You might also like
- Classification of Engines & Its ComponentsDocument33 pagesClassification of Engines & Its ComponentsSunil DhankharNo ratings yet
- We Are All So Good at Smiling by Amber McBrideDocument14 pagesWe Are All So Good at Smiling by Amber McBrideMacmillan Kids50% (2)
- Malleolar Fractures - Handout PDFDocument14 pagesMalleolar Fractures - Handout PDFAlin Bratu100% (2)
- Ankle FractureDocument87 pagesAnkle FractureStar Cruise100% (1)
- NexGen Flexion Balancing Instruments Surgical Technique 2897-5967-031-00 Rev1!29!2811 2009 29Document48 pagesNexGen Flexion Balancing Instruments Surgical Technique 2897-5967-031-00 Rev1!29!2811 2009 29flo1987No ratings yet
- Hip Knee Ankle Foot OrthosisDocument44 pagesHip Knee Ankle Foot OrthosisGulzar Ahmad100% (1)
- Pelvic FracturesDocument58 pagesPelvic Fracturesshammasbm100% (10)
- Diaphyseal Fixation Using Long Tapered StemDocument19 pagesDiaphyseal Fixation Using Long Tapered StemPurushotham NalamatiNo ratings yet
- GENIOPLASTYDocument36 pagesGENIOPLASTYJesus MullinsNo ratings yet
- JessDocument20 pagesJessdeepaliarneja67% (3)
- EmotionsDocument18 pagesEmotionsVinod DhanapalNo ratings yet
- Club Foot-Dr J SahooDocument9 pagesClub Foot-Dr J SahooSheel Gupta100% (1)
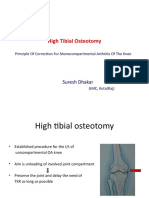
- High Tibial Osteotomy: Suresh DhakarDocument40 pagesHigh Tibial Osteotomy: Suresh DhakarAtul PandeyNo ratings yet
- Proximal Femoral NewDocument34 pagesProximal Femoral NewHimanshu HemantNo ratings yet
- Aaos2007 Hip Knee PDFDocument61 pagesAaos2007 Hip Knee PDFHéctor Pando Sánchez100% (1)
- UntitledDocument213 pagesUntitledSpike SpiguelNo ratings yet
- ORP - Handout - English - Malleolar FracturesDocument15 pagesORP - Handout - English - Malleolar Fracturesadrian1989No ratings yet
- Ankle Distraction ArthroplastyDocument15 pagesAnkle Distraction ArthroplastyJon Hook100% (1)
- Skeletal TractionDocument7 pagesSkeletal TractionAnnalyn Austria100% (2)
- Posterio Lateral Corner Injuries With Varus KneeDocument16 pagesPosterio Lateral Corner Injuries With Varus KneeVignesh WaranNo ratings yet
- OPEN WEDGE Distal Femoral OsteotomyDocument18 pagesOPEN WEDGE Distal Femoral OsteotomyAmr HassanNo ratings yet
- Accessory NavicularDocument24 pagesAccessory NavicularsprapurNo ratings yet
- Presentation 1Document16 pagesPresentation 1Moiz AliNo ratings yet
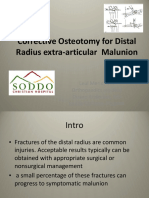
- Distal Radius Osteotomy ComDocument37 pagesDistal Radius Osteotomy ComIskolar MorenoNo ratings yet
- Sacral Fusion & Tarlov Cyst TreatmentDocument28 pagesSacral Fusion & Tarlov Cyst TreatmentMuhammad DickyNo ratings yet
- Total Knee Arthroplasty PrinciplesDocument40 pagesTotal Knee Arthroplasty PrinciplesMitri NassarNo ratings yet
- Primary Hip Arthroplasty Templating On Standard Radiographs A Stepwise ApproachDocument31 pagesPrimary Hip Arthroplasty Templating On Standard Radiographs A Stepwise ApproachMarius Chirila100% (1)
- ClubfootDocument52 pagesClubfootArianto PrabowoNo ratings yet
- High Tibial OsteotomiesDocument24 pagesHigh Tibial OsteotomiesMuhamad Izwan Bin HanafiNo ratings yet
- S-Malunion - Principals and ManagementDocument45 pagesS-Malunion - Principals and ManagementshahnazroeentanmailNo ratings yet
- Surgical Treatment of ClubfootDocument49 pagesSurgical Treatment of Clubfootvishwas dabasNo ratings yet
- General Management For Potts DiseaseDocument2 pagesGeneral Management For Potts Diseaseanreilegarde100% (1)
- PatellaDocument5 pagesPatellaDrNikhil ChandurkarNo ratings yet
- LL AmputationDocument119 pagesLL AmputationMpt SportsNo ratings yet
- Femoral Supracondylar Fractures: Prepared by Dr. Ramzy Sh. ShikhanDocument77 pagesFemoral Supracondylar Fractures: Prepared by Dr. Ramzy Sh. ShikhanRamzi ShukriNo ratings yet
- Spinal Osteotomies PDFDocument3 pagesSpinal Osteotomies PDFbandil deepanshuNo ratings yet
- Developmental Orthopedic Disease - EQDocument33 pagesDevelopmental Orthopedic Disease - EQCaitlinNo ratings yet
- Patellar FractureDocument43 pagesPatellar FractureAkash KoulNo ratings yet
- Limb Reconstruction SystemDocument12 pagesLimb Reconstruction SystemMarcus ChuahNo ratings yet
- Tindak Lanjut Jangka Panjang Hasil Metode Ongley ProlotherapyDocument3 pagesTindak Lanjut Jangka Panjang Hasil Metode Ongley ProlotherapyWindaNo ratings yet
- Tibia ProximalDocument51 pagesTibia Proximalchenth3r3No ratings yet
- реконструкция нижней челюстиDocument8 pagesреконструкция нижней челюстиIrinaBorodulinaNo ratings yet
- Pelvic FracturesDocument58 pagesPelvic FracturesVilasineeAriHaraKumarNo ratings yet
- Inverted L OsteotomyDocument9 pagesInverted L OsteotomyhaneefmdfNo ratings yet
- Soft Tissue Balancing in TKRDocument28 pagesSoft Tissue Balancing in TKRPrathyush PramodNo ratings yet
- RADIOLOGY OF KNEE For StudentDocument70 pagesRADIOLOGY OF KNEE For Studentjamie mutucNo ratings yet
- Solomon 2010Document10 pagesSolomon 2010Roger WatersNo ratings yet
- Dislocation of The Hip (July 2020)Document27 pagesDislocation of The Hip (July 2020)thehexhealthNo ratings yet
- Limb Salvage Surgery in Bone MalignanciesDocument56 pagesLimb Salvage Surgery in Bone MalignanciesKyaw SwaNo ratings yet
- Arvee AnkleDocument50 pagesArvee AnkleDesing RajNo ratings yet
- Journal of Orthopaedic Surgery and ResearchDocument6 pagesJournal of Orthopaedic Surgery and ResearchDewye SartikaNo ratings yet
- Spinal SurgeryDocument19 pagesSpinal SurgerySalomeSibashviliNo ratings yet
- Therapeutic Exercise: Foundation & Techniques: Resource Person: Dr. Rahat Ayub PT SHS.326.Lec.17Document45 pagesTherapeutic Exercise: Foundation & Techniques: Resource Person: Dr. Rahat Ayub PT SHS.326.Lec.17Mustafa ,GhulamNo ratings yet
- 2014 Article 9237Document6 pages2014 Article 9237Mahmoud A KhatabNo ratings yet
- jkhs-21-202 Ko enDocument9 pagesjkhs-21-202 Ko enlaurenNo ratings yet
- Article 5Document10 pagesArticle 5Rangga InktaenNdoek'sNo ratings yet
- Principles of Revision TKA Kelly VinceDocument12 pagesPrinciples of Revision TKA Kelly VincePraharsha100% (1)
- Scapula Fracture Treatment & Management: Author: Thomas P Goss, MD Chief Editor: S Ashfaq Hasan, MDDocument24 pagesScapula Fracture Treatment & Management: Author: Thomas P Goss, MD Chief Editor: S Ashfaq Hasan, MDjohanesNo ratings yet
- Management of Incarcerating Pincer-Type Femoroacetabular Impingement With Hip Arthroscopy - Arthroscopy TechniquesDocument1 pageManagement of Incarcerating Pincer-Type Femoroacetabular Impingement With Hip Arthroscopy - Arthroscopy TechniquesNica ReyesNo ratings yet
- Patellar Fracture: Karla Suzatte M. Dasargo DDC PT - InternDocument43 pagesPatellar Fracture: Karla Suzatte M. Dasargo DDC PT - Internk135dNo ratings yet
- Lower Limb Trauma: Cast Application For Common FracturesDocument58 pagesLower Limb Trauma: Cast Application For Common FracturesdrusmanjamilhcmdNo ratings yet
- Orthosis and ProsthesisDocument25 pagesOrthosis and Prosthesissanika pradhanNo ratings yet
- Traditional Surgical TreatmentDocument6 pagesTraditional Surgical TreatmentNadya Febriama NakhruddinNo ratings yet
- Posterior Crossbite in Primary and Mixed Dentition - Etiology and Management PedoDocument41 pagesPosterior Crossbite in Primary and Mixed Dentition - Etiology and Management PedoFourthMolar.comNo ratings yet
- Decrease in Paco2 With Prone Position Is Predictive of Improved Outcome in Acute Respiratory Distress SyndromeDocument7 pagesDecrease in Paco2 With Prone Position Is Predictive of Improved Outcome in Acute Respiratory Distress SyndromedarwigNo ratings yet
- Molecular Basis of InheritanceDocument37 pagesMolecular Basis of Inheritancechristopher lopezNo ratings yet
- Cul5a - Lecture - Week 9 - Singaporean Cuisine PDFDocument14 pagesCul5a - Lecture - Week 9 - Singaporean Cuisine PDFJJ GRNo ratings yet
- Consumer Forum JudgmentDocument19 pagesConsumer Forum JudgmentLatest Laws TeamNo ratings yet
- FIN242 Chapter Summary 6Document3 pagesFIN242 Chapter Summary 6Yan ChingNo ratings yet
- Chest X-Ray The BasicsDocument12 pagesChest X-Ray The BasicshefaesvaNo ratings yet
- Vacuum Circuit Breaker CatalogueDocument11 pagesVacuum Circuit Breaker Cataloguedabs_orangejuice0% (1)
- Nouvelle France Industrielle EnglishDocument76 pagesNouvelle France Industrielle EnglishasdasdNo ratings yet
- Chapter 1: The Principle of NMR: Some RemindersDocument51 pagesChapter 1: The Principle of NMR: Some RemindersAkino AskNo ratings yet
- B.tech ProjectDocument7 pagesB.tech ProjectSimaab AmirNo ratings yet
- Severe Acute Malnutrition: Facility-Based Management of Children WithDocument176 pagesSevere Acute Malnutrition: Facility-Based Management of Children WithNikitha RafeekNo ratings yet
- Hedging QuestionsDocument6 pagesHedging QuestionsAmeya LonkarNo ratings yet
- Research-2 SynthesisDocument11 pagesResearch-2 SynthesisJesusValenciaNo ratings yet
- Reaction To EJKDocument9 pagesReaction To EJKKevin DawangNo ratings yet
- Aircol HC 7, HC 10Document2 pagesAircol HC 7, HC 10Vladislav TrempoletsNo ratings yet
- Chapter 4 & 5Document12 pagesChapter 4 & 5endalkachewNo ratings yet
- Times Leader 06-04-2013Document32 pagesTimes Leader 06-04-2013The Times LeaderNo ratings yet
- D FTP Payslip 00040502 04 2023 PDFDocument1 pageD FTP Payslip 00040502 04 2023 PDFmuhammed basil kmNo ratings yet
- (Joe Jonas) : "Gotta Find You"Document8 pages(Joe Jonas) : "Gotta Find You"Erpin HabibahNo ratings yet
- LGDocument9 pagesLGSandeep SinglaNo ratings yet
- Gsa PPDocument15 pagesGsa PPSheikh Sahil MobinNo ratings yet
- Virgin Coconut OilDocument3 pagesVirgin Coconut OilEd CasasNo ratings yet
- Kirana Case Study - Final222Document15 pagesKirana Case Study - Final222Aseem Jain0% (1)
- Event Safety Check List: Group NameDocument12 pagesEvent Safety Check List: Group NameUs Cosplay SpecialistNo ratings yet
- Going Concern ChecklistDocument1 pageGoing Concern Checklisttunlinoo.067433No ratings yet