You might also like
- MCQs in Clinical BiochemistryDocument15 pagesMCQs in Clinical Biochemistrysidharta_chatterjee79% (14)
- Biochemistry II End of Semester Exam QuestionsDocument6 pagesBiochemistry II End of Semester Exam Questionsnima00No ratings yet
- MCQS BiochemistryDocument3 pagesMCQS Biochemistrynasibdin100% (3)
- Quick Review of Biochemistry For Undergraduates (Questions and Answers) PDFDocument312 pagesQuick Review of Biochemistry For Undergraduates (Questions and Answers) PDFNalini Rooplal100% (4)
- Hewer's Textbook of Histology for Medical StudentsFrom EverandHewer's Textbook of Histology for Medical StudentsRating: 5 out of 5 stars5/5 (2)
- Summary Judgments in Texas PDFDocument140 pagesSummary Judgments in Texas PDFS TNo ratings yet
- Endicrine MCQ-QuestionsDocument4 pagesEndicrine MCQ-QuestionsThe White Army100% (1)
- Lippincott BiochemistryDocument209 pagesLippincott BiochemistryAhmad Samir57% (7)
- Feed Fast CycleDocument19 pagesFeed Fast Cyclesaraimran54100% (2)
- Biochemistry 1001 V J Temple PDFDocument12 pagesBiochemistry 1001 V J Temple PDFAmjad Ali50% (2)
- Clinical Biochemistry IIDocument13 pagesClinical Biochemistry IIsidharta_chatterjeeNo ratings yet
- Neurology Board ReviewDocument16 pagesNeurology Board ReviewNabeel Kouka, MD, DO, MBA, MPH67% (3)
- RF Planning and OptimizationDocument5 pagesRF Planning and OptimizationAviral AgarwalNo ratings yet
- BS en 13481-2-2012 (2014)Document26 pagesBS en 13481-2-2012 (2014)Thanh Nghiem80% (5)
- Viva Voce Orals in BiochemistryDocument245 pagesViva Voce Orals in Biochemistryprimadon0375No ratings yet
- Viva Voce Orals in BiochemistryDocument25 pagesViva Voce Orals in Biochemistrydr.majumder7102100% (11)
- Biochemistry VivaDocument8 pagesBiochemistry VivaNazia WasimNo ratings yet
- Biochemistry MCQDocument24 pagesBiochemistry MCQpoojaNo ratings yet
- Biochemistry One LinersDocument11 pagesBiochemistry One Linerssandeep MahapatraNo ratings yet
- Clinical Biochemistry IDocument18 pagesClinical Biochemistry Isidharta_chatterjee100% (1)
- Clinical Biochemistry Practical IDocument73 pagesClinical Biochemistry Practical Isama_omery100% (1)
- Clinical Biochemistry Exam-2 andDocument1 pageClinical Biochemistry Exam-2 andMina MansourNo ratings yet
- Nucleotides McqsDocument8 pagesNucleotides McqsSp Ppv0% (1)
- Biochemistry MCQsDocument5 pagesBiochemistry MCQsKanchan KarmakarNo ratings yet
- Biochemistry Basic Science MCQsDocument26 pagesBiochemistry Basic Science MCQsSidharta Chatterjee50% (2)
- Biochemistry MCQ Books FreeDocument2 pagesBiochemistry MCQ Books FreeMajid Khan100% (1)
- Testbank MetabolismDocument11 pagesTestbank MetabolismRiky Ikhwan50% (2)
- BRS BiochemistryDocument345 pagesBRS Biochemistrysxymd321100% (1)
- Practical PhysiologyDocument436 pagesPractical Physiologyaastha212002100% (1)
- Mcqs Related To BiochemistryDocument8 pagesMcqs Related To BiochemistryRoha AsjadNo ratings yet
- Biochemistry MCQ IIDocument18 pagesBiochemistry MCQ IISidharta Chatterjee100% (2)
- Clinical BiochemistryDocument211 pagesClinical Biochemistrymyat25100% (1)
- BCH MCQs1Document304 pagesBCH MCQs1moxdegr8100% (1)
- Biochemistry Saeed Oraby Part 3Document276 pagesBiochemistry Saeed Oraby Part 3أسہہآمہهہ شہعہلآن100% (3)
- 5000 MCQs in BiochemistryDocument301 pages5000 MCQs in BiochemistryZia Ashraf Chaudhary94% (17)
- Final Biochemistry MCQDocument29 pagesFinal Biochemistry MCQsaraNo ratings yet
- 1 Red Blood Cells Anemia and PolycythemiaDocument43 pages1 Red Blood Cells Anemia and PolycythemiaGeevee Naganag VentulaNo ratings yet
- Mock Exam PhysiologyDocument150 pagesMock Exam Physiologyvnair112100% (1)
- Metabolism Lippincott's Q&ADocument86 pagesMetabolism Lippincott's Q&Alina amjadNo ratings yet
- Chemistry of Lipids: DR Rakesh Sharma, Professor North DMC Medical College, DelhiDocument50 pagesChemistry of Lipids: DR Rakesh Sharma, Professor North DMC Medical College, DelhiProfessor Rakesh Sharma Biochemistry Lectures100% (2)
- Lehninger Multiple ChoiceDocument13 pagesLehninger Multiple ChoiceHugo DuarteNo ratings yet
- Glycolysis, Gluconeogenesis, Pentose Phosphate PathwayDocument2 pagesGlycolysis, Gluconeogenesis, Pentose Phosphate PathwayDavid Miguel Landry100% (2)
- Biochemistry of Blood 1Document35 pagesBiochemistry of Blood 1AMEER ALSAABRAWINo ratings yet
- Clinical Biochemistry Past PaperDocument7 pagesClinical Biochemistry Past PaperAnonymous WkIfo0P100% (1)
- Metabolism MCQ ADocument0 pagesMetabolism MCQ ASurajit BhattacharjeeNo ratings yet
- BiochemistryDocument65 pagesBiochemistryRafique CNo ratings yet
- Biochemistry-MD21 and DD21-year 2, Semester 1 Lecturer: Bun SeangkhinDocument13 pagesBiochemistry-MD21 and DD21-year 2, Semester 1 Lecturer: Bun SeangkhinVathana SorNo ratings yet
- Proteins McqsDocument3 pagesProteins McqsAG Khan100% (1)
- Ganong - Physiology Self - Assessment Questions - 03Document46 pagesGanong - Physiology Self - Assessment Questions - 03Anonymous 4txA8N8et100% (3)
- Protein and Amino Acid MetabolismDocument52 pagesProtein and Amino Acid MetabolismRisky OpponentNo ratings yet
- Protein Structure and Folding LectureDocument18 pagesProtein Structure and Folding Lecturemaryscribd241No ratings yet
- Metabolism of Vitamins and Trace Elements: Comprehensive BiochemistryFrom EverandMetabolism of Vitamins and Trace Elements: Comprehensive BiochemistryNo ratings yet
- A Text - Book of Histology: Descriptive and Practical. For the Use of StudentsFrom EverandA Text - Book of Histology: Descriptive and Practical. For the Use of StudentsNo ratings yet
- BIOCHEMISTRY, CELL AND MOLECULAR BIOLOGY: Passbooks Study GuideFrom EverandBIOCHEMISTRY, CELL AND MOLECULAR BIOLOGY: Passbooks Study GuideNo ratings yet
- Channels, Carriers, and Pumps: An Introduction to Membrane TransportFrom EverandChannels, Carriers, and Pumps: An Introduction to Membrane TransportNo ratings yet
- Cells and Tissues: An Introduction to Histology and Cell BiologyFrom EverandCells and Tissues: An Introduction to Histology and Cell BiologyRating: 4 out of 5 stars4/5 (3)
- The Kidney: Morphology, Biochemistry, PhysiologyFrom EverandThe Kidney: Morphology, Biochemistry, PhysiologyCharles RouillerNo ratings yet
- Tutti FruttiDocument10 pagesTutti FruttishadapaaakNo ratings yet
- Medical Syndromes Internal Medicine NoteDocument4 pagesMedical Syndromes Internal Medicine NoteFranspol100% (1)
- Neuro TestDocument9 pagesNeuro TestHanung Merahbara100% (1)
- Cranial Nerves Anatomy Review NoteDocument5 pagesCranial Nerves Anatomy Review NoteOlu FasanyaNo ratings yet
- Cardiac TestsDocument6 pagesCardiac TestsRobert DowneyNo ratings yet
- Usmle Comlex Most CommonDocument3 pagesUsmle Comlex Most Commonsooryarao100% (1)
- Intertextuality EssayDocument2 pagesIntertextuality EssaySama AlkouniNo ratings yet
- Lidar Solutions in ArcGIS 10.0Document51 pagesLidar Solutions in ArcGIS 10.0Wanly PereiraNo ratings yet
- A New InterpretationDocument6 pagesA New InterpretationAlexandros KastanakisNo ratings yet
- King Lear Plot SummaryDocument3 pagesKing Lear Plot SummaryJasvinder Singh100% (2)
- Examples of Electrocyclic ReactionsDocument14 pagesExamples of Electrocyclic ReactionsAn TruongNo ratings yet
- Lecture 1Document87 pagesLecture 1Raymer OclaritNo ratings yet
- 0580 m17 QP 22Document12 pages0580 m17 QP 22Sameer Abu MunsharNo ratings yet
- DR B R Ambedkar and Making of The Constitution A Case Study of Indian FederalismDocument13 pagesDR B R Ambedkar and Making of The Constitution A Case Study of Indian FederalismDanexNo ratings yet
- Arterial Blood Gas InterpretationDocument74 pagesArterial Blood Gas InterpretationSarina AsuncionNo ratings yet
- Vienna Convention On The Law of Treaties PDFDocument104 pagesVienna Convention On The Law of Treaties PDFAbbie KwanNo ratings yet
- Weight Loss SpellsDocument10 pagesWeight Loss SpellsAnna Deniz Luna100% (2)
- Organizational Behavior I - Chapter 1Document6 pagesOrganizational Behavior I - Chapter 1Azfar JavaidNo ratings yet
- The DARK Side of Total Synthesis: Strategies and Tactics in Psychoactive Drug ProductionDocument24 pagesThe DARK Side of Total Synthesis: Strategies and Tactics in Psychoactive Drug Production943909No ratings yet
- Old Man and The SeaDocument22 pagesOld Man and The Seaapi-268644570No ratings yet
- Math10 Q3 Module10 Probalityofcompoundevents Lessonproper v2Document82 pagesMath10 Q3 Module10 Probalityofcompoundevents Lessonproper v2Anabel AlarconNo ratings yet
- Hamari Adhuri Kahani Chords - Arijit Singh - GUITAR CHORD WORLDDocument2 pagesHamari Adhuri Kahani Chords - Arijit Singh - GUITAR CHORD WORLDabhi100% (1)
- EntrepreneurshipDocument5 pagesEntrepreneurshipMahabub RabbaniNo ratings yet
- Grade - 8 - Mathematics - Week04 - Algebraic Fractions and Formulae - Check in 4Document18 pagesGrade - 8 - Mathematics - Week04 - Algebraic Fractions and Formulae - Check in 4Ignatia Fransiska Sari IndahNo ratings yet
- Brinas V People G.R. No. 254005Document9 pagesBrinas V People G.R. No. 254005weddanever.cornelNo ratings yet
- Meningitis and Encephalitis: PGI Roddame Angelo ErispeDocument100 pagesMeningitis and Encephalitis: PGI Roddame Angelo ErispeAngelo ErispeNo ratings yet
- UDIPDocument156 pagesUDIPVaishnavi JayakumarNo ratings yet
- Consumer Behaviour-Solomon-Ch 1Document31 pagesConsumer Behaviour-Solomon-Ch 1muhammad fadli100% (1)
- Ge10 Group 2Document63 pagesGe10 Group 2Callisto AstraeaNo ratings yet
- Questions & Answers Chapter - 7 Set 1Document6 pagesQuestions & Answers Chapter - 7 Set 1FaridOrahaNo ratings yet
- Chapter 3: Mathematical Analysis of Material Balance Equations and Process Flow SheetsDocument6 pagesChapter 3: Mathematical Analysis of Material Balance Equations and Process Flow Sheetsgoogley71No ratings yet
- Oil Spill Response Contingency Plan For Mumbai & JNPT HarbourDocument179 pagesOil Spill Response Contingency Plan For Mumbai & JNPT HarbourVaishnavi Jayakumar100% (1)
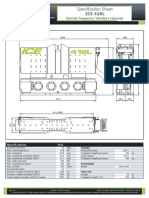
- Specification Sheet: ICE 416LDocument2 pagesSpecification Sheet: ICE 416LBapusaheb GuthaleNo ratings yet