterioushumane100% (2)
- Conception to Confinement: Facts an Antenatal Mother should KnowFrom EverandConception to Confinement: Facts an Antenatal Mother should KnowNo ratings yet
- Quantum NumbersDocument4 pagesQuantum NumbersAly HannahNo ratings yet
- CardioDocument9 pagesCardioAly HannahNo ratings yet
- Organic Compounds S3Document34 pagesOrganic Compounds S3Aly HannahNo ratings yet
- Urinary SystemDocument10 pagesUrinary SystemAly HannahNo ratings yet
- Magnetic PropertiesDocument3 pagesMagnetic PropertiesAly HannahNo ratings yet
- Quantum Numbers S3Document16 pagesQuantum Numbers S3Aly HannahNo ratings yet
- Mole ConceptDocument5 pagesMole ConceptAly HannahNo ratings yet
- IMF Liquids and SolidsDocument29 pagesIMF Liquids and SolidsAly HannahNo ratings yet
- IsomersDocument15 pagesIsomersAly HannahNo ratings yet
- Combined & Ideal Gas LawDocument12 pagesCombined & Ideal Gas LawAly HannahNo ratings yet
- Dalton Graham Gas LawsDocument16 pagesDalton Graham Gas LawsAly HannahNo ratings yet
- Organization of The Human BodyDocument8 pagesOrganization of The Human BodyAly HannahNo ratings yet
- Chemical BondingDocument17 pagesChemical BondingAly HannahNo ratings yet
- AtomsDocument8 pagesAtomsAly HannahNo ratings yet
- Blood VesselsDocument5 pagesBlood VesselsAly HannahNo ratings yet
- Electron Configuration & Orbital DiagramDocument3 pagesElectron Configuration & Orbital DiagramAly HannahNo ratings yet
- Respiratory SystemDocument13 pagesRespiratory SystemAly HannahNo ratings yet
- Nervous SystemDocument3 pagesNervous SystemAly HannahNo ratings yet
- Lymphatic SystemDocument10 pagesLymphatic SystemAly HannahNo ratings yet
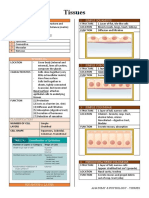
- TissuesDocument4 pagesTissuesAly HannahNo ratings yet
- CSS Airway Management RickyDocument53 pagesCSS Airway Management RickyArtha PutuNo ratings yet
- Re EvaluationDocument4 pagesRe EvaluationchandanaNo ratings yet
- MCN - P2 Post Test (Reviewer)Document3 pagesMCN - P2 Post Test (Reviewer)cianixNo ratings yet
- Hallucinations, Delusions and Paranoia: See The DoctorDocument3 pagesHallucinations, Delusions and Paranoia: See The DoctorNyong FenNo ratings yet
- Dementia - StatPearls - NCBI BookshelfDocument7 pagesDementia - StatPearls - NCBI BookshelfSMA N 1 TOROHNo ratings yet
- HTTPSWWW - whc.SgDocumentsWH Allied20Health and Pharmacy PDFDocument5 pagesHTTPSWWW - whc.SgDocumentsWH Allied20Health and Pharmacy PDFAndrew LimNo ratings yet
- Physiologic Changes in Pregnancy: 1. UterusDocument14 pagesPhysiologic Changes in Pregnancy: 1. UterusNiña Ricci MtflcoNo ratings yet
- TH Participant-Guide WebDocument5 pagesTH Participant-Guide WebYarden ShneyourNo ratings yet
- ACS BookletDocument14 pagesACS Bookletmyat25No ratings yet
- SA Anesthesia Drug Dosages 2022Document3 pagesSA Anesthesia Drug Dosages 2022KRLITHIU Borja100% (1)
- Odontoid FractureDocument40 pagesOdontoid FractureMOHMAMMEDSNo ratings yet
- Dental Health: The ComponentDocument1 pageDental Health: The Componentmaddie g.No ratings yet
- 2009 11 Oral GalvanismDocument2 pages2009 11 Oral GalvanismSppatilNo ratings yet
- Interpretation of Cardiac Enzymes:: Test: SGOTDocument4 pagesInterpretation of Cardiac Enzymes:: Test: SGOTMohammed AbdouNo ratings yet
- Secreciones SubgloticasDocument7 pagesSecreciones SubgloticascamilaNo ratings yet
- The New Yorker - 14 09 2020Document80 pagesThe New Yorker - 14 09 2020Dragoş Şerban PopNo ratings yet
- Statistics On Causes of Death, Malaysia, 2019 PDFDocument7 pagesStatistics On Causes of Death, Malaysia, 2019 PDFsamuelzombieNo ratings yet
- Microbiological Quality of Non-SterileDocument5 pagesMicrobiological Quality of Non-SterilePaula BelloNo ratings yet
- Endocrine of The Pancreas: Eman Alyaseen 20181081Document8 pagesEndocrine of The Pancreas: Eman Alyaseen 20181081ÂmoOł ÀhmdNo ratings yet
- Radiation Toxicity: 31.1 Principles of RadioactivityDocument9 pagesRadiation Toxicity: 31.1 Principles of RadioactivityVarshith GandlaNo ratings yet
- Chemistry 3Document105 pagesChemistry 3patricia pomarNo ratings yet
- Immunization Schedule in India 2017 (Latest !!)Document13 pagesImmunization Schedule in India 2017 (Latest !!)rajNo ratings yet
- Clinical Evaluation Report For Trilogy Evo Ventilator: Prepared For: Respironics, IncDocument79 pagesClinical Evaluation Report For Trilogy Evo Ventilator: Prepared For: Respironics, Incdaphnestc0211No ratings yet
- History of Blood BankingDocument4 pagesHistory of Blood BankingShaira AlcantaraNo ratings yet
- 4 EL Husseinys Essentials of Cardiovascular System @eduwaves360Document236 pages4 EL Husseinys Essentials of Cardiovascular System @eduwaves360ahmed_abu_alrobNo ratings yet
- The Challenge of Kidney Damage During Interventional Cardiology ProceduresDocument6 pagesThe Challenge of Kidney Damage During Interventional Cardiology ProceduresIJAR JOURNALNo ratings yet
- Drug StudyDocument5 pagesDrug Studyanon_168410816No ratings yet
- Use of Chlorhexidine Varnishes in Preventing and Treating Periodontal DiseaseDocument4 pagesUse of Chlorhexidine Varnishes in Preventing and Treating Periodontal Diseasetaher adelNo ratings yet
- Health and Wellness Calendar 2020Document1 pageHealth and Wellness Calendar 2020CHARMAINE ACEVEDONo ratings yet
- Aloe Ferox: A Promising Therapy For Irritable Bowel SyndromeDocument2 pagesAloe Ferox: A Promising Therapy For Irritable Bowel SyndromeYesNo ratings yet