You might also like
- Genetic Testing Guide: Types, Purpose, TechniquesDocument50 pagesGenetic Testing Guide: Types, Purpose, TechniquesLokeshwari KatreNo ratings yet
- Triple Test InvestigationDocument5 pagesTriple Test InvestigationJyothi Singh SuryavanshiNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 9: GynecologyFrom EverandComplementary and Alternative Medical Lab Testing Part 9: GynecologyNo ratings yet
- Prenatal Diagnosis and ScreeningDocument55 pagesPrenatal Diagnosis and ScreeningRania ZahoNo ratings yet
- tmp647F TMPDocument13 pagestmp647F TMPFrontiersNo ratings yet
- Prenatal DiagnosisDocument42 pagesPrenatal DiagnosisarunjyothishNo ratings yet
- Procreative Health Is The Moral Obligation of Parents To Have The Healthiest Children Through All Natural and Artificial Means AvailableDocument9 pagesProcreative Health Is The Moral Obligation of Parents To Have The Healthiest Children Through All Natural and Artificial Means AvailableShiela Mae GalisaNo ratings yet
- Prenatal Diagnosis Techniques GuideDocument33 pagesPrenatal Diagnosis Techniques Guidejien_yeenNo ratings yet
- Prenatal Diagnosis Methods and GoalsDocument22 pagesPrenatal Diagnosis Methods and GoalshusshamNo ratings yet
- DEVPSYPRENATALDocument24 pagesDEVPSYPRENATALguidancephiltechstarosa16No ratings yet
- CH 10 - Antepartum Fetal AssessmentDocument8 pagesCH 10 - Antepartum Fetal Assessmentnat0118100% (1)
- Antenatal Assessment of Fetal Well Being: DR - Abdulkarim Ahmed MohamudDocument46 pagesAntenatal Assessment of Fetal Well Being: DR - Abdulkarim Ahmed MohamudPeterNo ratings yet
- Adolescent Gynecologic Care QUESTIONS 1, 2, 3Document7 pagesAdolescent Gynecologic Care QUESTIONS 1, 2, 3patelkn_2005No ratings yet
- Undescended Testes (CryptorchidismDocument6 pagesUndescended Testes (CryptorchidismJayson Almario AranasNo ratings yet
- Assessment of Fetal Well BeingDocument29 pagesAssessment of Fetal Well Beingmalaika khanNo ratings yet
- DR Ogunwale A.N Ufm UnitDocument37 pagesDR Ogunwale A.N Ufm UnitzumarockNo ratings yet
- 1060 High Risk PregnancyDocument79 pages1060 High Risk PregnancyGOPIKA C KNo ratings yet
- Electronic Fetal Monitoring: Premature LaborDocument5 pagesElectronic Fetal Monitoring: Premature LaborEzraManzanoNo ratings yet
- Test During Anc (Antenatal Care) : Presented By-Veena Krishnamurthy Padakanti Roll No: - 17Document16 pagesTest During Anc (Antenatal Care) : Presented By-Veena Krishnamurthy Padakanti Roll No: - 17Anurag SuryawanshiNo ratings yet
- Prenatal Diagnosis Estimation of Foetal Age 1Document33 pagesPrenatal Diagnosis Estimation of Foetal Age 1Riya SinghNo ratings yet
- Cell Carcinoma, But Also To Other Cancers As Well (E.g., Thyroid Carcinoma, Melanoma)Document4 pagesCell Carcinoma, But Also To Other Cancers As Well (E.g., Thyroid Carcinoma, Melanoma)Erick EchualNo ratings yet
- Initial Visit4Document8 pagesInitial Visit4elgitharahayu67No ratings yet
- Risk Factors for High-Risk PregnanciesDocument8 pagesRisk Factors for High-Risk PregnanciesLRDR UCMEDNo ratings yet
- Prenatal diagnosis of genetic diseasesDocument11 pagesPrenatal diagnosis of genetic diseasesMini PGNo ratings yet
- Screening and Diagnostic Test For Chromosomal DisordersDocument21 pagesScreening and Diagnostic Test For Chromosomal DisordersJohn Van Dave TaturoNo ratings yet
- Antenatal Assessment of Foetal Wellbeing.Document30 pagesAntenatal Assessment of Foetal Wellbeing.Kavya S MohanNo ratings yet
- What Type of Prenatal Screening Is Available For Down SyndromeDocument2 pagesWhat Type of Prenatal Screening Is Available For Down SyndromeMichael MikuruNo ratings yet
- 1Document4 pages1James Victor Villanueva100% (2)
- Dev PsychDocument2 pagesDev PsychKharrel YballeNo ratings yet
- (L13) - Human Reproduction - Aug 4, 2019 - SundayDocument32 pages(L13) - Human Reproduction - Aug 4, 2019 - Sundayصوفي اشوڪ ڪمارNo ratings yet
- Screening Tests: Prenatal Diagnosis of Fetal DiseaseDocument6 pagesScreening Tests: Prenatal Diagnosis of Fetal DiseaseMischief ManagerNo ratings yet
- Diagnostic Procedures of PregnancyDocument7 pagesDiagnostic Procedures of PregnancyRuth Anne Zonio DamasoNo ratings yet
- O@g Maternal and Fetal Mesures ContentDocument22 pagesO@g Maternal and Fetal Mesures Contentjeya maniNo ratings yet
- Ultrasound Scanning of Fetal AnomalyDocument19 pagesUltrasound Scanning of Fetal AnomalyFA Khan0% (1)
- Ante PartumDocument49 pagesAnte PartumNikhil TyagiNo ratings yet
- Maternal Serum Alpha-Fetoprotein (MSAFP)Document2 pagesMaternal Serum Alpha-Fetoprotein (MSAFP)Shaells JoshiNo ratings yet
- Genetic Counselling and Prenatal ScreeningDocument8 pagesGenetic Counselling and Prenatal ScreeningFarheen khanNo ratings yet
- Prenatal Genetic Screening DBiagnosis Hamamy 2010Document27 pagesPrenatal Genetic Screening DBiagnosis Hamamy 2010Georgie StephenNo ratings yet
- Biochemical Methods ObgDocument25 pagesBiochemical Methods ObgRupali AroraNo ratings yet
- What Is Noninvasive Prenatal Screening (NIPS) ?Document5 pagesWhat Is Noninvasive Prenatal Screening (NIPS) ?Le Phuong LyNo ratings yet
- Discover Genetic Problems with Amniocentesis TestDocument5 pagesDiscover Genetic Problems with Amniocentesis TestMichael MikuruNo ratings yet
- Ultra Sound in PregnancyDocument77 pagesUltra Sound in Pregnancyhussain AltaherNo ratings yet
- Prenatal Screening and Diagnosis of SyndromesDocument49 pagesPrenatal Screening and Diagnosis of SyndromesSamuel WilliamsNo ratings yet
- En 22Document6 pagesEn 22Saulo AlmeidaNo ratings yet
- Genetic Testing of A FetusDocument2 pagesGenetic Testing of A Fetusapi-353526506No ratings yet
- EP C2 by EliDocument40 pagesEP C2 by EliElsai EsbNo ratings yet
- Essential Pregnancy Lab TestsDocument10 pagesEssential Pregnancy Lab TestsJoan Venida100% (1)
- Group A PDFDocument34 pagesGroup A PDFAnsa WaqarNo ratings yet
- The Objective of Prenatal Diagnosis Is To Determine Whether A Fetus Believed To Be at Risk For Some Genetic Disease Is or Is Not Actually AffectedDocument14 pagesThe Objective of Prenatal Diagnosis Is To Determine Whether A Fetus Believed To Be at Risk For Some Genetic Disease Is or Is Not Actually AffectednkivcNo ratings yet
- High Risk PregnancyDocument46 pagesHigh Risk PregnancySonali SoumyashreeNo ratings yet
- Government College of Nursing Jodhpur (Raj.) : Procedure On-Amniocentesis Subject-Obstetrics & Gynaecology Specialty-IDocument7 pagesGovernment College of Nursing Jodhpur (Raj.) : Procedure On-Amniocentesis Subject-Obstetrics & Gynaecology Specialty-Ipriyanka100% (1)
- Prenatal DiagnosisDocument26 pagesPrenatal DiagnosisShandy Suwanto PutraNo ratings yet
- Intra Uterine Growth RetardationDocument46 pagesIntra Uterine Growth RetardationIba Ghannam100% (1)
- Reviewed - IJANS-Recent Antenatal Investigations For Better Pregnancy OutcomesDocument4 pagesReviewed - IJANS-Recent Antenatal Investigations For Better Pregnancy Outcomesiaset123No ratings yet
- MATERNAL SERUM ALFA FETO PROTEIN (Jyoti Singh)Document11 pagesMATERNAL SERUM ALFA FETO PROTEIN (Jyoti Singh)Jyothi Singh SuryavanshiNo ratings yet
- Down syndrome screening resultsDocument11 pagesDown syndrome screening resultslightning proNo ratings yet
- Embarazo EctopicoDocument10 pagesEmbarazo EctopicocfsaludNo ratings yet
- Antepartum Diagnostic TestingDocument2 pagesAntepartum Diagnostic TestingRussel Kate SulangNo ratings yet
- Conners Scale For AdhdDocument3 pagesConners Scale For Adhdshreya sharmaNo ratings yet
- Literature Survey For Lung Cancer Analysis and PredictionDocument6 pagesLiterature Survey For Lung Cancer Analysis and PredictionIJRASETPublicationsNo ratings yet
- Hyperprolinemia as a clue in psychiatric diagnosisDocument3 pagesHyperprolinemia as a clue in psychiatric diagnosisAli Emre KöseNo ratings yet
- Clinical Predictors of Shoulders Tendon Pathology in Patients With Early Parkinson S Disease Sonographic and Clinical AssociationsDocument10 pagesClinical Predictors of Shoulders Tendon Pathology in Patients With Early Parkinson S Disease Sonographic and Clinical AssociationsHerald Scholarly Open AccessNo ratings yet
- EncephalitisDocument6 pagesEncephalitis4pm6gjq78cNo ratings yet
- Dementia - Symptoms, Diagnosis, Causes, TreatmentsDocument6 pagesDementia - Symptoms, Diagnosis, Causes, TreatmentsRatnaPrasadNalamNo ratings yet
- Child Symptom Inventory-4 (CSI-4)Document2 pagesChild Symptom Inventory-4 (CSI-4)Trisha Yap100% (1)
- Case Presentation DengueDocument3 pagesCase Presentation DengueEver Seneca EscaLeraNo ratings yet
- PrednisoloneDocument8 pagesPrednisoloneAjaybpaNo ratings yet
- ICMR Specimen Referral Form for COVID-19 testingDocument2 pagesICMR Specimen Referral Form for COVID-19 testingSufyan UmarNo ratings yet
- Parasite Worms in Intestine SymptomsDocument3 pagesParasite Worms in Intestine SymptomsMichael AngNo ratings yet
- Long Covid An Update Full Presentation Final VersionDocument99 pagesLong Covid An Update Full Presentation Final VersionyudistiraanwarNo ratings yet
- Evolve Resources For Goulds Pathophysiology For The Health Professions 6th Edition Hubert Test BankDocument8 pagesEvolve Resources For Goulds Pathophysiology For The Health Professions 6th Edition Hubert Test Bankjosephgillmtjirpxngk100% (15)
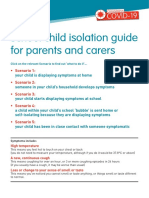
- Coronavirus school isolation guide for parentsDocument6 pagesCoronavirus school isolation guide for parentsMohammad TaNo ratings yet
- Medical Decision Making NEWDocument10 pagesMedical Decision Making NEWKrishna KamuniNo ratings yet
- Pediatric ClerkshipDocument56 pagesPediatric ClerkshipSyukriNo ratings yet
- Social Science & MedicineDocument9 pagesSocial Science & MedicineTriana virgaNo ratings yet
- Designing Inclusion and Exclusion CriteriaDocument13 pagesDesigning Inclusion and Exclusion CriteriaSamuel GarciaNo ratings yet
- Long COVIDDocument8 pagesLong COVIDSMIBA MedicinaNo ratings yet
- BHERT OrientationDocument16 pagesBHERT Orientationsheila gugudanNo ratings yet
- Headache Oet ReadingDocument22 pagesHeadache Oet ReadinglianausinNo ratings yet
- Schizophrenia Patient GuideDocument14 pagesSchizophrenia Patient GuideDragutin PetrićNo ratings yet
- Schizophrenia: Schizophrenia Is A Mental DisorderDocument54 pagesSchizophrenia: Schizophrenia Is A Mental Disorderhasan jamiNo ratings yet
- Q3 Health 8 Module 3 PDFDocument13 pagesQ3 Health 8 Module 3 PDFkateNo ratings yet
- Cervical Assessment Form FILLABLE Jun 2020 PDFDocument2 pagesCervical Assessment Form FILLABLE Jun 2020 PDFsanavoraNo ratings yet
- Adjunctive Deep Touch Pressure For Comorbid Anxiety in Bipolar Disorder Mediated by Control of Sensory InputDocument7 pagesAdjunctive Deep Touch Pressure For Comorbid Anxiety in Bipolar Disorder Mediated by Control of Sensory Inputariq imamNo ratings yet
- Government Service Insurance System, Petitioner, vs. ASTRID V. CORRALES, RespondentDocument20 pagesGovernment Service Insurance System, Petitioner, vs. ASTRID V. CORRALES, RespondentMaryland AlajasNo ratings yet
- Email Consultation Form GuideDocument21 pagesEmail Consultation Form GuideJoshua Diaz FloroNo ratings yet
- Ettinger 2005Document7 pagesEttinger 2005Santy P Vásconez CalderónNo ratings yet
- ANNEX E CONSENT FORM Edited 082922Document2 pagesANNEX E CONSENT FORM Edited 082922leslie buenNo ratings yet