You might also like
- Liver RebeDocument81 pagesLiver RebeOded YanaNo ratings yet
- Varicose Vein - Management, DVT: BY Anandhu Lal Anjali P K AnjusjDocument108 pagesVaricose Vein - Management, DVT: BY Anandhu Lal Anjali P K AnjusjAsif AbbasNo ratings yet
- 2 POCUS in Emergency FAST IVC LUNGresidents December 2022Document92 pages2 POCUS in Emergency FAST IVC LUNGresidents December 2022dr mohd abdul basithNo ratings yet
- Jeac 239Document4 pagesJeac 239Spam MailerNo ratings yet
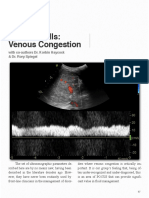
- Venous Congestion ChapterDocument8 pagesVenous Congestion ChapterpcarrascoeNo ratings yet
- SSS, BCS, Avf, MalDocument42 pagesSSS, BCS, Avf, MalchintamaniNo ratings yet
- US Liver Doppler OnlyDocument8 pagesUS Liver Doppler OnlymicropocketfilmsNo ratings yet
- Doppler of Varicose VeinsDocument85 pagesDoppler of Varicose VeinsDiaa Eldeeb100% (2)
- Cyanotic Heart DiseaseDocument66 pagesCyanotic Heart DiseasePrasanth SankarNo ratings yet
- Hemodialysis Access: Ultrasound Evaluation Before & After CreationDocument40 pagesHemodialysis Access: Ultrasound Evaluation Before & After CreationobdeeNo ratings yet
- Natalya Master CardioDocument71 pagesNatalya Master CardioTaman Hoang100% (1)
- Abdominal AortaDocument41 pagesAbdominal AortaMichael IdowuNo ratings yet
- Right Superior Vena Cava Draining To Left AtriumDocument42 pagesRight Superior Vena Cava Draining To Left AtriumKunwar Sidharth SaurabhNo ratings yet
- Aortic Stenosis:: Updates in Diagnosis & ManagementDocument48 pagesAortic Stenosis:: Updates in Diagnosis & ManagementCuca PcelaNo ratings yet
- Emergency UltrasoundDocument32 pagesEmergency UltrasoundChoga ArlandoNo ratings yet
- Jo Boy With SOB 04202016Document25 pagesJo Boy With SOB 04202016sirrfsNo ratings yet
- Fontan Operation: DR Hussain BuxDocument62 pagesFontan Operation: DR Hussain BuxMujeeb Ur RehmanNo ratings yet
- CCPACatheter Basics 07 MedicineDocument44 pagesCCPACatheter Basics 07 MedicinerinbijoyNo ratings yet
- CC, CVP MonitoringDocument5 pagesCC, CVP MonitoringM7md Al-HuwaitiNo ratings yet
- Take5 Hemodynamic1Document2 pagesTake5 Hemodynamic1est03No ratings yet
- HydrocephalusDocument39 pagesHydrocephalusAjeng Aristiany Rahawarin100% (1)
- HydrocephalusDocument39 pagesHydrocephalusspiritNo ratings yet
- Echo PresentationDocument36 pagesEcho PresentationSalman MajidNo ratings yet
- Congenital Heart Disease: Kriti Puri, MD Hugh D. Allen, MD Athar M. Qureshi, MDDocument30 pagesCongenital Heart Disease: Kriti Puri, MD Hugh D. Allen, MD Athar M. Qureshi, MDhari ilman toniNo ratings yet
- LiverultrasoundDocument62 pagesLiverultrasoundiuliia94No ratings yet
- Monitoring Hemodynamic Utk MahasiswaDocument49 pagesMonitoring Hemodynamic Utk MahasiswaPratami Rieuwpassa IINo ratings yet
- Haemodynamicmonitoring 180208210620Document30 pagesHaemodynamicmonitoring 180208210620Morad KananNo ratings yet
- Physiomonitoring TransDocument4 pagesPhysiomonitoring TransAimie DagaleaNo ratings yet
- Portal Hypertension SurgeryDocument6 pagesPortal Hypertension SurgeryjackSNMMCNo ratings yet
- Ecr2017 C-2166Document33 pagesEcr2017 C-2166jbmbritoNo ratings yet
- Imaging in Abdominal Trauma: S ThiyagarajanDocument133 pagesImaging in Abdominal Trauma: S ThiyagarajanEdward Arthur IskandarNo ratings yet
- Central Lines AND Arterial LinesDocument30 pagesCentral Lines AND Arterial LinesamiraattyaNo ratings yet
- Foetalcirculationpphn 151109152112 Lva1 App6891Document45 pagesFoetalcirculationpphn 151109152112 Lva1 App6891shravaniNo ratings yet
- Clinical Portal Hyoer TensionDocument8 pagesClinical Portal Hyoer TensionAhmed ImranNo ratings yet
- Portal HypertensionDocument22 pagesPortal Hypertensionsara.sherif099No ratings yet
- Non-Invasive Monitoring EquipmentDocument6 pagesNon-Invasive Monitoring EquipmentSuhana PathanNo ratings yet
- PCV VetlearnDocument1 pagePCV VetlearnJorge Pablo VillaseñorNo ratings yet
- (FEU) Central Venous Pressure Notes PDFDocument25 pages(FEU) Central Venous Pressure Notes PDFBryJos tiongsonNo ratings yet
- Haemodynamic MonitoringDocument30 pagesHaemodynamic MonitoringMaiiaNo ratings yet
- Hemodaynamic Monitoring KHDocument91 pagesHemodaynamic Monitoring KHomar kmr97No ratings yet
- Extended Focused Assessment With Sonography in Trauma (eFAST)Document45 pagesExtended Focused Assessment With Sonography in Trauma (eFAST)vimal rajNo ratings yet
- Baltarowich ABD pt1 Hepatobiliary US PDFDocument22 pagesBaltarowich ABD pt1 Hepatobiliary US PDFEka KusumaningatiNo ratings yet
- Hydrocephalus Teori FinalDocument19 pagesHydrocephalus Teori Finalaurelia_rlNo ratings yet
- Trauma Ultrasound and The FAST ExamDocument7 pagesTrauma Ultrasound and The FAST ExamhaldiszopianNo ratings yet
- Central Venous PressureDocument22 pagesCentral Venous Pressurejhong100% (1)
- Cirrhosis and Its ComplicationsDocument3 pagesCirrhosis and Its ComplicationsMahaNo ratings yet
- Hemodynamic MonitoringDocument39 pagesHemodynamic MonitoringNor Jeannah PolaoNo ratings yet
- Physiologic Monitoring of A Surgical PatientDocument41 pagesPhysiologic Monitoring of A Surgical PatientAlna Shelah IbañezNo ratings yet
- Partially Reversed Intrasplenic Venous Blood Flow Detected by Color Doppler SonographyDocument4 pagesPartially Reversed Intrasplenic Venous Blood Flow Detected by Color Doppler SonographydenisegmeloNo ratings yet
- Venous and Lymphatic DiseaseDocument46 pagesVenous and Lymphatic DiseaseHendra AjahNo ratings yet
- Congenital Heart Surgery: The Appropriate Diagnosis Is Achieved byDocument9 pagesCongenital Heart Surgery: The Appropriate Diagnosis Is Achieved byprofarmahNo ratings yet
- CVPDocument13 pagesCVPmeisin kuraesinNo ratings yet
- RadiologyDocument46 pagesRadiologyitho23100% (1)
- UW Notes - 7 - Cardiology ArrangedDocument84 pagesUW Notes - 7 - Cardiology ArrangedAaquib AmirNo ratings yet
- CVP LineDocument26 pagesCVP LineÂbdàlláh Âl Ñàjjár0% (1)
- Anesthetic Aspects of The Fontan PatientDocument69 pagesAnesthetic Aspects of The Fontan PatientdavidmontoyaNo ratings yet
- Cardio AssessmentDocument104 pagesCardio Assessmentlowell.cerezo.ihsNo ratings yet
- Aplio Platinum Series Innovation 2016Document4 pagesAplio Platinum Series Innovation 2016SikliNo ratings yet
- QuestionsDocument21 pagesQuestionsashaaman0325No ratings yet
- International Journal of Veterinary Science and MedicineDocument6 pagesInternational Journal of Veterinary Science and MedicineXinevlin XinevlinNo ratings yet
- Ocular UltrasoundDocument184 pagesOcular UltrasoundAlinaBrinzaNo ratings yet
- 34implementation of Zoom FFT in Ultrasonic Blood Flow ADocument15 pages34implementation of Zoom FFT in Ultrasonic Blood Flow ARamanjaneyulu Chandana100% (2)
- Gynaecological Ultrasound in Clinical PracticeDocument247 pagesGynaecological Ultrasound in Clinical Practiceyulb_1100% (5)
- Precision Spec H E V14-01Document23 pagesPrecision Spec H E V14-01Rama Tenis CopecNo ratings yet
- Article. Rectal Carcinoma-Imaging For Staging (2018)Document31 pagesArticle. Rectal Carcinoma-Imaging For Staging (2018)Trí Cương NguyễnNo ratings yet
- Simple. Fast. Precise. Empowering Point of Care.: e Pro EditionDocument6 pagesSimple. Fast. Precise. Empowering Point of Care.: e Pro EditionAgung Prio UtomoNo ratings yet
- Thesis Radiology TopicsDocument6 pagesThesis Radiology Topicsafbwrszxd100% (2)
- Ultrasound 2018 PDFDocument106 pagesUltrasound 2018 PDFSatrio N. W. Notoamidjojo100% (1)
- 2008 Gomez Ut Artery PIDocument5 pages2008 Gomez Ut Artery PIRibeiro SáNo ratings yet
- Cement Evaluation Tool: A New Approach To Cement EvaluationDocument7 pagesCement Evaluation Tool: A New Approach To Cement EvaluationMauro CostaNo ratings yet
- Ped&kid&dis&gea&sch&2nd PDFDocument1,968 pagesPed&kid&dis&gea&sch&2nd PDFAna-Mihaela BalanuțaNo ratings yet
- Manual de Servicio Ultraview 2202Document156 pagesManual de Servicio Ultraview 2202Yohn FaizerNo ratings yet
- Doppler PresentationDocument51 pagesDoppler PresentationPbawal100% (2)
- HRQ Common Interview QuestionsDocument2 pagesHRQ Common Interview QuestionsJing CruzNo ratings yet
- Ultrasound Guidance in Regional AnaesthesiaDocument261 pagesUltrasound Guidance in Regional AnaesthesiaMihai Perescu100% (2)
- Voluson™ P8 / Voluson™ P6: Basic Service ManualDocument384 pagesVoluson™ P8 / Voluson™ P6: Basic Service Manualthaiduong buiquangNo ratings yet
- DEEP Vein ThrombosisDocument72 pagesDEEP Vein ThrombosisLevy Garcia SanchezNo ratings yet
- Clinical Chest UltrasoundDocument228 pagesClinical Chest UltrasoundBulborea Mihaela67% (3)
- Voluson S6 Data SheetDocument15 pagesVoluson S6 Data SheetNanang YlNo ratings yet
- UT L3 Question BankDocument62 pagesUT L3 Question BankJiten Karmakar75% (4)
- Della Core DutiesDocument12 pagesDella Core DutiesSt SNo ratings yet
- Ul BR Aplio A550Document20 pagesUl BR Aplio A550JC 89No ratings yet
- Answer Key 5Document9 pagesAnswer Key 5Sajjala Poojith reddyNo ratings yet
- Ulite Brosura PDFDocument12 pagesUlite Brosura PDFAdryana StefyNo ratings yet
- Tests of Backscatter Coefficient Measurement Using Broadband PulsesDocument5 pagesTests of Backscatter Coefficient Measurement Using Broadband PulsesMostafa AbdelrahmanNo ratings yet
- VIVID E95 4D SpesifikasiDocument2 pagesVIVID E95 4D SpesifikasiTopan AssyNo ratings yet
- SONOCAREDocument2 pagesSONOCAREArun SivamNo ratings yet