You might also like
- Operating RoomDocument17 pagesOperating RoomNoor GraphicsNo ratings yet
- Hospital Planning - Non - Clinical DepartmentDocument32 pagesHospital Planning - Non - Clinical DepartmentNidhi KhareNo ratings yet
- Architecture of Hospital DesignDocument38 pagesArchitecture of Hospital DesignPriyanka_Kh_3016No ratings yet
- Planning and Designing of OTDocument42 pagesPlanning and Designing of OTPaul Priyaraj100% (3)
- Chapter 3 - Operating Theater DesignDocument69 pagesChapter 3 - Operating Theater Designmarye agegnNo ratings yet
- Faculty of Nursing & Health Science Advance Nursing Nurse 337Document18 pagesFaculty of Nursing & Health Science Advance Nursing Nurse 337Yousef JafarNo ratings yet
- Guideline For Ideal OT LayoutDocument36 pagesGuideline For Ideal OT Layoutjake369100% (2)
- Architectural Design VI Daignostics: Group Members-Anubhav Gupta Pranav Sharma Saalim Jia BhattDocument33 pagesArchitectural Design VI Daignostics: Group Members-Anubhav Gupta Pranav Sharma Saalim Jia BhattAnubhav GuptaNo ratings yet
- Hospital Planning - Operating RoomDocument51 pagesHospital Planning - Operating RoomNidhi KhareNo ratings yet
- Theatre and CSSD Issues in Infection Control FINAL DOCUMENTDocument57 pagesTheatre and CSSD Issues in Infection Control FINAL DOCUMENTRanganathan IyerNo ratings yet
- Peri-Operative Care (Theatre Nursing) : Learning ObjectivesDocument21 pagesPeri-Operative Care (Theatre Nursing) : Learning ObjectivesGabriel GagaNo ratings yet
- ADW Presentasi Desain Ruangan RS Perdalin 2021Document50 pagesADW Presentasi Desain Ruangan RS Perdalin 2021Fergy puspitaNo ratings yet
- Designing Hospital For Better Infection ControlDocument13 pagesDesigning Hospital For Better Infection ControlMohd SalahuddinNo ratings yet
- Operation Theater 1Document24 pagesOperation Theater 1Susmita BeheraNo ratings yet
- Organization of Intensive Care UnitDocument39 pagesOrganization of Intensive Care UnitHarshil Dave100% (2)
- Chapter 1Document67 pagesChapter 1Abel AbebeNo ratings yet
- Ancillary ServicesDocument88 pagesAncillary ServicesSangeeta BSR0% (1)
- Hospital Design: Operation Theatre ComplexDocument21 pagesHospital Design: Operation Theatre ComplexNaitik JaiswalNo ratings yet
- Guidelines For Design of Operating Theaters 2007: State of Kuwait Ministry of Health Infection Control DirectorateDocument23 pagesGuidelines For Design of Operating Theaters 2007: State of Kuwait Ministry of Health Infection Control DirectorateSameera ShamanNo ratings yet
- Hvac MergedDocument64 pagesHvac MergedAbhishek RajputNo ratings yet
- Theatre Nursing: By: Gachuhi WangariDocument130 pagesTheatre Nursing: By: Gachuhi WangariJonah nyachae100% (1)
- Docs 15Document11 pagesDocs 15Lokesh KandyNo ratings yet
- Operation Theatre ComplexDocument26 pagesOperation Theatre ComplexS AkashNo ratings yet
- International Case StudyDocument36 pagesInternational Case Studymamona zaheerNo ratings yet
- PSSRDocument31 pagesPSSRAsadullah MeharNo ratings yet
- Group-6 Hospital ServicesDocument76 pagesGroup-6 Hospital ServicesParth AgarwalNo ratings yet
- Hospital and Health Care FacilitiesDocument7 pagesHospital and Health Care FacilitiesToteng TanglaoNo ratings yet
- Operating Room 2Document66 pagesOperating Room 2Ogy Ayop Mummy UddinNo ratings yet
- Report Presentation ON Central Sterile Supply Department (CSSD) CRH, 5Th Mile TadongDocument35 pagesReport Presentation ON Central Sterile Supply Department (CSSD) CRH, 5Th Mile TadongPraty Sawaden100% (1)
- Environmental Cleaning Presentation 3 OR and Procedure RoomsDocument77 pagesEnvironmental Cleaning Presentation 3 OR and Procedure RoomsYahia HassaanNo ratings yet
- A&E ServicesDocument38 pagesA&E ServiceskanikaNo ratings yet
- GENERAL HOSPITAL DESIGN SSTDocument19 pagesGENERAL HOSPITAL DESIGN SSTmamona zaheerNo ratings yet
- Module 3 Cleaning The or and Procedure RoomsDocument79 pagesModule 3 Cleaning The or and Procedure RoomsNurul Uswatin100% (1)
- Planning an Operation Theatre ComplexDocument47 pagesPlanning an Operation Theatre Complexamol_taam100% (11)
- Organization of Intensive Care Unit: Department of Anesthesiology M.L.B. Medical College, JhansiDocument40 pagesOrganization of Intensive Care Unit: Department of Anesthesiology M.L.B. Medical College, JhansiFalguni PaulNo ratings yet
- Cleaning The or and Procedure RoomsDocument79 pagesCleaning The or and Procedure RoomsDaole Van100% (2)
- Operating RoomDocument23 pagesOperating RoomTheresa Bread83% (6)
- Laundry Design in Hospital Literature Study - RMDocument26 pagesLaundry Design in Hospital Literature Study - RMrishad mufas100% (1)
- Lecture 19-Selection, Installation & CommissioningDocument29 pagesLecture 19-Selection, Installation & CommissioningAbdul RehmanNo ratings yet
- Central Sterile Supply DepartmentDocument43 pagesCentral Sterile Supply DepartmentMohd SalahuddinNo ratings yet
- Instrument Washer DisinfectorDocument12 pagesInstrument Washer DisinfectorsamiNo ratings yet
- EMERGENCY DEPARTMENT OVERVIEWDocument48 pagesEMERGENCY DEPARTMENT OVERVIEWRachana VishwajeetNo ratings yet
- HOSPITAL LITERATURE STUDY: KEY AREAS AND DESIGN CONSIDERATIONSDocument32 pagesHOSPITAL LITERATURE STUDY: KEY AREAS AND DESIGN CONSIDERATIONSShivanand Pegu100% (1)
- Designing Ideal Operating Room ComplexDocument7 pagesDesigning Ideal Operating Room ComplexAliyya RifkiNo ratings yet
- GrossingDocument38 pagesGrossingNatalia Haikali100% (1)
- CSSD PresentationDocument23 pagesCSSD PresentationNirali Sheth91% (22)
- Central Sterile ServiceDocument75 pagesCentral Sterile ServiceSUBHENDU SIKDAR100% (1)
- 1-Planning and Design Guidelines For Dialysis ClinicsDocument25 pages1-Planning and Design Guidelines For Dialysis ClinicsMichael Marc Andico DeleonNo ratings yet
- Central Sterile Supply DepartmentDocument25 pagesCentral Sterile Supply DepartmentRevati shindeNo ratings yet
- Planning Accident and Emergency FacilitiesDocument29 pagesPlanning Accident and Emergency FacilitiesJaina JoseNo ratings yet
- Planning An Operation Theatre ComplexDocument65 pagesPlanning An Operation Theatre Complexpdamodar200794% (66)
- Chapter 2 Tissue CultureDocument134 pagesChapter 2 Tissue CultureTesfamichaelLibenNo ratings yet
- Design of Isolation RoomDocument3 pagesDesign of Isolation Room791221No ratings yet
- Planin N Org of Hosp Unit and Ancillary ServicesDocument61 pagesPlanin N Org of Hosp Unit and Ancillary ServicesCynthia Thomas69% (13)
- Kebijakan Pelayanan Sterilisasi Sentral (CSSD) : Ali SyamlanDocument37 pagesKebijakan Pelayanan Sterilisasi Sentral (CSSD) : Ali SyamlanMorion ReskiNo ratings yet
- Handbook To Build An Hospital CRF PDFDocument25 pagesHandbook To Build An Hospital CRF PDFFernanda Ramírez100% (1)
- Definition of CSSD - Central Sterile Supply DepartmentDocument3 pagesDefinition of CSSD - Central Sterile Supply DepartmentRevati shindeNo ratings yet
- CHEMO&LAB DesignDocument38 pagesCHEMO&LAB DesignDanish RaisNo ratings yet
- Inside the Pill Bottle: A Comprehensive Guide to the Pharmaceutical IndustryFrom EverandInside the Pill Bottle: A Comprehensive Guide to the Pharmaceutical IndustryNo ratings yet
- 16th Edition IEE Wiring Regulations: Design and Verification of Electrical InstallationsFrom Everand16th Edition IEE Wiring Regulations: Design and Verification of Electrical InstallationsRating: 4 out of 5 stars4/5 (1)
- Accessibility of Healthcare Among Poor Women in Coastal CommunitiesDocument30 pagesAccessibility of Healthcare Among Poor Women in Coastal Communitiesajdgafjsdga100% (1)
- Hospital Department & Giving DirectionDocument3 pagesHospital Department & Giving Directionaida khairunnisaNo ratings yet
- Surgical Technology For The Surgical Technologist A Positive Care Approach 5th Edition Association of Surgical Technologists Test BankDocument36 pagesSurgical Technology For The Surgical Technologist A Positive Care Approach 5th Edition Association of Surgical Technologists Test Bankandrefloresxudd100% (28)
- Effectiveness of Myofunctional Therapy in Ankyloglossia: A Systematic ReviewDocument18 pagesEffectiveness of Myofunctional Therapy in Ankyloglossia: A Systematic Reviewmistic0No ratings yet
- List of Doctors and Schedule (Cebu Province)Document16 pagesList of Doctors and Schedule (Cebu Province)Airwind Villarin100% (3)
- Euroanaesthesia 2015 Abstract BookDocument481 pagesEuroanaesthesia 2015 Abstract BookTrình BiomedicNo ratings yet
- AP Animal Husbandry Assistant Syllabus 2023Document4 pagesAP Animal Husbandry Assistant Syllabus 2023Shaik WazeedNo ratings yet
- Federal Law No. 16 of 2007 EngDocument26 pagesFederal Law No. 16 of 2007 EngZaki AziziNo ratings yet
- Steam SterilizationDocument2 pagesSteam SterilizationHeru Prabowo HadiNo ratings yet
- The Dog Boy of WestminsterDocument12 pagesThe Dog Boy of WestminsterKurt GarwoodNo ratings yet
- Skims Syllabus Staff NurseDocument9 pagesSkims Syllabus Staff NurseWani Zahoor50% (2)
- Conscious Sedation Policy: Levels of Consciousness 84Document12 pagesConscious Sedation Policy: Levels of Consciousness 84rajtherisingstarNo ratings yet
- Health InsuranceDocument21 pagesHealth Insuranceadhitya0% (1)
- Henry Lindlahr-Nature CureDocument275 pagesHenry Lindlahr-Nature Curegem68meg100% (3)
- Midas Rex Legend: Pneumatic High-Speed SystemDocument48 pagesMidas Rex Legend: Pneumatic High-Speed SystemSveto SlNo ratings yet
- 2009-SUPPORT Tools For Evidence-Informed Policymaking in Health 18-Planning Monitoring and Evaluation of PoliciesDocument8 pages2009-SUPPORT Tools For Evidence-Informed Policymaking in Health 18-Planning Monitoring and Evaluation of PoliciesJULIO CESAR MATEUS SOLARTENo ratings yet
- Practices and Beliefs Regarding Throat Pack: A Reviewon UsageDocument4 pagesPractices and Beliefs Regarding Throat Pack: A Reviewon UsageIJAR JOURNALNo ratings yet
- How To Plan Treatment Costing With CancerDocument2 pagesHow To Plan Treatment Costing With CancerShraddhanvita TiwariNo ratings yet
- Physio After SurgeryDocument2 pagesPhysio After SurgeryGursangeet KaurNo ratings yet
- QRS For BDS 4th Year Oral and Maxillofacial SurgeryDocument299 pagesQRS For BDS 4th Year Oral and Maxillofacial SurgeryHumna Khan100% (1)
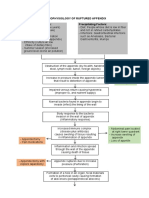
- Pathophysiology of Ruptured AppendixDocument2 pagesPathophysiology of Ruptured AppendixAya PaquitNo ratings yet
- Perforated Peptic Ulcer DictationDocument4 pagesPerforated Peptic Ulcer DictationHassanNo ratings yet
- Removal of SutureDocument52 pagesRemoval of SutureChris_Bentres_3615No ratings yet
- Healthcare 10 00760Document17 pagesHealthcare 10 00760Wanda HafidzahNo ratings yet
- Trinidad, Mikhaela Gayle A. BSN-3C: 1) Suction Poole Drain-UDocument13 pagesTrinidad, Mikhaela Gayle A. BSN-3C: 1) Suction Poole Drain-UJewenson SalvadorNo ratings yet
- ZZZZZDocument2 pagesZZZZZleandro__scribdNo ratings yet
- What To Expect After GallbladderDocument2 pagesWhat To Expect After GallbladderJennifer PorlaresNo ratings yet
- Preparing Room For Major Surgery Updated 2020Document6 pagesPreparing Room For Major Surgery Updated 2020Riza Angela BarazanNo ratings yet
- Hospital Pekan PresentationDocument25 pagesHospital Pekan PresentationImtiazNo ratings yet
- FK Conox Product Brochure 4ppa4 v6Document4 pagesFK Conox Product Brochure 4ppa4 v6Lucas ShotsNo ratings yet