You might also like
- Invertebrate ZoologyDocument1,016 pagesInvertebrate ZoologyRACHANA PURKAYASTHA 2140623No ratings yet
- Yoga For Skin Diseases Anna MayerDocument22 pagesYoga For Skin Diseases Anna Mayerjaideep negi100% (1)
- Derma NotesDocument52 pagesDerma NotesUsmanNo ratings yet
- Dermatology Class NotesDocument48 pagesDermatology Class Notesapi-26938624100% (6)
- Littelfuse EVI EV Charging Infrastructure Presentation PDFDocument19 pagesLittelfuse EVI EV Charging Infrastructure Presentation PDFRaka Pratindy100% (1)
- Viral and Bacterial Infections of The SkinDocument200 pagesViral and Bacterial Infections of The SkinKarla Jane100% (1)
- Q.1 Components of Skin: The Skin: Basic Structure and FunctionDocument7 pagesQ.1 Components of Skin: The Skin: Basic Structure and Functionnani100No ratings yet
- Distance Relay BasicsDocument58 pagesDistance Relay Basicsaalamz93_854917254100% (1)
- 3.skin PathologyDocument38 pages3.skin PathologyFaisal MehboobNo ratings yet
- SKIN DISORDERS AND DISEASES HandoutsDocument9 pagesSKIN DISORDERS AND DISEASES HandoutsMARIALUPE ESTOQUENo ratings yet
- Graha YuddhaDocument10 pagesGraha YuddhaHeather WilliamsNo ratings yet
- 1926 PapionianDocument108 pages1926 PapionianPLCS_FoundationNo ratings yet
- 547 2094 1 PB PDFDocument8 pages547 2094 1 PB PDFYesichaNo ratings yet
- Acne VulgarisDocument60 pagesAcne Vulgarischarmaine_olivia_1100% (2)
- Quiz 2 Principles of DesignDocument4 pagesQuiz 2 Principles of DesignJovito Reyes0% (1)
- Test Engleza Clasa A5a Modul 3Document3 pagesTest Engleza Clasa A5a Modul 3Adelina HasasNo ratings yet
- Skin-PathologyDocument32 pagesSkin-PathologyArfa BaigNo ratings yet
- Disorders of Sebaceous GlandDocument54 pagesDisorders of Sebaceous GlandAnurag PandeyNo ratings yet
- Pediatric Disorders of The Integumentary SystemDocument70 pagesPediatric Disorders of The Integumentary SystemJezreel OrquinaNo ratings yet
- DERMATOLOGY QuinterDocument177 pagesDERMATOLOGY QuinterstaceyatienoomaNo ratings yet
- Skin Conditions Part II-1Document54 pagesSkin Conditions Part II-1mohamedkallon1996No ratings yet
- Clinical Overview of Acne Vulgaris: Rich Callahan MSPA, PA-C ICM I - Summer 2009Document22 pagesClinical Overview of Acne Vulgaris: Rich Callahan MSPA, PA-C ICM I - Summer 2009Christopher DennisNo ratings yet
- Commonskindiseases 150110033432 Conversion Gate02 1Document70 pagesCommonskindiseases 150110033432 Conversion Gate02 1Dr. Siraphop OneSongchai RatanasubanNo ratings yet
- Dermatosis-WPS Office-1Document111 pagesDermatosis-WPS Office-1PriyaNo ratings yet
- Meth Elab Topic N2Document19 pagesMeth Elab Topic N2Group M1869No ratings yet
- Psoriasis BBBDocument28 pagesPsoriasis BBBPramod ChoudharyNo ratings yet
- Integumentary SystemDocument44 pagesIntegumentary SystemAnonymous -No ratings yet
- Dermatological Conditions KOROS E.k-1Document107 pagesDermatological Conditions KOROS E.k-1victorNo ratings yet
- Medsurg 7 Assessment: Integumentary System: Structures and FunctionsDocument7 pagesMedsurg 7 Assessment: Integumentary System: Structures and FunctionsjefrocNo ratings yet
- AbscessDocument4 pagesAbscessShivBalakChauhanNo ratings yet
- Superficial Mycoses Group 4Document38 pagesSuperficial Mycoses Group 4prudence azenaborNo ratings yet
- Presentation Advanced TechnologyDocument26 pagesPresentation Advanced Technologyahmad allalaNo ratings yet
- Bacterial - Viral InfectionsDocument61 pagesBacterial - Viral InfectionsMoayad NawaflehNo ratings yet
- Diseases of SkinDocument18 pagesDiseases of SkinrishikeshkallaNo ratings yet
- Acne VulgarisDocument45 pagesAcne VulgarisKeith OmwoyoNo ratings yet
- Skin An Essential Organ-IIDocument30 pagesSkin An Essential Organ-IIsameen tahirNo ratings yet
- Dermatology 1Document47 pagesDermatology 1Edwin OkonNo ratings yet
- Skin DisordersDocument202 pagesSkin DisordersMj Briones100% (1)
- Continuing Medical Education: Amanda M M Oakley MBCHB Fracp DiphealinfDocument4 pagesContinuing Medical Education: Amanda M M Oakley MBCHB Fracp DiphealinfCarol SantosNo ratings yet
- Minor Skin and Soft Tissue TumorsDocument27 pagesMinor Skin and Soft Tissue TumorsLouie BelloNo ratings yet
- Acne VulgarisDocument58 pagesAcne VulgarisNargisNo ratings yet
- MycosesDocument28 pagesMycosesAiman TymerNo ratings yet
- Overview of Skin InfectionsDocument53 pagesOverview of Skin Infectionsadamu mohammadNo ratings yet
- ParasiticDocument106 pagesParasitichelloaNo ratings yet
- Dermatology 2010 2011Document28 pagesDermatology 2010 2011Qasim HaleimiNo ratings yet
- IntegumentaryDocument54 pagesIntegumentaryA-Mark Gabriel PesanteNo ratings yet
- Chapter 4: Examination of The Skin, Coat and Associated StructuresDocument19 pagesChapter 4: Examination of The Skin, Coat and Associated StructuresZekarias GetachewNo ratings yet
- Fungal Infections-MlcDocument31 pagesFungal Infections-Mlcsamuel gathenyaNo ratings yet
- Integumentary System PhysioDocument53 pagesIntegumentary System PhysioMhykhaela CaparasNo ratings yet
- GENOVE, ERICKA IS-Module2Document11 pagesGENOVE, ERICKA IS-Module2Ericka GenoveNo ratings yet
- Important Diseases1 - Skin and EyeDocument40 pagesImportant Diseases1 - Skin and EyePeiyong TanNo ratings yet
- ACNEDocument20 pagesACNEShreyas WalvekarNo ratings yet
- CHAPTER V: Pathogenic Microorganisms: Pathogens That Enter The Body Through The SkinDocument6 pagesCHAPTER V: Pathogenic Microorganisms: Pathogens That Enter The Body Through The SkinKarla Karina Dela CruzNo ratings yet
- Acne and Rosacea: AetiologyDocument7 pagesAcne and Rosacea: AetiologyananNo ratings yet
- Presentasi Kasus Acne VulgarisDocument27 pagesPresentasi Kasus Acne VulgarisAndi Rizki TenryayuNo ratings yet
- S96 CKS Acne VulgarisDocument41 pagesS96 CKS Acne VulgarisGabriel CampolinaNo ratings yet
- Module 3 HomeworkDocument6 pagesModule 3 HomeworkCj LinceNo ratings yet
- 2022 MIKRO - INTEGUMEN BakteriDocument47 pages2022 MIKRO - INTEGUMEN BakterifatharaniNo ratings yet
- Common Skin Dis WPS OfficeDocument17 pagesCommon Skin Dis WPS OfficeJoan JumawanNo ratings yet
- Prev Next: © 2014 Webmd, Llc. All Rights ReservedDocument5 pagesPrev Next: © 2014 Webmd, Llc. All Rights ReservedOlfaktorius GoenawanNo ratings yet
- Fungal ClassificationDocument109 pagesFungal ClassificationMirza Shaharyar BaigNo ratings yet
- Chapter III - Dermatology: Common Skin Conditions and PathologyDocument5 pagesChapter III - Dermatology: Common Skin Conditions and PathologyIndranil SinhaNo ratings yet
- Lecture Note 2A DISEASES OF THE SKIN AND EYEDocument8 pagesLecture Note 2A DISEASES OF THE SKIN AND EYERAFAELLA SALVE MARIE GAETOSNo ratings yet
- Q3 - Perform Facial TreatmentDocument19 pagesQ3 - Perform Facial TreatmentAzucenas, Mycha Blace V.No ratings yet
- Week 5. Superficial, Systemic, & Opportunistic MycosesDocument73 pagesWeek 5. Superficial, Systemic, & Opportunistic MycosesAsdfghjklNo ratings yet
- Micr Biology: Microbial Diseases of The Skin and EyesDocument62 pagesMicr Biology: Microbial Diseases of The Skin and EyesIvy L VonierNo ratings yet
- KIN LONG Shower Screen CatalogueDocument58 pagesKIN LONG Shower Screen CatalogueFaiz ZentNo ratings yet
- Apple Computer Inc. v. Burst - Com, Inc. - Document No. 146Document39 pagesApple Computer Inc. v. Burst - Com, Inc. - Document No. 146Justia.comNo ratings yet
- Case How Innovation Drives Research and DevelopmentDocument4 pagesCase How Innovation Drives Research and DevelopmentMohit KumarNo ratings yet
- Dr. M. Syed Jamil Asghar: Paper Published: 80Document6 pagesDr. M. Syed Jamil Asghar: Paper Published: 80Awaiz NoorNo ratings yet
- Benguet Folktales Bases For Tracing Family BloodlineDocument17 pagesBenguet Folktales Bases For Tracing Family BloodlineJohn Rey PelilaNo ratings yet
- IM300-20 (LCMass RHE 14) PDFDocument40 pagesIM300-20 (LCMass RHE 14) PDFLazzarus Az GunawanNo ratings yet
- 4K Resolution: The Future of ResolutionsDocument15 pages4K Resolution: The Future of ResolutionsRavi JoshiNo ratings yet
- Geographic Information Systems and Science-GoodchildDocument8 pagesGeographic Information Systems and Science-GoodchildChoc OlateNo ratings yet
- 413 1684 1 PB PDFDocument5 pages413 1684 1 PB PDFMhd RidwanNo ratings yet
- Unit P1, P1.1: The Transfer of Energy by Heating ProcessesDocument9 pagesUnit P1, P1.1: The Transfer of Energy by Heating ProcessesTemilola OwolabiNo ratings yet
- ShimadzuDocument66 pagesShimadzueka_setyowati0No ratings yet
- Doosan Dielsel Forklift d35s 7 d40s 7 d45s 7 d50c 7 d55c 7 d40sc 7 d45sc 7 d50sc 7 d55sc 7 Part Book Sb1223e01Document22 pagesDoosan Dielsel Forklift d35s 7 d40s 7 d45s 7 d50c 7 d55c 7 d40sc 7 d45sc 7 d50sc 7 d55sc 7 Part Book Sb1223e01daleherrera100788nke100% (23)
- Embryo AssignmentDocument2 pagesEmbryo AssignmentA.j. MasagcaNo ratings yet
- GFB V2 - VNT Boost Controller: (Part # 3009)Document2 pagesGFB V2 - VNT Boost Controller: (Part # 3009)blumng100% (1)
- Turcite T51 Engineering DataDocument1 pageTurcite T51 Engineering DataAntonio Rivera VillavicencioNo ratings yet
- Cyclic VoltammetryDocument4 pagesCyclic Voltammetryreddynivas100% (1)
- QuizBowl QuestionsDocument84 pagesQuizBowl QuestionsJowel MercadoNo ratings yet
- Hemiplegia Case 18.12.21Document5 pagesHemiplegia Case 18.12.21Beedhan KandelNo ratings yet
- Mcbe2798 e 10 1Document42 pagesMcbe2798 e 10 1Manh DuyNo ratings yet
- 15b. FANC - Focused Antenatal Care - Koros E.KDocument71 pages15b. FANC - Focused Antenatal Care - Koros E.KMercy KeruboNo ratings yet
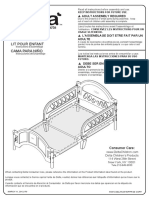
- BB204-Toddler Bed Assembly InstructionsDocument10 pagesBB204-Toddler Bed Assembly InstructionsCaloi PastorfideNo ratings yet
- 7th Chemistry DLP Study Package FinalDocument101 pages7th Chemistry DLP Study Package FinalAdityaNo ratings yet
- Jammer Final Report Mod PDFDocument41 pagesJammer Final Report Mod PDFNourhanGamalNo ratings yet