You might also like
- MASD Marina RuranDocument39 pagesMASD Marina RuransaerodinNo ratings yet
- 4.penyembuhan LukaDocument52 pages4.penyembuhan LukaazisaaidrNo ratings yet
- Wounds (Types, Phases of Wound Healing, Complications, Types of Dressings)Document32 pagesWounds (Types, Phases of Wound Healing, Complications, Types of Dressings)Ann Merlin JobinNo ratings yet
- Wound Management GuidelinesDocument12 pagesWound Management GuidelinesFransiscus Braveno RapaNo ratings yet
- 4.penyembuhan LukaDocument52 pages4.penyembuhan LukaFajar Satria Rahmaditya100% (1)
- Skin Integrity:WoundCareDocument7 pagesSkin Integrity:WoundCareBella RomualdoNo ratings yet
- Why Wounds Fail To HealDocument6 pagesWhy Wounds Fail To HealMsPocketbook HoarderNo ratings yet
- Nursing Care For Patient With Wound Nursing Care For Patient With WoundDocument48 pagesNursing Care For Patient With Wound Nursing Care For Patient With Woundayu triaNo ratings yet
- Wound AssessmentDocument64 pagesWound AssessmentKeown MukhtarNo ratings yet
- Nursing Care For Patient With Wound: by PurwaningsihDocument48 pagesNursing Care For Patient With Wound: by Purwaningsihzaenal abidinNo ratings yet
- Bu VonnyDocument41 pagesBu VonnyZola IsmuNo ratings yet
- Basic Principles of Wound MGMT - Poengki DP-ilovepdf-compressedDocument38 pagesBasic Principles of Wound MGMT - Poengki DP-ilovepdf-compressednugrahaNo ratings yet
- Community Nursing Wound Care PresentationDocument56 pagesCommunity Nursing Wound Care PresentationkugernnesNo ratings yet
- Nursing:: CommunityDocument59 pagesNursing:: CommunityIlyes RaniNo ratings yet
- WoundDocument45 pagesWoundHailemariam MebratuNo ratings yet
- Lecture 3Document33 pagesLecture 3Muhammad AhmadNo ratings yet
- Pressure Injury Documentation and Assessment: A Guide To State-Of-The-Art Staging and Recording of PisDocument7 pagesPressure Injury Documentation and Assessment: A Guide To State-Of-The-Art Staging and Recording of PisAlexis TrivinoNo ratings yet
- Chronic Wound Managment HMIDocument37 pagesChronic Wound Managment HMIannisa edwarNo ratings yet
- Wound Care - HandoutDocument8 pagesWound Care - HandoutAryanto HabibieNo ratings yet
- 4.wound Care IDocument46 pages4.wound Care Iamir aizatNo ratings yet
- Webinar Perawatan Luka Dan Tata Laksana Pemeriksaan InfeksiDocument41 pagesWebinar Perawatan Luka Dan Tata Laksana Pemeriksaan Infeksiqoote3No ratings yet
- Pak EdyDocument41 pagesPak EdyZola IsmuNo ratings yet
- Wound HealingDocument36 pagesWound HealingShahenda El-falkyNo ratings yet
- Module 2 Vettech325Document31 pagesModule 2 Vettech325cejproiloNo ratings yet
- Wound-TypesDocument1 pageWound-TypesJamie W.No ratings yet
- Module Five: Wound Care and DressingDocument40 pagesModule Five: Wound Care and DressingZahraJaneANo ratings yet
- Exam 4 Study Guide - Eo JTZDocument16 pagesExam 4 Study Guide - Eo JTZapi-371785797No ratings yet
- Wound Care, Suture Materials & Suturing TechniquesDocument80 pagesWound Care, Suture Materials & Suturing TechniquesAlwin PrasetyaNo ratings yet
- Wounds & Care of Wounds: Lecture DPTDocument52 pagesWounds & Care of Wounds: Lecture DPTSalman KhanNo ratings yet
- Classification and Management of Wound, Principle of Wound Healing, Haemorrhage and Bleeding ControlDocument39 pagesClassification and Management of Wound, Principle of Wound Healing, Haemorrhage and Bleeding ControlrohitNo ratings yet
- Surgery Image BankDocument180 pagesSurgery Image BankRishik RanaNo ratings yet
- Nursing CS Wound-Types 01Document1 pageNursing CS Wound-Types 01Jazzmine GuraNo ratings yet
- A Seb Előadásom HonlapraDocument52 pagesA Seb Előadásom HonlapraAliyah Tofani PawelloiNo ratings yet
- Module 3 HomeworkDocument6 pagesModule 3 HomeworkCj LinceNo ratings yet
- Asuhan Keperawatan Pada Klien Dengan Proses Penyembuhan Luka. Pengkajian Diagnosa Perencanaan Implementasi EvaluasiDocument43 pagesAsuhan Keperawatan Pada Klien Dengan Proses Penyembuhan Luka. Pengkajian Diagnosa Perencanaan Implementasi EvaluasiCak FirmanNo ratings yet
- Classification of WoundsDocument22 pagesClassification of Woundsbuttashly125No ratings yet
- Seminar Bu Vony FixDocument40 pagesSeminar Bu Vony Fixdwi jayantiNo ratings yet
- Types of Wounds & ManagementDocument19 pagesTypes of Wounds & ManagementHina BatoolNo ratings yet
- Surgical WoundDocument40 pagesSurgical WoundAyro Business CenterNo ratings yet
- Cebu Institute of Technology - University College of NursingDocument2 pagesCebu Institute of Technology - University College of NursingSergi Lee OrateNo ratings yet
- Cronic Wound Care PresentDocument30 pagesCronic Wound Care PresentAnonymous pTQIbWT2i9No ratings yet
- Wound ManagementDocument72 pagesWound Managementdrsonuchawla100% (1)
- Diabetic Foot Hajera FinalDocument38 pagesDiabetic Foot Hajera FinalAfifah SelamatNo ratings yet
- Wounds, Tissue Repair and ScarsDocument28 pagesWounds, Tissue Repair and ScarsShahid HameedNo ratings yet
- Maintaining Skin Integrity and Preventing Pressure Ulcers - Information For Nursing Care Homes - January 2018 Final v1.0Document29 pagesMaintaining Skin Integrity and Preventing Pressure Ulcers - Information For Nursing Care Homes - January 2018 Final v1.0JOSHUA DICHOSO100% (1)
- Complex Wounds 2020Document38 pagesComplex Wounds 2020Ài ZìjǐNo ratings yet
- Hips Back Ankles Buttocks HeelsDocument13 pagesHips Back Ankles Buttocks Heelsفرزدق الحسيناويNo ratings yet
- Ho Skin InfectionsDocument10 pagesHo Skin Infectionsnalinigobin22No ratings yet
- A Seb Előadásom HonlapraDocument52 pagesA Seb Előadásom HonlapraChristabella Natalia WijayaNo ratings yet
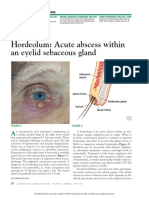
- Hordeolum: Acute Abscess Within An Eyelid Sebaceous Gland: The Clinical PictureDocument3 pagesHordeolum: Acute Abscess Within An Eyelid Sebaceous Gland: The Clinical PictureCamNo ratings yet
- Forensic Project ReportDocument42 pagesForensic Project ReportNIKITANo ratings yet
- WOUNDDocument52 pagesWOUNDIrfan Ritonga100% (6)
- Wound Care 1Document12 pagesWound Care 1Afril CadagNo ratings yet
- WoundDocument22 pagesWoundSandip VaghelaNo ratings yet
- Safari - 26 Mar 2023, 11:28 AMDocument1 pageSafari - 26 Mar 2023, 11:28 AMErza KabashiNo ratings yet
- Integumentary System: Burns and Wounds Clinical Case Study: Degree Burn Depth in Dermal Layers Description ImageDocument6 pagesIntegumentary System: Burns and Wounds Clinical Case Study: Degree Burn Depth in Dermal Layers Description ImageGabrielitoNo ratings yet
- Wound HealingDocument32 pagesWound Healingtepat rshsNo ratings yet
- 2 Wound Care in Patients With Total Bedrest With DecubitusDocument50 pages2 Wound Care in Patients With Total Bedrest With DecubitusGendewa Goa WijayaNo ratings yet
- Pengkajian LukaDocument27 pagesPengkajian LukabayuNo ratings yet
- CRS - Sonia Pradepta - G1a219096 (Wound - Dr. Amran)Document27 pagesCRS - Sonia Pradepta - G1a219096 (Wound - Dr. Amran)heta aprianaNo ratings yet
- Lesson 6 APPLY A DRESSING TO AN OPEN ABDOMINAL WOUNDDocument18 pagesLesson 6 APPLY A DRESSING TO AN OPEN ABDOMINAL WOUNDsrtmedicNo ratings yet
- Forensic Science 2Document20 pagesForensic Science 2Paramjit SinghNo ratings yet
- Show Me How To SurviveDocument19 pagesShow Me How To SurviveWeldon Owen Publishing100% (1)
- Adeshwar Nursing Institute Khamhargaon, Jagdalpur: Community Health Nursing Lesson Plan ON Wound DressingDocument8 pagesAdeshwar Nursing Institute Khamhargaon, Jagdalpur: Community Health Nursing Lesson Plan ON Wound DressingNitesh BhuraNo ratings yet
- How To Assess Surgical Site InfectionDocument4 pagesHow To Assess Surgical Site InfectionswestyNo ratings yet
- 2011 NMC QuestionsDocument8 pages2011 NMC QuestionsKwabena Amankwa100% (2)
- Wound Healing With Vitamin CDocument4 pagesWound Healing With Vitamin CAntonio TovarNo ratings yet
- Teknik AutopsiDocument94 pagesTeknik AutopsiNisa AsikinNo ratings yet
- Homoeopathic Rmedy For ShockDocument2 pagesHomoeopathic Rmedy For ShockSuhas IngaleNo ratings yet
- Child Labor in The PhilippinesDocument7 pagesChild Labor in The PhilippinesMark Gerald Lagamia0% (1)
- Dressing and Bandaging: Book TitleDocument17 pagesDressing and Bandaging: Book TitleJohn TombocNo ratings yet
- Price Per DressingDocument4 pagesPrice Per DressingSmit SanganiNo ratings yet
- أسئلة محلولة خاصة بالسفر البرومترك للمعاهد التمريضDocument25 pagesأسئلة محلولة خاصة بالسفر البرومترك للمعاهد التمريضMohamed MahmoudNo ratings yet
- Fractal Robots Seminar Report PDFDocument24 pagesFractal Robots Seminar Report PDFbiswajitsahoo1111No ratings yet
- Diabetic Foot Ulcers Prevention & ManagementDocument59 pagesDiabetic Foot Ulcers Prevention & Managementcharity kalinowsky100% (2)
- Blackherbals' Product CatalogueDocument73 pagesBlackherbals' Product CatalogueBlackHerbals100% (2)
- LIFE ON THE WESTERN FRONT Aaliya AbdurRahmanDocument5 pagesLIFE ON THE WESTERN FRONT Aaliya AbdurRahmanHeba Fouad100% (1)
- Nursing Care Plan Assessment Nursing Diagnosis Planning Interventions Rationale EvaluationDocument2 pagesNursing Care Plan Assessment Nursing Diagnosis Planning Interventions Rationale EvaluationValerie FischerNo ratings yet
- NCP Stab WoundDocument3 pagesNCP Stab WoundjovedNo ratings yet
- NSTP 2 Midterm ReviewerDocument6 pagesNSTP 2 Midterm ReviewerTrexy NorialNo ratings yet
- Food Laboratory Safety and Sanitation PracticesDocument7 pagesFood Laboratory Safety and Sanitation PracticesCarlson Brian LeeNo ratings yet
- Nail Bed InjuryDocument17 pagesNail Bed InjuryGunjan UpadhyayNo ratings yet
- Jurnal Burst AbdomenDocument7 pagesJurnal Burst AbdomenDeana Annisa AzizNo ratings yet
- Impaired Skin DMDocument3 pagesImpaired Skin DMimnotdatsunny100% (1)
- A Sistematic Review of Clinical Effectiveness of Wound Edge Protector Device in Abdominal Surgery Sajid2017Document8 pagesA Sistematic Review of Clinical Effectiveness of Wound Edge Protector Device in Abdominal Surgery Sajid2017andreigustvNo ratings yet
- Untitled PresentationDocument228 pagesUntitled PresentationSafira WasimNo ratings yet
- Fitness Choices and First Aid Study NotesDocument11 pagesFitness Choices and First Aid Study NotesAlan VanNo ratings yet
- SUTURESDocument33 pagesSUTURESChin Chan100% (4)
- Wound Management of Venous Leg Ulcer, Hartmann, 2006Document47 pagesWound Management of Venous Leg Ulcer, Hartmann, 2006Karen PinemNo ratings yet