You might also like
- Avatar Neytiri 1Document48 pagesAvatar Neytiri 1Jheix Diniz100% (5)
- ACR Thyroid Imaging, Reporting and Data 2018 TesslerDocument9 pagesACR Thyroid Imaging, Reporting and Data 2018 TesslerdianaveebaeNo ratings yet
- 11 - Topic 20 Organic Chemistry AnswersDocument60 pages11 - Topic 20 Organic Chemistry AnswersNeen NaazNo ratings yet
- Biomarkers HER2+ MBCDocument30 pagesBiomarkers HER2+ MBChiroshima123No ratings yet
- 1 s2.0 S1078143923000893 MainDocument9 pages1 s2.0 S1078143923000893 MainJulio MineraNo ratings yet
- Trial: Tailorx: Trial Assigning Individualized Options For Treatment (RX)Document4 pagesTrial: Tailorx: Trial Assigning Individualized Options For Treatment (RX)Natalia QuinteroNo ratings yet
- Brachytherapy Boost (BT-boost) or Stereotactic Body Radiation Therapy Boost (SBRT-boost) For High-Risk Prostate Cancer (HR-PCa)Document10 pagesBrachytherapy Boost (BT-boost) or Stereotactic Body Radiation Therapy Boost (SBRT-boost) For High-Risk Prostate Cancer (HR-PCa)Oncología CdsNo ratings yet
- Cleopatra InicialDocument21 pagesCleopatra InicialAndersson SaenzNo ratings yet
- 2.4.B DR Denni Clinical Evidence of Ribociclib Into Clinical PracticeDocument40 pages2.4.B DR Denni Clinical Evidence of Ribociclib Into Clinical Practicetepat rshsNo ratings yet
- Abstracts: Annals of OncologyDocument1 pageAbstracts: Annals of OncologyAsaikkutti AnnamalaiNo ratings yet
- Tucatinib, Trastuzumab, and Capecitabine For HER2-Positive Metastatic Breast CancerDocument13 pagesTucatinib, Trastuzumab, and Capecitabine For HER2-Positive Metastatic Breast Cancertpatel0986No ratings yet
- Comparative Effectiveness of Primary Radiotherapy Versus Surgery in ElderlyDocument9 pagesComparative Effectiveness of Primary Radiotherapy Versus Surgery in ElderlyBárbara Meza LewisNo ratings yet
- Impower 132Document12 pagesImpower 132linxiaNo ratings yet
- Gastrointestinal Tumours, Colorectal: 555P Integrated Safety Summary (ISS) For Trifluridine/tipiracil (TAS-102)Document1 pageGastrointestinal Tumours, Colorectal: 555P Integrated Safety Summary (ISS) For Trifluridine/tipiracil (TAS-102)Amina GoharyNo ratings yet
- The Breast: SciencedirectDocument9 pagesThe Breast: SciencedirectFrengky MaweaNo ratings yet
- ARM AR2021 FINAL-singlesDocument40 pagesARM AR2021 FINAL-singlesYefinadya MfNo ratings yet
- Early Breast Cancer Prognostic Options Including CanAssistDocument49 pagesEarly Breast Cancer Prognostic Options Including CanAssistIndranil GhoshNo ratings yet
- Seminars in Oncology: Lauren Chiec, Ami N. ShahDocument10 pagesSeminars in Oncology: Lauren Chiec, Ami N. ShahNelson William UsnayoNo ratings yet
- PD-1 and PD-L1 Expression Predicts Radiosensitivity and Clinical Outcomes in Head and Neck Cancer and Is Associated With HPV InfectionDocument12 pagesPD-1 and PD-L1 Expression Predicts Radiosensitivity and Clinical Outcomes in Head and Neck Cancer and Is Associated With HPV InfectionApriliza RalasatiNo ratings yet
- Differentiated Thyroid Cancer: How Do Current Practice Guidelines Affect Management?Document8 pagesDifferentiated Thyroid Cancer: How Do Current Practice Guidelines Affect Management?wafasahilahNo ratings yet
- New Treatment Options For Metastatic Thyroid CancerDocument6 pagesNew Treatment Options For Metastatic Thyroid CancermarcelinaNo ratings yet
- Biblio 13Document6 pagesBiblio 13ManganusNo ratings yet
- The Role of Post-RT FDG PET in Neck Dissection For Regionally Advanced Head and Neck Cancer (PDFDrive)Document165 pagesThe Role of Post-RT FDG PET in Neck Dissection For Regionally Advanced Head and Neck Cancer (PDFDrive)Bianca DanielaNo ratings yet
- Comparison of Medical Therapy Alone ToDocument9 pagesComparison of Medical Therapy Alone ToTeuku Ahmad HasanyNo ratings yet
- Koay 2020Document30 pagesKoay 2020Laura QuirozNo ratings yet
- Tirads NuevoDocument13 pagesTirads NuevoLuisMamaniTercerosNo ratings yet
- Breast CancerhggDocument20 pagesBreast CancerhggCatherine RajanNo ratings yet
- Adjuvant Pertuzumab and Trastuzumab in Early HER2-Positive Breast CancerDocument10 pagesAdjuvant Pertuzumab and Trastuzumab in Early HER2-Positive Breast Cancerfaris nagibNo ratings yet
- ACR TI-RADS: Pitfalls, Solutions, and Future DirectionsDocument13 pagesACR TI-RADS: Pitfalls, Solutions, and Future Directionsmapeos tiroides100% (1)
- Zapatero 1580 FINALDocument5 pagesZapatero 1580 FINALJohn SlorNo ratings yet
- Current Therapies For Human Epidermal Growth Factor Receptor 2-Positive Metastatic Breast Cancer PatientsDocument17 pagesCurrent Therapies For Human Epidermal Growth Factor Receptor 2-Positive Metastatic Breast Cancer PatientsmrsilNo ratings yet
- D'Amico Risk ClassificationDocument6 pagesD'Amico Risk ClassificationStirNo ratings yet
- PrEP RiveraDocument12 pagesPrEP RiveraSeptian 99No ratings yet
- TIRADS2017Document9 pagesTIRADS2017Eliana RuizNo ratings yet
- MainDocument8 pagesMainIoana CucuNo ratings yet
- The Addition of Paclitaxel To Doxorubicin and Cisplatin and Cispalatin Volume Directed RadiationDocument21 pagesThe Addition of Paclitaxel To Doxorubicin and Cisplatin and Cispalatin Volume Directed RadiationGarsa GarnolNo ratings yet
- Developing A Clinically Important Class of Glycan-Targeted Biologics With Unprecedented Tumor Specificity Funding First Human DataDocument17 pagesDeveloping A Clinically Important Class of Glycan-Targeted Biologics With Unprecedented Tumor Specificity Funding First Human DataNuno Prego RamosNo ratings yet
- Thyroid GuidelinesDocument43 pagesThyroid GuidelinesNathaly LapoNo ratings yet
- Trastuzumab Deruxtecan in Previously Treated HER2-Positive Breast CancerDocument12 pagesTrastuzumab Deruxtecan in Previously Treated HER2-Positive Breast CancerRocio SolervicensNo ratings yet
- FENG Et Al., 2011Document7 pagesFENG Et Al., 2011Weslay Rodrigues da SilvaNo ratings yet
- Clinical InvestigationDocument9 pagesClinical InvestigationOncología CdsNo ratings yet
- CNS Met From HER2+ BCDocument27 pagesCNS Met From HER2+ BChiroshima123No ratings yet
- Identification of Five Cytotoxicity-Related GenesDocument12 pagesIdentification of Five Cytotoxicity-Related GenesFiona TranNo ratings yet
- cOASIS, The Online Abstract Submission SystemDocument2 pagescOASIS, The Online Abstract Submission SystemPuig CozarNo ratings yet
- Jamaoncology Vinayak 2019 Oi 190028Document9 pagesJamaoncology Vinayak 2019 Oi 190028Noema AmorochoNo ratings yet
- Creating Vibrant EcosystemDocument7 pagesCreating Vibrant Ecosystem周一行No ratings yet
- 3.4. Hypofractionated-Prostate - 60 - 20ses - y - 70 - 28sesDocument12 pages3.4. Hypofractionated-Prostate - 60 - 20ses - y - 70 - 28sesMigue PerezNo ratings yet
- The Evolving Role of Immunotherapy As A Component of Multimodal Therapy in Earlier Stages of Lung CancerDocument59 pagesThe Evolving Role of Immunotherapy As A Component of Multimodal Therapy in Earlier Stages of Lung CancerRiya ChaturvediNo ratings yet
- Current Controversies in The Initial Post-Surgical Radioactive Iodine Therapy For Thyroid Cancer: A Narrative ReviewDocument12 pagesCurrent Controversies in The Initial Post-Surgical Radioactive Iodine Therapy For Thyroid Cancer: A Narrative ReviewAura GorneaNo ratings yet
- Gene Expression Signature To Inform On Adjuvant Treatment: Maria Vittoria DieciDocument43 pagesGene Expression Signature To Inform On Adjuvant Treatment: Maria Vittoria DiecihsfbjbfsNo ratings yet
- CDK Luminal ABCDocument85 pagesCDK Luminal ABCSusanto SalimNo ratings yet
- Hoskin Et Al., 2012 UK TrialDocument6 pagesHoskin Et Al., 2012 UK TrialandresNo ratings yet
- Monday KordeDocument19 pagesMonday KordeNational Press FoundationNo ratings yet
- Abdollah 2018Document4 pagesAbdollah 2018Neetumishti ChadhaNo ratings yet
- Comparison of Elastic and Rigid Registration During MRI US Fusion Guided Prostate BiopsyDocument2 pagesComparison of Elastic and Rigid Registration During MRI US Fusion Guided Prostate BiopsyWilson LozanoNo ratings yet
- Thyroid Fine Needle Aspirate - A Post-Bethesda UpdateDocument10 pagesThyroid Fine Needle Aspirate - A Post-Bethesda UpdateLaraNo ratings yet
- VOL. 129, NO. 5 (SUPPLEMENT), MAY 2017 Monday Posters 133SDocument2 pagesVOL. 129, NO. 5 (SUPPLEMENT), MAY 2017 Monday Posters 133STeguh SulistiyantoNo ratings yet
- Rce0321 Diop Cinv Webinar - FinalDocument48 pagesRce0321 Diop Cinv Webinar - Finalamaal ramadanNo ratings yet
- Tsao 2015Document26 pagesTsao 2015Ivan InkovNo ratings yet
- Triple-Negative Breast Cancer: A Clinician’s GuideFrom EverandTriple-Negative Breast Cancer: A Clinician’s GuideAntoinette R. TanNo ratings yet
- Targeted Therapies for Lung CancerFrom EverandTargeted Therapies for Lung CancerRavi SalgiaNo ratings yet
- MedComm - 2024 - Yuan - Perioperative Immunotherapy The Main Clinical Treatment For Resectable Non Small Cell Lung CancerDocument4 pagesMedComm - 2024 - Yuan - Perioperative Immunotherapy The Main Clinical Treatment For Resectable Non Small Cell Lung CancerMihary RamanandraitsioryNo ratings yet
- Thoracic 428 Edited2Document87 pagesThoracic 428 Edited2Mihary RamanandraitsioryNo ratings yet
- 10 1093-Bja-85 3 462figureDocument3 pages10 1093-Bja-85 3 462figureMihary RamanandraitsioryNo ratings yet
- 10 1053-j Optechstcvs 2012 03 001figureDocument11 pages10 1053-j Optechstcvs 2012 03 001figureMihary RamanandraitsioryNo ratings yet
- 10 1046-j 1440-1843 1999 00154 Xfigure4Document1 page10 1046-j 1440-1843 1999 00154 Xfigure4Mihary RamanandraitsioryNo ratings yet
- 10 1016-j Jtcvs 2009 03 055figureDocument4 pages10 1016-j Jtcvs 2009 03 055figureMihary RamanandraitsioryNo ratings yet
- Rojo CateringDocument2 pagesRojo Cateringsupport_local_flavorNo ratings yet
- D12D380, Em-Ec96 - Esa - 02 - 586088Document2 pagesD12D380, Em-Ec96 - Esa - 02 - 586088asif basha100% (2)
- Installation Manual: Energy Recovery VentilatorDocument24 pagesInstallation Manual: Energy Recovery VentilatorBryan HuNo ratings yet
- Separation and Purification of Organic CompoundsDocument3 pagesSeparation and Purification of Organic CompoundsDyaharra AgangNo ratings yet
- Run To Failure / Breakdown Maintenance. - Planned / Calendar Based Preventive' Maintenance (PM) - Predictive Maintenance (PDM)Document30 pagesRun To Failure / Breakdown Maintenance. - Planned / Calendar Based Preventive' Maintenance (PM) - Predictive Maintenance (PDM)Chetan PatilNo ratings yet
- Fire Safety in The Home - JGDocument2 pagesFire Safety in The Home - JGJamieGillumNo ratings yet
- FIITJEE Admission Tests '2013Document4 pagesFIITJEE Admission Tests '2013FIITJEE Mumbai Centre100% (4)
- CRH Dietary Policies and Procedures.11.2014 Final PDFDocument325 pagesCRH Dietary Policies and Procedures.11.2014 Final PDFShivanipandey100% (2)
- Report On Attendance: Isabela Colleges, IncDocument2 pagesReport On Attendance: Isabela Colleges, IncAnnabelle Dasalla DomingoNo ratings yet
- Job Satisfaction and Acculturation Among Filipino Registered Nurses Request PDFDocument1 pageJob Satisfaction and Acculturation Among Filipino Registered Nurses Request PDFMelissa Barrientos SimanganNo ratings yet
- Marine Paint Guide: 5. Safety PrecautionsDocument3 pagesMarine Paint Guide: 5. Safety PrecautionsPolaris BridgemanNo ratings yet
- Carbon Fiber vs. Metal FrameworkDocument14 pagesCarbon Fiber vs. Metal FrameworkDental Del NorteNo ratings yet
- Alkaline Earth Metals and Their Uses Chemistry ProjectDocument9 pagesAlkaline Earth Metals and Their Uses Chemistry ProjectINo ratings yet
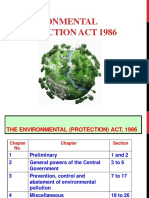
- The Environmental Protection ActDocument48 pagesThe Environmental Protection ActEco Electrotech SolutionsNo ratings yet
- Serology NewDocument116 pagesSerology NewFarlogyNo ratings yet
- PsychologicaldisorderprojectDocument18 pagesPsychologicaldisorderprojectapi-273867984No ratings yet
- 2021版MobiEye 700 H-046-007582-01 DR60使用说明书(英文)-153-200Document48 pages2021版MobiEye 700 H-046-007582-01 DR60使用说明书(英文)-153-200javo599No ratings yet
- Lab Diagnosis of NeoplasiaDocument14 pagesLab Diagnosis of Neoplasiasapphiresia100% (6)
- NEET For PlanDocument1 pageNEET For PlanshivendrakumarNo ratings yet
- 1 13.8 Kv. 1 69 KVDocument35 pages1 13.8 Kv. 1 69 KVDedy SubagyoNo ratings yet
- Final Programme 2016 WEB ADDocument204 pagesFinal Programme 2016 WEB ADNahui IcatlNo ratings yet
- S Stage 6 p840 Ms AfpDocument18 pagesS Stage 6 p840 Ms AfpMCH100% (4)
- Positioning Pressure ReliefDocument4 pagesPositioning Pressure Reliefapi-455513786No ratings yet
- 1610130042Document2 pages1610130042Kuldeep ShrivastavaNo ratings yet
- Soil Test LevelsDocument8 pagesSoil Test LevelsAhmed abd elkaderNo ratings yet
- Overview of Common Nutritional Disorders of Captive Reptiles PDFDocument9 pagesOverview of Common Nutritional Disorders of Captive Reptiles PDFDhasiaNo ratings yet
- Hustle Culture and The Implications For Our WorkforceDocument54 pagesHustle Culture and The Implications For Our WorkforceDYMAS PRASETIYONo ratings yet
- Graetz Probesx5cplus PDFDocument2 pagesGraetz Probesx5cplus PDFjvillert2No ratings yet