You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Completely Reverse Heart Disease With This Revolutionary TreatmentDocument8 pagesCompletely Reverse Heart Disease With This Revolutionary TreatmentSamee's Music100% (3)
- Enteral NutritionDocument73 pagesEnteral NutritionYosep Sutandar100% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- General Medicine MCQDocument73 pagesGeneral Medicine MCQkhalida shaik begumNo ratings yet
- The 29 Pulses in Chinese Medicine (TCM) Pulse DiagnosisDocument7 pagesThe 29 Pulses in Chinese Medicine (TCM) Pulse DiagnosisPrakash Aradhya RNo ratings yet
- Step by Step Pediatric Echocardiography PDFDocument141 pagesStep by Step Pediatric Echocardiography PDFDiana_anca6100% (1)
- Pacemaker Invasive Cardiac PacingDocument57 pagesPacemaker Invasive Cardiac PacingAhmad Khalil Ahmad Al-SadiNo ratings yet
- Topic 7 Cardiorespiratory Adaptations To TrainingDocument26 pagesTopic 7 Cardiorespiratory Adaptations To TrainingCikguAmelia100% (1)
- Spesifikasi Philips Incisive CT 128 PremiumDocument2 pagesSpesifikasi Philips Incisive CT 128 PremiumvitapabloNo ratings yet
- PT3 Science Chapter 19 Blood Circulation and TransportDocument8 pagesPT3 Science Chapter 19 Blood Circulation and TransportSpike ChingyenNo ratings yet
- OBG DrugsDocument85 pagesOBG Drugsvivekkumar05468No ratings yet
- Biology Syllabus Forms 3-4Document88 pagesBiology Syllabus Forms 3-4Malack Chagwa100% (6)
- The Harvard Step Test PDFDocument32 pagesThe Harvard Step Test PDFRajalakshmiNo ratings yet
- PIIS000293781502102XDocument1 pagePIIS000293781502102XYosep SutandarNo ratings yet
- Routine Firsttrimester Ultrasound Screening Using A Standardized Anatomical ProtocolDocument15 pagesRoutine Firsttrimester Ultrasound Screening Using A Standardized Anatomical ProtocolYosep SutandarNo ratings yet
- Ferra RettiDocument51 pagesFerra RettiYosep SutandarNo ratings yet
- Physiology of Amniotic Fluid Volume RegulationDocument8 pagesPhysiology of Amniotic Fluid Volume RegulationYosep SutandarNo ratings yet
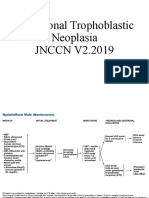
- Gestational Trophoblastic NeoplasiaDocument14 pagesGestational Trophoblastic NeoplasiaYosep SutandarNo ratings yet
- Changes in The Sexual Function During Pregnancy: Aim. MethodsDocument10 pagesChanges in The Sexual Function During Pregnancy: Aim. MethodsYosep SutandarNo ratings yet
- Mao2014 Article ImagingOfPelvicLymphNodesDocument13 pagesMao2014 Article ImagingOfPelvicLymphNodesYosep SutandarNo ratings yet
- Ovarian Reserve Testing: A User's Guide: Expert ReviewsDocument12 pagesOvarian Reserve Testing: A User's Guide: Expert ReviewsYosep SutandarNo ratings yet
- Acog Committee Opinion: Dysmenorrhea and Endometriosis in The AdolescentDocument10 pagesAcog Committee Opinion: Dysmenorrhea and Endometriosis in The AdolescentYosep SutandarNo ratings yet
- Pi Is 0884217517304100Document3 pagesPi Is 0884217517304100Yosep SutandarNo ratings yet
- Eng - PDF JsessionidDocument34 pagesEng - PDF JsessionidYosep SutandarNo ratings yet
- Practice Bullet In: Emergency ContraceptionDocument11 pagesPractice Bullet In: Emergency ContraceptionYosep SutandarNo ratings yet
- Clue CellsDocument10 pagesClue CellsYosep SutandarNo ratings yet
- Compare Atenolol Vs PropranololDocument5 pagesCompare Atenolol Vs Propranololpooja lokhandeNo ratings yet
- Case Report ASMIHA 2022Document1 pageCase Report ASMIHA 2022Ghina NinditasariNo ratings yet
- Adrenaline PDFDocument1 pageAdrenaline PDFPilaRocio YHNo ratings yet
- Animal Physiology and Anatomy Practical ExamDocument15 pagesAnimal Physiology and Anatomy Practical ExamFake GamerNo ratings yet
- Heart Failure Cheat SheetDocument2 pagesHeart Failure Cheat SheetNicolle GaleNo ratings yet
- Chapter Three-Occupational Anatomy and PhysiologyDocument29 pagesChapter Three-Occupational Anatomy and PhysiologyNkuuwe EdmundNo ratings yet
- Mitral Valve Repair TrialDocument11 pagesMitral Valve Repair TrialAnawhatNo ratings yet
- GC Approved Curriculum PDFDocument282 pagesGC Approved Curriculum PDFSohailNo ratings yet
- Comparative Study of Serum and Biliary Lipid Profile in Libyan Gallstone PatientsDocument54 pagesComparative Study of Serum and Biliary Lipid Profile in Libyan Gallstone PatientsJagannadha Rao PeelaNo ratings yet
- Sorted Feedback TopicwiseDocument55 pagesSorted Feedback TopicwiseLokesh BakshiNo ratings yet
- All About Bradycardia and Conduction DisturbanceDocument40 pagesAll About Bradycardia and Conduction DisturbancenureNo ratings yet
- Circulatory and Respiratory Unit TestDocument5 pagesCirculatory and Respiratory Unit TestfojanpriNo ratings yet
- BP Pump 2Document3 pagesBP Pump 2sirtaeNo ratings yet
- Pathology of Myxomatous Mitral Valve Disease in The Dog: Philip R. Fox, DVM, MSCDocument24 pagesPathology of Myxomatous Mitral Valve Disease in The Dog: Philip R. Fox, DVM, MSCKrlÖz Ändrz Hërëdîa ÖpzNo ratings yet
- Science QPDocument67 pagesScience QPVENKATESH YNo ratings yet
- Review of Systems: Skin MusculoskeletalDocument2 pagesReview of Systems: Skin MusculoskeletalAngelino HernandezNo ratings yet
- Anti Anginal DrugsDocument109 pagesAnti Anginal Drugsvingul2006No ratings yet
- Danielle Karen Widjaja 22010113130175 Lap - Kti Bab2Document2 pagesDanielle Karen Widjaja 22010113130175 Lap - Kti Bab2Mamanya Fadhil HaniNo ratings yet
- Circulationaha 108 191098Document9 pagesCirculationaha 108 191098rajesh kumarNo ratings yet