You might also like
- Maternal Anatomy WilliamsDocument60 pagesMaternal Anatomy WilliamsZari Novela100% (2)
- Pathophysiology OsteosarcomaDocument4 pagesPathophysiology OsteosarcomaGladys Barcelona0% (1)
- Surgical Wound ClassificationDocument1 pageSurgical Wound Classificationgeclear323No ratings yet
- Inguinal Canal: DR - Lubna NazliDocument28 pagesInguinal Canal: DR - Lubna NazliAhmed AminNo ratings yet
- Sahitya Snigdha (Hernia Module)Document159 pagesSahitya Snigdha (Hernia Module)h9pkyd9dg9No ratings yet
- Anatomy of GIT For PCII Students..Document106 pagesAnatomy of GIT For PCII Students..AMANUEL HABTEWOLDNo ratings yet
- Abdominal WallDocument56 pagesAbdominal WallAHMAD KHANNo ratings yet
- Hernia: Dr. NachmanyDocument69 pagesHernia: Dr. NachmanyDvir AviramNo ratings yet
- Inguinal CanalDocument16 pagesInguinal Canalabdul haseebNo ratings yet
- Female PerineumDocument27 pagesFemale Perineumkaartikey dubeNo ratings yet
- Anterolateral Abdominal Wall and Abdominal IncisionsDocument42 pagesAnterolateral Abdominal Wall and Abdominal IncisionsSamar AhmadNo ratings yet
- Inguinal Canal and ScrotumDocument55 pagesInguinal Canal and ScrotumAuza Moses IbrahimNo ratings yet
- Anatomy of The Abdomen: Samara University Biomedical Sciences DepartmentDocument142 pagesAnatomy of The Abdomen: Samara University Biomedical Sciences Departmentfentaw melkieNo ratings yet
- Hernia FTDDocument71 pagesHernia FTDEmmanuel Papa AcquahNo ratings yet
- Vagina Anat, Episiotomy and MGMT of Cervical TearDocument50 pagesVagina Anat, Episiotomy and MGMT of Cervical TearCapricious BibekNo ratings yet
- 3-Inguinal Canal PDFDocument58 pages3-Inguinal Canal PDFN A0% (1)
- Anatomy of The AbdomenDocument107 pagesAnatomy of The AbdomenmichaelhossianNo ratings yet
- Abdominal WallDocument75 pagesAbdominal WallJojo RyelciusNo ratings yet
- Inguinal Hernias: Trix M. Asuncion M.D. General SurgeryDocument55 pagesInguinal Hernias: Trix M. Asuncion M.D. General Surgeryjitendra magarNo ratings yet
- General AnatomyDocument46 pagesGeneral AnatomyIhab IsmailNo ratings yet
- Perineal TearsDocument49 pagesPerineal TearsvisakhaNo ratings yet
- Abdominal Wall and HerniaDocument35 pagesAbdominal Wall and HerniaMohammad BanisalmanNo ratings yet
- Dinding Abdomen PSIKDocument79 pagesDinding Abdomen PSIKSondang DamanikNo ratings yet
- Inguinal CanalDocument22 pagesInguinal CanalAaryan PatelNo ratings yet
- Anterior Abdominal WallDocument24 pagesAnterior Abdominal WallIAMSANWAR019170No ratings yet
- Pelvic Diaphragm & Pelvic FasciaDocument22 pagesPelvic Diaphragm & Pelvic Fasciafarwafurqan1No ratings yet
- Ischiorectal Fossa Anatomy and It's Suppuration: DR - Niveditha S Dr.S.Chandak DR - Melissa P Dr.C.MahkalkarDocument18 pagesIschiorectal Fossa Anatomy and It's Suppuration: DR - Niveditha S Dr.S.Chandak DR - Melissa P Dr.C.MahkalkarSagarRathodNo ratings yet
- Anatomi PelvisDocument44 pagesAnatomi Pelvisari naNo ratings yet
- PELVIS AND PERINEUM Session 4 - 2022Document53 pagesPELVIS AND PERINEUM Session 4 - 2022zealotwisdom0No ratings yet
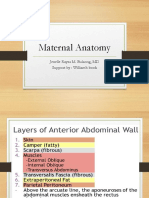
- Maternal Anatomy: Julao, Fritz Adrian C. Kho, Nicole Alexandra P. Lagmay, Paul Angelo ADocument115 pagesMaternal Anatomy: Julao, Fritz Adrian C. Kho, Nicole Alexandra P. Lagmay, Paul Angelo ANicole Alexandra KhoNo ratings yet
- 2 Inguinal Region DiyaDocument31 pages2 Inguinal Region DiyaOmotosho DavidNo ratings yet
- Inguinal Hernia Ana PhyDocument16 pagesInguinal Hernia Ana PhyJay Marie GonzagaNo ratings yet
- Inguinal Hernia FinalDocument42 pagesInguinal Hernia FinalRajath Kumar K R KNo ratings yet
- Abdomen - IntroductionDocument63 pagesAbdomen - IntroductionPriyanka SharmaNo ratings yet
- Perineum: Dr. Edi Patmini SS, Spog/Dr. M. Nurhadi Rahman, SpogDocument16 pagesPerineum: Dr. Edi Patmini SS, Spog/Dr. M. Nurhadi Rahman, Spogpuskesmas gebangNo ratings yet
- Lec.1.Anatomy of PregnancyDocument53 pagesLec.1.Anatomy of PregnancyManal AsadNo ratings yet
- Internal Oblique Muscle: Nerve SupplyDocument1 pageInternal Oblique Muscle: Nerve SupplyBogdan Robert CNo ratings yet
- Anatomy For Groin Hernia RepairDocument69 pagesAnatomy For Groin Hernia RepairROUNAK MEHROTRANo ratings yet
- Perineum and UG TriangleDocument27 pagesPerineum and UG TriangleAbiola NerdNo ratings yet
- Abdomen and Abdominal WallDocument40 pagesAbdomen and Abdominal WallAlex ChagalaNo ratings yet
- P. Cavity: (Female Reproductive Organs)Document38 pagesP. Cavity: (Female Reproductive Organs)SAKARIYE MAXAMEDNo ratings yet
- 20 RectumDocument125 pages20 RectumBibek GajmerNo ratings yet
- Surgical-ANATOMY OF Anterior Abdominal WallDocument83 pagesSurgical-ANATOMY OF Anterior Abdominal WallSyed Irfan ArifNo ratings yet
- Rectus Abdominis: Perp by Lect: S Hassn AskariDocument21 pagesRectus Abdominis: Perp by Lect: S Hassn AskariShimmering MoonNo ratings yet
- The Perineum: Dr:Ahmed Ibrahim Abdi (Nawawi) AnatomistDocument21 pagesThe Perineum: Dr:Ahmed Ibrahim Abdi (Nawawi) AnatomistSAKARIYE MAXAMEDNo ratings yet
- The AbdomenDocument67 pagesThe AbdomenOriade TaiwoNo ratings yet
- Inguinal Canal: Medial One-Half of The Inguinal Ligament Also Known As Poupart LigamentDocument4 pagesInguinal Canal: Medial One-Half of The Inguinal Ligament Also Known As Poupart LigamentDivya RanasariaNo ratings yet
- The Pelvis IiDocument25 pagesThe Pelvis IiFaith ChepoghishoNo ratings yet
- PelvisDocument35 pagesPelvisAdan ImanNo ratings yet
- 4rd Lecture - AbdomenDocument26 pages4rd Lecture - AbdomenZainab Jamal SiddiquiNo ratings yet
- Pelvic WallDocument56 pagesPelvic WallYousef El bannaNo ratings yet
- Abdomen Engl PDFDocument51 pagesAbdomen Engl PDFShuler0071No ratings yet
- Ureter, Urinary Bladder.Document16 pagesUreter, Urinary Bladder.Shimmering MoonNo ratings yet
- Deep PouchDocument12 pagesDeep PouchBalaji KarunakaranNo ratings yet
- Uterus and Ovary UltrasoundDocument144 pagesUterus and Ovary Ultrasoundisicheipraise3No ratings yet
- Abdomen 2023Document131 pagesAbdomen 2023Fenot YBNo ratings yet
- 1 Introduction To The Pelvis and The Pelvic Peritoneum DIYADocument38 pages1 Introduction To The Pelvis and The Pelvic Peritoneum DIYAOmotosho DavidNo ratings yet
- 5 The Perineum DiyaDocument35 pages5 The Perineum DiyaOmotosho DavidNo ratings yet
- Uterus, Tubes, Ovaries, VaginaDocument45 pagesUterus, Tubes, Ovaries, VaginasahrNo ratings yet
- Abdomen 1Document49 pagesAbdomen 1Cristina-Alexandra ConstantinNo ratings yet
- Abdominal Wall (Cont) : Dr. Qandeel Hamidullah KhanDocument25 pagesAbdominal Wall (Cont) : Dr. Qandeel Hamidullah Khanقندیل محسودNo ratings yet
- Anatomy and Pathoanatomic of Lumbosacral PlexusDocument33 pagesAnatomy and Pathoanatomic of Lumbosacral PlexusRachmad FaisalNo ratings yet
- Construction Law PresentationDocument5 pagesConstruction Law PresentationChoon Aik WeeNo ratings yet
- Recover at Work Plan 5 ProposedDocument2 pagesRecover at Work Plan 5 ProposedSiosiana DenhamNo ratings yet
- Radiation Induced Skin Reaction ManagementDocument7 pagesRadiation Induced Skin Reaction ManagementLokesh ViswanathNo ratings yet
- Indiana University Physical Education Lesson Plan: Robert Wilkinson (Squat Form)Document4 pagesIndiana University Physical Education Lesson Plan: Robert Wilkinson (Squat Form)api-402765215No ratings yet
- Current Evidence Does Not Support The Use of Kinesio Taping in Clinical Practice - A Systematic ReviewDocument9 pagesCurrent Evidence Does Not Support The Use of Kinesio Taping in Clinical Practice - A Systematic Reviewhrvoje09No ratings yet
- Ques NeboshDocument4 pagesQues Neboshanoop0% (1)
- 302 Hydrant TestDocument5 pages302 Hydrant Testsmartleo_waloNo ratings yet
- Product Catalog Bauerfeind Usa 0312Document88 pagesProduct Catalog Bauerfeind Usa 0312Guillermo Carpio FloriaNo ratings yet
- Printed LecturesDocument10 pagesPrinted LecturesCla SeNo ratings yet
- Ligaments HipDocument5 pagesLigaments HipRizka Kartikasari100% (1)
- Synchronous Motors 1FK7: Operating Instructions 03/2011Document58 pagesSynchronous Motors 1FK7: Operating Instructions 03/2011Krittaphak HacheyramNo ratings yet
- Risk Assessment/Management FormDocument4 pagesRisk Assessment/Management FormNazriNo ratings yet
- The One Ring - Online Character Sheet PDFDocument2 pagesThe One Ring - Online Character Sheet PDFJustinNo ratings yet
- General Pathology NotesDocument29 pagesGeneral Pathology NotesMohd Syaiful Mohd ArisNo ratings yet
- Recalls of Paper 2 - 11/9/2018: ConsentDocument6 pagesRecalls of Paper 2 - 11/9/2018: ConsentGiovanni Henry0% (1)
- Risk Assessment Matrix: ManualDocument13 pagesRisk Assessment Matrix: Manualck19654840100% (1)
- CREW: Department of Defense: Department of The Army: Regarding PTSD Diagnosis: 6/30/2011 - Release Pgs 1-241 On 24 May 2011Document241 pagesCREW: Department of Defense: Department of The Army: Regarding PTSD Diagnosis: 6/30/2011 - Release Pgs 1-241 On 24 May 2011CREWNo ratings yet
- DVT & PeDocument57 pagesDVT & PeRashed ShatnawiNo ratings yet
- InfanticideDocument28 pagesInfanticideJMac PadillaNo ratings yet
- 0000180Document53 pages0000180Nirmala MaranNo ratings yet
- Distal Femur (Sandeep Sir)Document22 pagesDistal Femur (Sandeep Sir)Kirubakaran Saraswathy PattabiramanNo ratings yet
- Arc Welder Risk MG T FormDocument9 pagesArc Welder Risk MG T FormMohd FikryNo ratings yet
- Orthobullet 2007 DDocument17 pagesOrthobullet 2007 DNanda GemaNo ratings yet
- ALSBLS PPT FinalDocument64 pagesALSBLS PPT FinalIbnu Fadirul WahedNo ratings yet
- Module Description. Pathology of Musculosceletal SystemDocument52 pagesModule Description. Pathology of Musculosceletal SystemAlberto MayorgaNo ratings yet
- CAUSATIONDocument54 pagesCAUSATIONgleeNo ratings yet
- Buku Koding 1Document74 pagesBuku Koding 1indra_igrNo ratings yet