You might also like
- California Hawking Club Test GuideDocument128 pagesCalifornia Hawking Club Test Guidegonnaboy100% (13)
- Microbe Mission Cheat SheetDocument5 pagesMicrobe Mission Cheat Sheetgangakolli100% (3)
- FalconryDocument25 pagesFalconryDragonMistressNo ratings yet
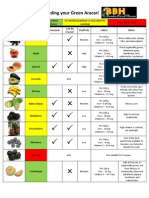
- Produce Guide For Feeding Your Green AracariDocument5 pagesProduce Guide For Feeding Your Green AracariaracariNo ratings yet
- Reptile Pathology - Necropsy TechniquesDocument70 pagesReptile Pathology - Necropsy TechniquesJustine Paola Delos SantosNo ratings yet
- AVIAN-Calculating The Required Volume of Avian Nutritional ProductsDocument2 pagesAVIAN-Calculating The Required Volume of Avian Nutritional Productstaner_soysurenNo ratings yet
- Novice FalconryDocument87 pagesNovice Falconryx13x13100% (1)
- Avian Medicine PDFDocument1,384 pagesAvian Medicine PDFCamila Dergam100% (5)
- Scarlet Macaw DietDocument8 pagesScarlet Macaw DietgabrielwerneckNo ratings yet
- Apprenticeship GuideDocument29 pagesApprenticeship GuideRotiseria La Flamme100% (2)
- Caring For Injured Reptiles2004Document40 pagesCaring For Injured Reptiles2004SujayJainNo ratings yet
- 2003 Avian Care Manual PDFDocument132 pages2003 Avian Care Manual PDFRonald ChavezNo ratings yet
- Cilinical Examination of Sheep& GoatDocument23 pagesCilinical Examination of Sheep& GoatTAMIL71% (7)
- PW Book SampleDocument17 pagesPW Book SampleNina Sapphire100% (1)
- DocxDocument4 pagesDocxFarah FarahNo ratings yet
- Khan USMLE Pearls MicroDocument8 pagesKhan USMLE Pearls Microlourdesfercab75% (4)
- Poultry diseases: Causes, symptoms and treatment, with notes on post-mortem examinationsFrom EverandPoultry diseases: Causes, symptoms and treatment, with notes on post-mortem examinationsNo ratings yet
- Raptor ManualDocument75 pagesRaptor ManualCarlos Juan Martínez Pámanes100% (1)
- Raptor Nutrition enDocument39 pagesRaptor Nutrition enMark AbellaNo ratings yet
- Falconry Information ChecklistDocument5 pagesFalconry Information Checklisttoha putraNo ratings yet
- Falconry TermsDocument4 pagesFalconry Termsgonnaboy100% (1)
- Practical Raptor Nutrition Neil Forbes PDFDocument9 pagesPractical Raptor Nutrition Neil Forbes PDFWisnu JuliastitoNo ratings yet
- Practical Falconry PDFDocument106 pagesPractical Falconry PDFMichael Lennon de Moura100% (1)
- Falcon ApprenticeDocument3 pagesFalcon ApprenticeState of UtahNo ratings yet
- Falconry Guide - Public Edition (SM)Document32 pagesFalconry Guide - Public Edition (SM)Agung Satriya Wibowo100% (2)
- EXOTİC-Raptor Medicine, Basic Principles and Noninfectious ConditionsDocument9 pagesEXOTİC-Raptor Medicine, Basic Principles and Noninfectious Conditionstaner_soysuren100% (1)
- Haginbalds Arte of Medieval FaulconryDocument23 pagesHaginbalds Arte of Medieval FaulconryimmortalskyNo ratings yet
- Emergency RaptorsDocument24 pagesEmergency RaptorsjudithNo ratings yet
- Falconry: Perigrinus) Are Some of The More Commonly Used Birds of Prey. The Practice ofDocument19 pagesFalconry: Perigrinus) Are Some of The More Commonly Used Birds of Prey. The Practice ofLeonardo Miranda CollantesNo ratings yet
- CageDocument10 pagesCageYannick PrattNo ratings yet
- Feather Destructive BehaviorDocument20 pagesFeather Destructive BehaviorAnh-MinhNo ratings yet
- Falc GuideDocument28 pagesFalc GuideMark AbellaNo ratings yet
- Hints on the Management of Hawks and Practical FalconryFrom EverandHints on the Management of Hawks and Practical FalconryNo ratings yet
- ParrotsDocument304 pagesParrotstobiasaxo5653No ratings yet
- JOSEPH 2006 Raptor Medicine - An Approach To Wild, Falconry, and Educational Birds of PreyDocument25 pagesJOSEPH 2006 Raptor Medicine - An Approach To Wild, Falconry, and Educational Birds of PreyigorvetNo ratings yet
- Basic Avian AnatomyDocument10 pagesBasic Avian AnatomyHarry MontriNo ratings yet
- Falconry - Celebrating A Living HeritageDocument11 pagesFalconry - Celebrating A Living HeritagebooksarabiaNo ratings yet
- Hawks and OwlsDocument10 pagesHawks and Owlsaccipiter67100% (4)
- Parrot Breeding and Keeping:: The Impact of Capture and CaptivityDocument66 pagesParrot Breeding and Keeping:: The Impact of Capture and CaptivityOjeda BorisNo ratings yet
- WoF LoresDocument44 pagesWoF LoresSolentDesignNo ratings yet
- ExoticDocument252 pagesExoticVirhuezKSNo ratings yet
- Reptile Nutritional DiseasesDocument9 pagesReptile Nutritional DiseasesDiah PiastutiNo ratings yet
- Avian PathologyDocument48 pagesAvian PathologyEric Cheah100% (1)
- Avian Hematology and Related DisordersDocument22 pagesAvian Hematology and Related DisordersIban Hernández100% (1)
- Exotic Birds NutritionDocument21 pagesExotic Birds NutritiongabrielwerneckNo ratings yet
- Avian HematologyDocument16 pagesAvian HematologyNatalie Woodward100% (1)
- Home Reference Manual - FalconryDocument50 pagesHome Reference Manual - FalconryOliver Tomlinson100% (1)
- HedgehogDocument9 pagesHedgehogRalph Laurence GulfoNo ratings yet
- Anesthesia of Pet BirdsDocument12 pagesAnesthesia of Pet Birdstrung5848No ratings yet
- Caring for a Canary - Answers to Frequently Asked Questions about Caring for your Canary - With Sections on Bird Choice, Training, Aviaries, Common Ailments and CuresFrom EverandCaring for a Canary - Answers to Frequently Asked Questions about Caring for your Canary - With Sections on Bird Choice, Training, Aviaries, Common Ailments and CuresNo ratings yet
- Mammalian Diseases Found in Captivity FinalDocument45 pagesMammalian Diseases Found in Captivity Finalapi-250146149No ratings yet
- Interpretation of The Reptile Blood ProfileDocument8 pagesInterpretation of The Reptile Blood ProfileAndre NgoNo ratings yet
- Manual of Exotic Pet Practice - HedgehogDocument23 pagesManual of Exotic Pet Practice - HedgehogNoriane RhouyNo ratings yet
- Manul of Avian DiseaseDocument305 pagesManul of Avian Diseasenasih hamadNo ratings yet
- Veterinary AnatomyDocument49 pagesVeterinary AnatomyAdeel SarfrazNo ratings yet
- Parasitic Diseases of The Fish 2Document35 pagesParasitic Diseases of The Fish 2Saraturituri100% (2)
- Veterinary ImmunologyDocument20 pagesVeterinary ImmunologyJennifer Bumagat-BermudezNo ratings yet
- Red Gut Pow-Wow GroundsDocument2 pagesRed Gut Pow-Wow GroundspegspirateNo ratings yet
- Eastern Equine Encephalitis (EEE) Stats For MassachusettsDocument3 pagesEastern Equine Encephalitis (EEE) Stats For MassachusettsGarrett QuinnNo ratings yet
- OSH 310 Readings Enviromental HealthDocument134 pagesOSH 310 Readings Enviromental Healthizzyklin23No ratings yet
- Emerging and Less Common Viral Encephalitides - Chapter 91Document34 pagesEmerging and Less Common Viral Encephalitides - Chapter 91Victro ChongNo ratings yet
- Molecular Diagnostics of Infectious Diseases, 2010, PGDocument207 pagesMolecular Diagnostics of Infectious Diseases, 2010, PGrieza_husein100% (2)
- 10clinical VignettespdfDocument71 pages10clinical VignettespdfKerin Ardy100% (1)
- SAS 08 - MLS 054 - Epidemiology, Epidemiological MeasurementsDocument14 pagesSAS 08 - MLS 054 - Epidemiology, Epidemiological MeasurementsNaomi Yazzie CabusNo ratings yet
- West Nile Disease (Author) (Institution)Document7 pagesWest Nile Disease (Author) (Institution)Eman MunirNo ratings yet
- CodeDocument88 pagesCodeGLADYSNo ratings yet
- Emerging Vector-Borne Diseases: Sioux Falls, South DakotaDocument7 pagesEmerging Vector-Borne Diseases: Sioux Falls, South DakotaHakiki Oksan SaputraNo ratings yet
- Times Leader 08-13-2013Document36 pagesTimes Leader 08-13-2013The Times LeaderNo ratings yet
- Foundations in Microbiology: TalaroDocument76 pagesFoundations in Microbiology: Talaromertx013No ratings yet
- 02 107學測英文 定稿Document11 pages02 107學測英文 定稿罐頭TNTNo ratings yet
- Karen Radner, “The Assyrian king and his scholars: The Syro-Anatolian and the Egyptian Schools.” In M. Luukko/S. Svärd/R. Mattila (ed.), Of God(s), Trees, Kings, and Scholars: Neo-Assyrian and Related Studies in Honour of Simo Parpola. Studia Orientalia 106 (Helsinki 2009) 221-238.Document85 pagesKaren Radner, “The Assyrian king and his scholars: The Syro-Anatolian and the Egyptian Schools.” In M. Luukko/S. Svärd/R. Mattila (ed.), Of God(s), Trees, Kings, and Scholars: Neo-Assyrian and Related Studies in Honour of Simo Parpola. Studia Orientalia 106 (Helsinki 2009) 221-238.nerakrendarNo ratings yet
- Diseases Caused by Bacteria, Viruses, and Nematodes and OthersDocument748 pagesDiseases Caused by Bacteria, Viruses, and Nematodes and OthersNeha UpadhyayNo ratings yet
- Cordia Viral MeningitisDocument7 pagesCordia Viral MeningitisAyuagung Chandra Maha DewiNo ratings yet
- COMMUNICABLE DISEASES - Power Point PDFDocument143 pagesCOMMUNICABLE DISEASES - Power Point PDFGel Marie LobatonNo ratings yet
- Times Leader 08-14-2011Document93 pagesTimes Leader 08-14-2011The Times LeaderNo ratings yet
- Texas West Nile Outbreak Most Deadly in The NationDocument11 pagesTexas West Nile Outbreak Most Deadly in The NationmfadegreeNo ratings yet
- 08-23-12 EditionDocument36 pages08-23-12 EditionSan Mateo Daily JournalNo ratings yet
- The Lagonian - October 2012Document16 pagesThe Lagonian - October 2012TheLagonianNo ratings yet
- Dr. Jane P. Messina, March 2014Document5 pagesDr. Jane P. Messina, March 2014Janey MessinaNo ratings yet
- EncephalitisDocument40 pagesEncephalitisjayalakshmiNo ratings yet
- August 19, 2016Document16 pagesAugust 19, 2016Anonymous KMKk9Msn5No ratings yet
- West Nile Virus Homeopathy HandoutDocument3 pagesWest Nile Virus Homeopathy HandoutRoger Auge100% (1)
- ZikaDocument11 pagesZikasamjaisheel100% (1)