You might also like
- Vagina Anat, Episiotomy and MGMT of Cervical TearDocument50 pagesVagina Anat, Episiotomy and MGMT of Cervical TearCapricious BibekNo ratings yet
- Maternal Anatomy: Julao, Fritz Adrian C. Kho, Nicole Alexandra P. Lagmay, Paul Angelo ADocument115 pagesMaternal Anatomy: Julao, Fritz Adrian C. Kho, Nicole Alexandra P. Lagmay, Paul Angelo ANicole Alexandra KhoNo ratings yet
- Female PerineumDocument27 pagesFemale Perineumkaartikey dubeNo ratings yet
- Sahitya Snigdha (Hernia Module)Document159 pagesSahitya Snigdha (Hernia Module)h9pkyd9dg9No ratings yet
- Hernia FTDDocument71 pagesHernia FTDEmmanuel Papa AcquahNo ratings yet
- Perineal TearsDocument49 pagesPerineal TearsvisakhaNo ratings yet
- Maternal Anatomy WilliamsDocument60 pagesMaternal Anatomy WilliamsZari Novela100% (2)
- Anatomi PelvisDocument44 pagesAnatomi Pelvisari naNo ratings yet
- Anterior Abdominal Wall& Inguinal Canal 2023 (1)Document26 pagesAnterior Abdominal Wall& Inguinal Canal 2023 (1)GanapathyGaneshNo ratings yet
- Abdominal WallDocument56 pagesAbdominal WallAHMAD KHANNo ratings yet
- Inguinal Canal and ScrotumDocument55 pagesInguinal Canal and ScrotumAuza Moses IbrahimNo ratings yet
- Surgical Anatomy-Anal Canal: Dr. Belal MansoorDocument79 pagesSurgical Anatomy-Anal Canal: Dr. Belal MansoorYogi drNo ratings yet
- 20 RectumDocument125 pages20 RectumBibek GajmerNo ratings yet
- Inguinal Canal: DR - Lubna NazliDocument28 pagesInguinal Canal: DR - Lubna NazliAhmed AminNo ratings yet
- External & Internal Generative Organs OrgansDocument78 pagesExternal & Internal Generative Organs OrgansdeevoncNo ratings yet
- Anatomical Considerations During G-Laparoscopic SurgeryDocument28 pagesAnatomical Considerations During G-Laparoscopic SurgeryMahia RahmanNo ratings yet
- Anatomy of the Perineum RegionDocument35 pagesAnatomy of the Perineum RegionOmotosho DavidNo ratings yet
- Perineum and UG TriangleDocument27 pagesPerineum and UG TriangleAbiola NerdNo ratings yet
- Anatomy of GIT For PCII Students..Document106 pagesAnatomy of GIT For PCII Students..AMANUEL HABTEWOLDNo ratings yet
- NECK1 Part OneDocument99 pagesNECK1 Part OneZelallem AnileyNo ratings yet
- Anatomy of The Abdomen: Samara University Biomedical Sciences DepartmentDocument142 pagesAnatomy of The Abdomen: Samara University Biomedical Sciences Departmentfentaw melkieNo ratings yet
- 2 Inguinal Region DiyaDocument31 pages2 Inguinal Region DiyaOmotosho DavidNo ratings yet
- PERINEUMDocument24 pagesPERINEUMmhr27112002No ratings yet
- Surgical Anatomy of the Anal CanalDocument69 pagesSurgical Anatomy of the Anal CanalVijaya Dwarampudi100% (1)
- The Perineum: Dr:Ahmed Ibrahim Abdi (Nawawi) AnatomistDocument21 pagesThe Perineum: Dr:Ahmed Ibrahim Abdi (Nawawi) AnatomistSAKARIYE MAXAMEDNo ratings yet
- Abdominal WallDocument75 pagesAbdominal WallJojo RyelciusNo ratings yet
- Jigjiga University: Anatomy of PerineumDocument114 pagesJigjiga University: Anatomy of PerineumKamal AhmedNo ratings yet
- Perineum AnatomyDocument23 pagesPerineum Anatomyrohitrohillapalwal999No ratings yet
- Maternal Anatomy External and Internal Generative OrgansDocument84 pagesMaternal Anatomy External and Internal Generative OrgansChristine HoNo ratings yet
- Infratemporal Fossa: Dr. Prathyusha PG ENT Narayana Medical College NelloreDocument87 pagesInfratemporal Fossa: Dr. Prathyusha PG ENT Narayana Medical College NelloreSARAVANANNo ratings yet
- Understanding the Pelvis and Pelvic FloorDocument35 pagesUnderstanding the Pelvis and Pelvic FloorAdan ImanNo ratings yet
- Dinding Abdomen PSIKDocument79 pagesDinding Abdomen PSIKSondang DamanikNo ratings yet
- Abdominal Wall Hernia GuideDocument35 pagesAbdominal Wall Hernia GuideMohammad BanisalmanNo ratings yet
- 13 Genital Tract InjuriesDocument100 pages13 Genital Tract InjuriesRana Vandana100% (1)
- Female Perineum and External Genitalia AnatomyDocument23 pagesFemale Perineum and External Genitalia AnatomySyed Irfan Arif100% (1)
- PharynxDocument47 pagesPharynxAchraf RabadiNo ratings yet
- The Anatomy of the Pelvis: Structures and ContentsDocument25 pagesThe Anatomy of the Pelvis: Structures and ContentsFaith ChepoghishoNo ratings yet
- Chapter 8 Neck Skin, Fascia, And Sternocleidomastoid NewDocument64 pagesChapter 8 Neck Skin, Fascia, And Sternocleidomastoid NewMohan PalanimalaiNo ratings yet
- Surgical-ANATOMY OF Anterior Abdominal WallDocument83 pagesSurgical-ANATOMY OF Anterior Abdominal WallSyed Irfan ArifNo ratings yet
- HerniaDocument106 pagesHerniaDr-Mohammad Ali-Fayiz Al TamimiNo ratings yet
- Abdominal wall anatomy and common abdominal incisionsDocument42 pagesAbdominal wall anatomy and common abdominal incisionsSamar AhmadNo ratings yet
- Perineum: Dr. Edi Patmini SS, Spog/Dr. M. Nurhadi Rahman, SpogDocument16 pagesPerineum: Dr. Edi Patmini SS, Spog/Dr. M. Nurhadi Rahman, Spogpuskesmas gebangNo ratings yet
- The PerineumDocument3 pagesThe PerineumSanjay KishoreNo ratings yet
- Abdomen - IntroductionDocument63 pagesAbdomen - IntroductionPriyanka SharmaNo ratings yet
- Publication 3 5662 6381Document25 pagesPublication 3 5662 6381Sunil YadavNo ratings yet
- Pelvis.: Moore, Keith. Clinically Oriented Anatomy. Seventh Edition. Lippincott Williams & Wilkins. Baltimore. 2014Document44 pagesPelvis.: Moore, Keith. Clinically Oriented Anatomy. Seventh Edition. Lippincott Williams & Wilkins. Baltimore. 2014Paola Solarte Chicaiza100% (1)
- Perineum 180922120553 PDFDocument45 pagesPerineum 180922120553 PDFFazle RabbiNo ratings yet
- Triangels of NeckDocument86 pagesTriangels of NeckNayela AkramNo ratings yet
- Rectus Abdominis: Perp by Lect: S Hassn AskariDocument21 pagesRectus Abdominis: Perp by Lect: S Hassn AskariShimmering MoonNo ratings yet
- Abdominal CavityDocument78 pagesAbdominal Cavitytanishapatel1005No ratings yet
- Inguinal Hernias: Trix M. Asuncion M.D. General SurgeryDocument55 pagesInguinal Hernias: Trix M. Asuncion M.D. General Surgeryjitendra magarNo ratings yet
- General AnatomyDocument46 pagesGeneral AnatomyIhab IsmailNo ratings yet
- LG 1 (Half - The Salivary Glands)Document31 pagesLG 1 (Half - The Salivary Glands)allanNo ratings yet
- Deep Cervical FasciaDocument53 pagesDeep Cervical FasciaSyeda AlizaNo ratings yet
- lec 11 - the neckDocument19 pageslec 11 - the neckbf28215No ratings yet
- Abdomen Anatomy and RegionsDocument40 pagesAbdomen Anatomy and RegionsAlex ChagalaNo ratings yet
- Topography Femoral RegionDocument40 pagesTopography Femoral RegionmonaNo ratings yet
- Anatomy - Anterior Triangle of The Neck PDFDocument6 pagesAnatomy - Anterior Triangle of The Neck PDFAngel KimNo ratings yet
- Anterior Abdominal Wall Lecture - Nov2015Document75 pagesAnterior Abdominal Wall Lecture - Nov2015Nithin0% (1)
- Stoma SabiDocument7 pagesStoma SabiSagarRathodNo ratings yet
- Surgical Anatomy of Axilla With LymphaticsDocument15 pagesSurgical Anatomy of Axilla With LymphaticsSagarRathodNo ratings yet
- CASE SCENARIO-labcDocument20 pagesCASE SCENARIO-labcSagarRathodNo ratings yet
- Mirizzi SyndromeDocument2 pagesMirizzi SyndromeSagarRathodNo ratings yet
- Short Case-StnDocument26 pagesShort Case-StnSagarRathodNo ratings yet
- Serum Alb Conc FigureDocument1 pageSerum Alb Conc FigureSagarRathodNo ratings yet
- Sagar Rathod Pratikshit Raghuwanshi DR.D.D Wagh Dr.P.GhardeDocument46 pagesSagar Rathod Pratikshit Raghuwanshi DR.D.D Wagh Dr.P.GhardeSagarRathodNo ratings yet
- Title PageDocument1 pageTitle PageSagarRathodNo ratings yet
- Eqb - Breast: Le DischargeDocument22 pagesEqb - Breast: Le DischargeSagarRathodNo ratings yet
- Rathod Final PosterDocument100 pagesRathod Final PosterSagarRathodNo ratings yet
- Appeal: 2. of of of inDocument3 pagesAppeal: 2. of of of inSagarRathodNo ratings yet
- WelcomeDocument5 pagesWelcomeCatNo ratings yet
- DR Sagar Rathod Drddwagh: Presented by GuideDocument1 pageDR Sagar Rathod Drddwagh: Presented by GuideSagarRathodNo ratings yet
- WelcomeDocument74 pagesWelcomeSagarRathodNo ratings yet
- DR Sagar Rathod Drddwagh: Presented by GuideDocument1 pageDR Sagar Rathod Drddwagh: Presented by GuideSagarRathodNo ratings yet
- DR Sagar Rathod Drddwagh: Presented by GuideDocument1 pageDR Sagar Rathod Drddwagh: Presented by GuideSagarRathodNo ratings yet
- 1-Tetradecene (MATERIAL SAFETY DATA SHEETDocument11 pages1-Tetradecene (MATERIAL SAFETY DATA SHEETkaryokinezNo ratings yet
- Ref 27 Mortalitas Pada Malnutrisi DG AMLDocument9 pagesRef 27 Mortalitas Pada Malnutrisi DG AMLmuarifNo ratings yet
- Management of Gallbladder Polyps - An Optimal Strategy ProposedDocument4 pagesManagement of Gallbladder Polyps - An Optimal Strategy ProposedTANH NGUYENNo ratings yet
- Analytical Exposition TextDocument8 pagesAnalytical Exposition TextMelki RaparNo ratings yet
- Updated 15-04-2022: 4 Year Mbbs GuidelinesDocument84 pagesUpdated 15-04-2022: 4 Year Mbbs GuidelinesUmer RamzanNo ratings yet
- 11 Amazing Benefits of PineapplesDocument9 pages11 Amazing Benefits of PineapplesEirojram MarjorieNo ratings yet
- Emergency Dept Coding 10-07Document37 pagesEmergency Dept Coding 10-07TintinNo ratings yet
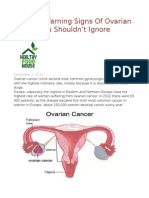
- 10 Early Warning Signs of Ovarian Cancer You Shouldn't IgnoreDocument4 pages10 Early Warning Signs of Ovarian Cancer You Shouldn't IgnoreThavam RatnaNo ratings yet
- Natural Ink From AlugbatiDocument14 pagesNatural Ink From AlugbatiAthena Irish Lastimosa0% (1)
- Helicobacter Pylori: Dr. Chairul SandroDocument40 pagesHelicobacter Pylori: Dr. Chairul SandroAhmedNo ratings yet
- PRULady PDS 2024 1704762736Document6 pagesPRULady PDS 2024 1704762736shirley lee wenNo ratings yet
- Learning Neuroimaging - 100 Essential CasesDocument239 pagesLearning Neuroimaging - 100 Essential CasesLaia Gasull100% (1)
- Deep Learning MamaDocument29 pagesDeep Learning MamaPJ GsNo ratings yet
- Appendix: Joseph Angelo Kiat, MDDocument78 pagesAppendix: Joseph Angelo Kiat, MDMark Angelo PonferradoNo ratings yet
- Uterine Fibroid EmbolizationDocument2 pagesUterine Fibroid EmbolizationWasim ShaheenNo ratings yet
- Amylase and LipaseDocument28 pagesAmylase and LipaseHazel AsperaNo ratings yet
- MSDS Af 11 PDFDocument6 pagesMSDS Af 11 PDFIseng 19No ratings yet
- White Blood Cell WBC Differential PDFDocument15 pagesWhite Blood Cell WBC Differential PDFStefan SuhartoNo ratings yet
- OsteosarcomaDocument25 pagesOsteosarcomaDimas PrasetyoNo ratings yet
- Bowel StatisticsDocument2 pagesBowel StatisticsbillpaparounisNo ratings yet
- IAGI BookletDocument76 pagesIAGI BookletFajar AlamNo ratings yet
- Kjadjk BkjbasjdDocument23 pagesKjadjk BkjbasjdzaenalNo ratings yet
- Rectal Bleeding OverviewDocument7 pagesRectal Bleeding OverviewYanceHanzieNo ratings yet
- Nejmoa1113162 AppendixDocument35 pagesNejmoa1113162 AppendixayuannisahusnaNo ratings yet
- SR 90Document2 pagesSR 90Aeron John GallaNo ratings yet
- CBA - s17 - Class NotesDocument78 pagesCBA - s17 - Class NotesEric YoungNo ratings yet
- Fundamentals of Nursing 100Document6 pagesFundamentals of Nursing 100Succeed ReviewNo ratings yet
- Pediatric Hematology Diseases and ClassificationsDocument48 pagesPediatric Hematology Diseases and ClassificationsZiyan BilqisNo ratings yet
- Causes and Symptoms of Abdominal MassesDocument2 pagesCauses and Symptoms of Abdominal MassesIliriana Bisha TaganiNo ratings yet
- Update On Systemic Therapies For Atopic DermatitisDocument19 pagesUpdate On Systemic Therapies For Atopic Dermatitisrini rossellini utamiNo ratings yet